Fatal progressive right heart failure in a pancreatic cancer patient
- Affiliations
-
- 1Department of Cardiology, Wonkwang University Hospital, Iksan, Korea
- KMID: 2501419
- DOI: http://doi.org/10.12701/yujm.2019.00332
Abstract
- Pulmonary tumor thrombotic microangiopathy (PTTM) is a rare but fatal complication of cancer and causes pulmonary hypertension and acute/subacute right heart failure. PTTM is most commonly associated with gastric cancer and more rarely associated with pancreatic cancer. We report a case of progressive right heart failure associated with clinically diagnosed pancreatic cancer, suggesting PTTM.
Keyword
Figure
-
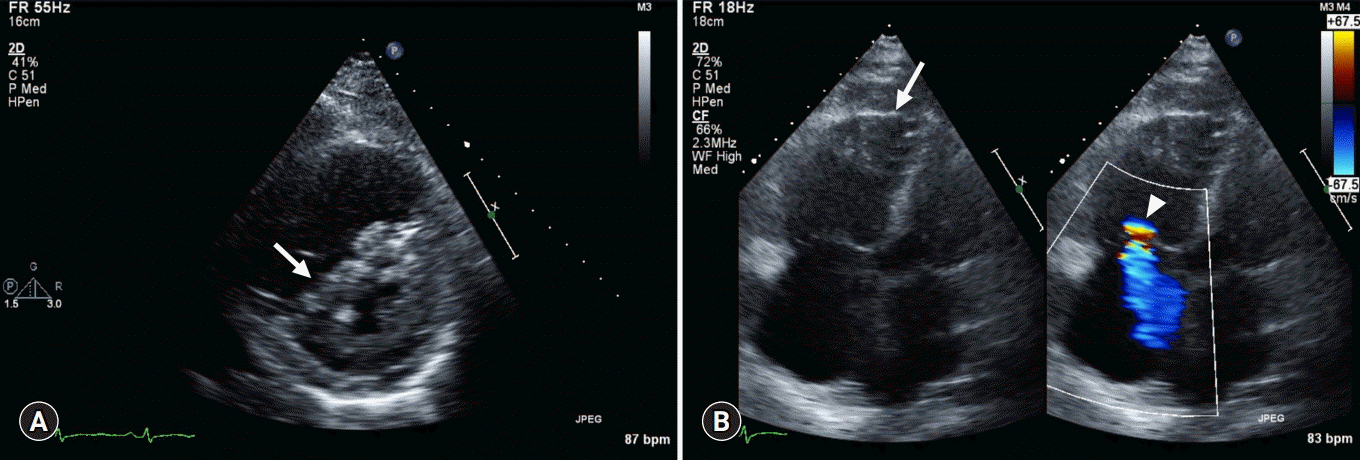
Fig. 1. Transthoracic echocardiography. (A) Parasternal short-axis view shows LV systolic septal flattening (arrow) with RV enlargement. (B) Apical 4 chamber view with color Doppler of the tricuspid valve shows RV enlargement (arrow) and moderate tricuspid regurgitation (arrowhead). LV, left ventricle; RV, right ventricle.

Fig. 2. Contrast-enhanced CT. (A) Chest CT (lung window) with centrilobular nodules with “tree-in-bud” sign (arrows). (B) Chest CT (mediastinal window) with pleural-enhancing nodules (arrowhead). (C) Abdominopelvic CT show upstream pancreatic duct dilatation (arrow). (D) Abdominopelvic CT with pancreatic head neoplasm (arrowhead). CT, computed tomography.
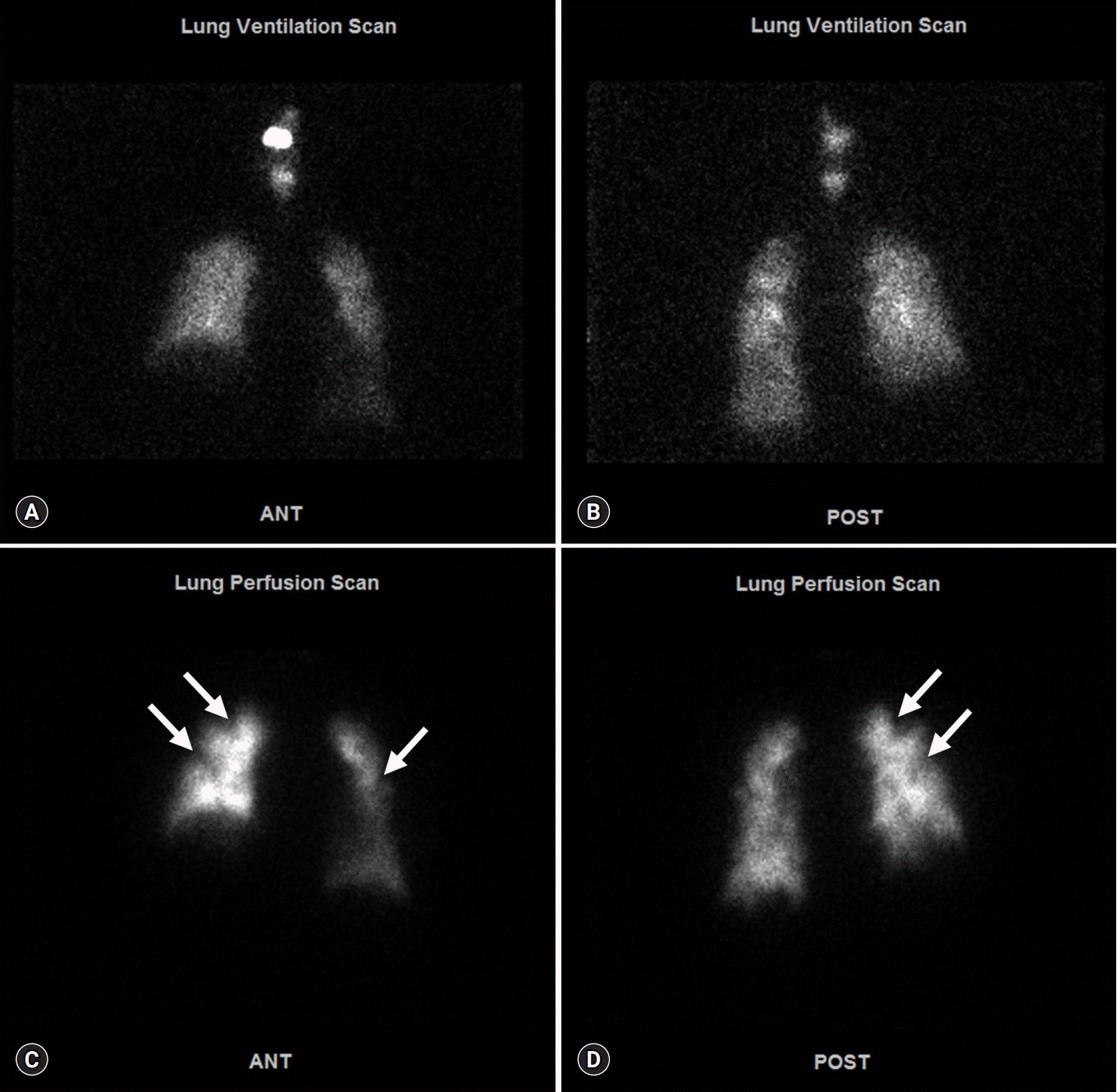
Fig. 3. Ventilation/perfusion lung scan. Anterior view (A) and posterior view (B) of ventilation lung scan present no significant decreased ventilation activity. Anterior view (C) and posterior view (D) of perfusion lung scan show multifocal peripherally distributed small perfusion defects in bilateral lung fields (arrows).

Fig. 4. 18F-2-fluoro-2-deoxy-D-glucose-positron emission tomography integrated with computed tomography. Maximum intensity projection image (A) and fusion axial views (B, C) show a hypermetabolic mass at the pancreatic head and neck region (arrow) with systemic lymph nodes, bilateral lung and both pleural metastases (arrowhead).
Reference
-
References
1. von Herbay A, Illes A, Waldherr R, Otto HF. Pulmonary tumor thrombotic microangiopathy with pulmonary hypertension. Cancer. 1990; 66:587–92.
Article2. Price LC, Seckl MJ, Dorfmüller P, Wort SJ. Tumoral pulmonary hypertension. Eur Respir Rev. 2019; 28:pii: 180065.
Article3. Price LC, Wells AU, Wort SJ. Pulmonary tumour thrombotic microangiopathy. Curr Opin Pulm Med. 2016; 22:421–8.
Article4. Chun YS, Pawlik TM, Vauthey JN. 8th edition of the AJCC cancer staging manual: pancreas and hepatobiliary cancers. Ann Surg Oncol. 2018; 25:845–7.
Article5. Fujishiro T, Shuto K, Shiratori T, Kono T, Akutsu Y, Uesato M, et al. A case report of pulmonary tumor thrombotic microangiopathy (PTTM) caused by esophageal squamous cell carcinoma. Esophagus. 2013; 10:247–51.
Article6. Patrignani A, Purcaro A, Calcagnoli F, Mandolesi A, Bearzi I, Ciampani N. Pulmonary tumor thrombotic microangiopathy: the challenge of the antemortem diagnosis. J Cardiovasc Med (Hagerstown). 2014; 15:828–33.7. Godbole RH, Saggar R, Kamangar N. Pulmonary tumor thrombotic microangiopathy: a systematic review. Pulm Circ. 2019; 9:2045894019851000.
Article8. Uruga H, Fujii T, Kurosaki A, Hanada S, Takaya H, Miyamoto A, et al. Pulmonary tumor thrombotic microangiopathy: a clinical analysis of 30 autopsy cases. Intern Med. 2013; 52:1317–23.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pain Control, Nutritional and Emotional Support
- Pancreatic Cancer with Brain Metastases: Case Report with Literature Review
- Heart Transplantation Performed in a Patient with Isolated Cardiac Sarcoidosis
- Supportive Care for Symptom Relief in Pancreatic Cancer
- Fatal liver injury complicated by percutaneous catheter drainage after distal pancreatosplenectomy in a patient with pancreatic cancer
