Anterior Gradient 3 Promotes Breast Cancer Development and Chemotherapy Response
- Affiliations
-
- 1Department of Tumor Cell Biology, Tianjin Medical University Cancer Institute and Hospital, National Clinical Research Center for Cancer, Tianjin, China
- 2Tianjin’s Clinical Research Center for Cancer, Tianjin, China
- 3Key Laboratory of Cancer Prevention and Therapy, Tianjin, Chin
- 4Key Laboratory of Breast Cancer Prevention and Therapy, Tianjin Medical University, Ministry of Education, Tianjin, China
- 5Department of Breast Cancer Pathology and Research Laboratory, Tianjin Medical University Cancer Institute and Hospital, Tianjin, China
- KMID: 2501215
- DOI: http://doi.org/10.4143/crt.2019.217
Abstract
- Purpose
Anterior gradient 3 (AGR3) belongs to human anterior gradient (AGR) family. The function of AGR3 on cancer remains unknown. This research aimed to investigate if AGR3 had prognostic values in invasive ductal carcinoma (IDC) of breast cancer and could promote tumor progression.
Materials and Methods
AGR3 expression was detected in breast benign lesions, ductal carcinoma in situ and IDC by immunohistochemistry analysis. AGR3’s correlations with clinicopathological features and prognosis of IDC patients were analyzed. By cell function experiments, collagen gel droplet-embedded culture drug sensitivity test and cytotoxic analysis, AGR3’s impacts on proliferation, invasion ability, and chemotherapeutic drug sensitivity of breast cancer cells were also detected.
Results
AGR3 was up-regulated in luminal subtype of histological grade I-II of IDC patients and positively correlated with high risks of recurrence and distant metastasis. AGR3 high expression could lead to bone or liver metastasis and predict poor prognosis of luminal B. In cell lines, AGR3 could promote proliferation and invasion ability of breast cancer cells which were consistent with clinical analysis. Besides, AGR3 could indicate poor prognosis of breast cancer patients treated with taxane but a favorable prognosis with 5-fluoropyrimidines. And breast cancer cells with AGR3 high expression were resistant to taxane but sensitive to 5-fluoropyrimidines.
Conclusion
AGR3 might be a potential prognostic indicator in luminal B subtype of IDC patients of histological grade I-II. And patients with AGR3 high expression should be treated with chemotherapy regimens consisting of 5-fluoropyrimidines but no taxane.
Keyword
Figure
-

Fig. 1. Anterior gradient 3 (AGR3) expression increased with the development of breast tumor malignancy and was negatively correlated with histological grade but positively correlated with estrogen receptor (ER)/progesterone receptor (PR) status. (A) Representative immunohistochemistry (IHC) images of AGR3 low expression group (upper) and AGR3 high expression group (lower). (B) AGR3 expression increased with progression of malignancy degree of lesions. AGR3 expression of benign lesions was low, ductal carcinoma in situ (DCIS) was higher and IDC was the highest. (C) Representative IHC images of AGR3 expression in different histological grades of IDC (left panel). Western blot analysis of AGR3 expression in the frozen breast tumor specimens consisting of normal tissues, grade I, grade II, and grade III. Every type of tissues had 6 cases. β-actin was used as a loading control (right panel). (D) The expression of AGR3, ER, and PR were detected by IHC in serial paraffin sections. The upper panel was representative IHC images of AGR3 and ER. The lower was AGR3 and PR. (E) Representative IHC images of AGR3 expression in disease-free group and recurrence or metastasis group.

Fig. 2. High expression of anterior gradient 3 (AGR3) was associated with high risk of recurrence or metastasis in luminal B subtype of invasive ductal carcinoma (IDC) patients of grade I-II. Compared the proportion of AGR3 highly expressed patients in the group developing metastasis or recurrence (MR group) and the group disease-free (DF group). Besides, compared the proportion of AGR3 highly expressed patients in the group developing metastasis or recurrence within 5 years (MR 5 years group) and the group disease-free over 5 years (DF 5 years group). The proportion of every group was as follows. (A) MR, 55.1%; DF, 33.7%; MR 5 years, 50.0%; DF 5 years, 33.9%. (B) Luminal of MR, 70.8%; luminal of DF, 40.9%; luminal of MR 5 years, 69.4%; luminal of DF 5 years, 42.2%. (C) Luminal A of MR, 56.9%; luminal A of DF, 37.7%; luminal A of MR 5 years, 72.7%; luminal A of DF 5 years, 40.0%. (D) Luminal B of MR, 68.6%; luminal B of DF, 42.2%; luminal B of MR 5 years, 68.0%; luminal B of DF 5 years, 43.0%. (E) Non-luminal of MR, 19.0%; non-luminal of DF, 10.4%; non-luminal of MR 5 years, 15.0%; non-luminal of DF 5 years, 2.6%. (F) Human epidermal growth factor receptor 2 (HER2)-overexpressing of MR, 13.0%; HER2-overexpressing of DF, 0%; HER2-overexpressing of MR 5 years, 0%; HER2-overexpressing of DF 5 years, 7.7%. (G) Triple-negative breast cancer (TNBC) of MR, 23.5%; TNBC of DF, 9.1%; TNBC of MR 5 years, 18.7%; TNBC of DF 5 years, 0%. (H) Grade Ⅰ-Ⅱ of MR, 64.0%; grade Ⅰ-Ⅱ of DF, 36.5%; grade Ⅰ-Ⅱ of MR 5 years, 58.5%; grade Ⅰ-Ⅱ of DF 5 years, 37.0%. (I) Luminal of grade Ⅰ-Ⅱ in MR, 75.68%; luminal of grade Ⅰ-Ⅱ in DF, 43.13%; luminal of grade Ⅰ-Ⅱ in MR 5 years, 72.41%; luminal of grade Ⅰ-Ⅱ in DF 5 years, 44.44%. (J) Luminal A of grade Ⅰ-Ⅱ in MR, 72.72%; luminal A of grade Ⅰ-Ⅱ in DF, 40.91%; luminal A of grade Ⅰ-Ⅱ in MR 5 years, 70.0%; luminal A of grade Ⅰ-Ⅱ in DF 5 years, 44.8%. (K) Luminal B of grade Ⅰ-Ⅱ in MR, 76.9%; luminal B of grade Ⅰ-Ⅱ in DF, 43.9%; luminal B of grade Ⅰ-Ⅱ in MR 5 years, 73.7%; luminal B of grade Ⅰ-Ⅱ in DF 5 years, 44.3%. (L) Non-luminal of grade Ⅰ-Ⅱ in MR, 30.8%; non-luminal of grade Ⅰ-Ⅱ in DF, 8.9%; non-luminal of grade Ⅰ-Ⅱ in MR 5 years, 17.0%; non-luminal of grade Ⅰ-Ⅱ in DF 5 years, 0%. (M) TNBC of grade Ⅰ-Ⅱ in MR, 36.4%; TNBC of grade Ⅰ-Ⅱ in DF, 10.3%; TNBC of grade Ⅰ-Ⅱ in MR 5 years, 30.0%; TNBC of grade Ⅰ-Ⅱ in DF 5 years, 0%. (N) Grade Ⅲ of MR, 30.8%; grade Ⅲ of DF, 20.0%; grade Ⅲ of MR 5 years, 20.7%; grade Ⅲ of DF 5 years, 22.2%.
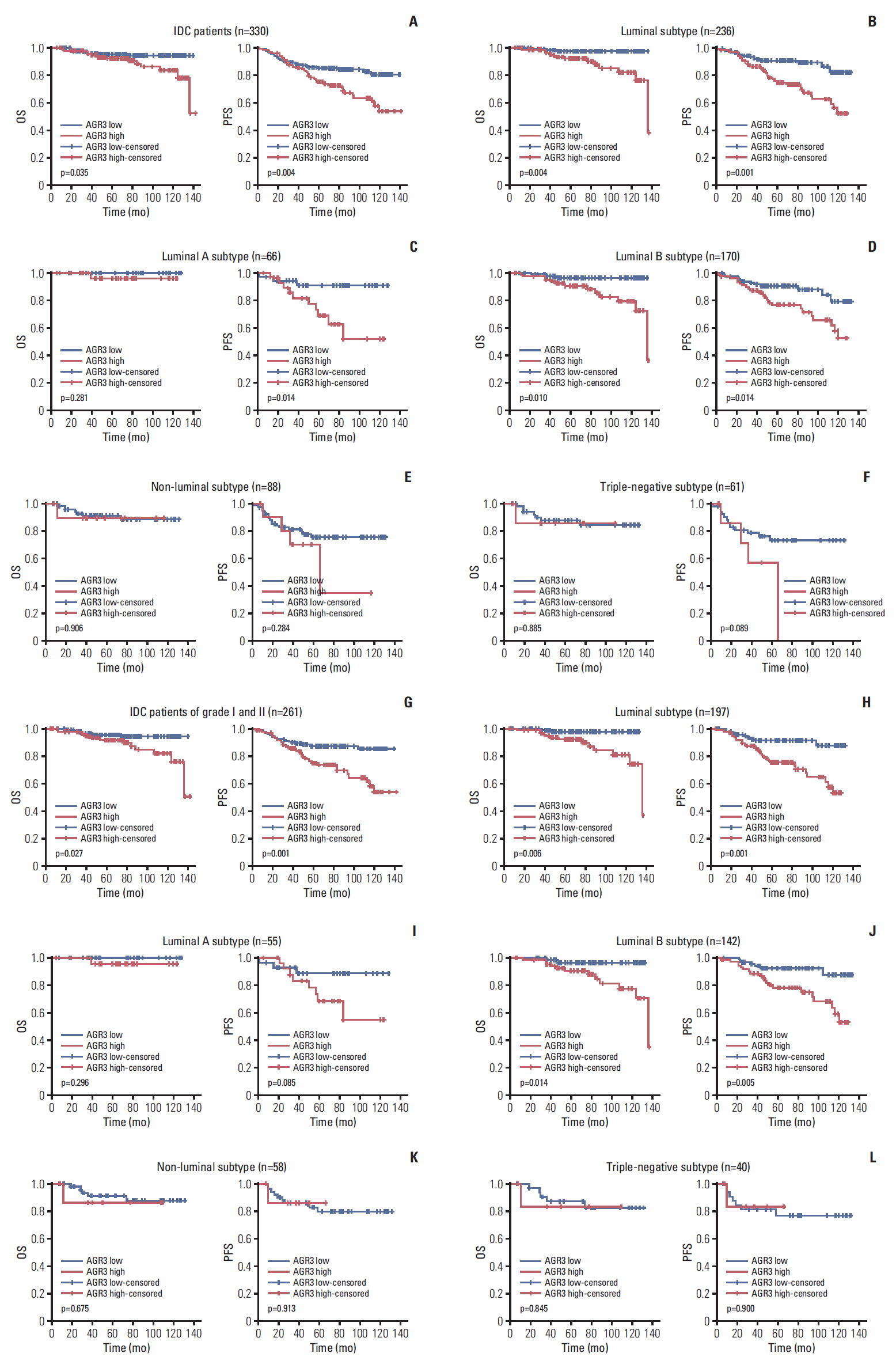
Fig. 3. High expression of anterior gradient 3 (AGR3) was associated with poor prognosis in luminal B subtype of invasive ductal carcinoma (IDC) patients of grade I-II. (A) Overall survival (OS) and progression-free survival (PFS) curves of 330 cases of IDC patients were shown, respectively. (B) OS and PFS of 236 luminal patients were shown, respectively. (C) OS and PFS of 66 luminal A patients were shown, respectively. (D) OS and PFS of 170 luminal B patients were shown, respectively. (E) OS and PFS of 88 non-luminal patients were shown, respectively. (F) OS and PFS of 61 triple-negative breast cancer (TNBC) patients were shown, respectively. (G) OS and PFS curves of 261 IDC patients of grade Ⅰ-Ⅱ were shown, respectively. (H) OS and PFS of 197 luminal patients of grade Ⅰ-Ⅱ were shown, respectively. (I) OS and PFS of 55 luminal A patients of grade Ⅰ-Ⅱ were shown, respectively. (J) OS and PFS of 142 luminal B patients of grade Ⅰ-Ⅱ were shown, respectively. (K) OS and PFS of 58 non-luminal patients of grade Ⅰ-Ⅱ were shown, respectively. (L) OS and PFS of 40 TNBC patients of grade Ⅰ-Ⅱ were shown, respectively.
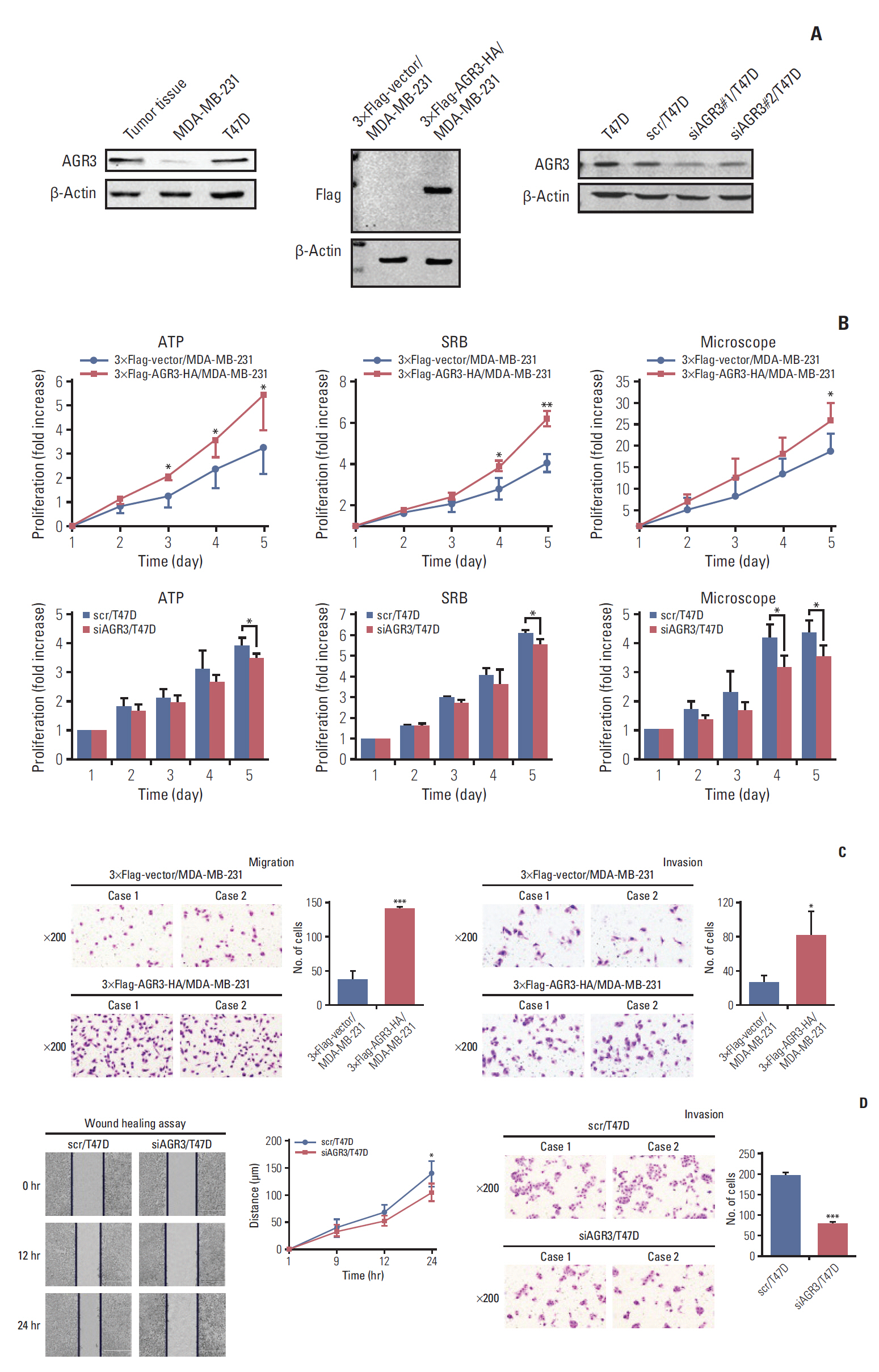
Fig. 4. Anterior gradient 3 (AGR3) promoted proliferation and invasion ability of breast cancer cells. (A) Western blot analysis of AGR3 expression in MDA-MB-231 and T47D cells (patient tissues with AGR3 high expression as positive control) (left panel). AGR3 expression was detected by primary flag antibodies in 3×Flag-vector/MDA-MB-231 and 3×Flag-AGR3-HA/MDA-MB-231 cells (middle panel). AGR3 expression was detected by primary AGR3 antibodies in T47D, scr/T47D and siAGR3/T47D cells (right panel). (B) Proliferation ability was detected by ATP and sulforhodamine B (SRB) assays in 3×Flag-vector/MDA-MB-231 and 3×Flag-AGR3-HA/MDA-MB-231 cells, respectively (upper panel in left and middle). Proliferation assay was repeated by using Nikon ECLIPSE Ti microscope to count cell number in 3×Flag-vector/MDA-MB-231 and 3×Flag-AGR3-HA/MDA-MB-231 cells (upper panel in right). Proliferation ability was also detected by ATP and SRB assays in scr/T47D and siAGR3/T47D cells, respectively (lower panel in left and middle). Proliferation assay was also repeated by using Nikon ECLIPSE Ti microscope to count cell numbers in scr/T47D and siAGR3/T47D cells (lower panel in right). Bars are mean±SD. All experiments were performed 3 times independently (*p < 0.05, **p < 0.01). (C) Migration ability was detected by Matrigel Boyden chamber assays in 3×Flag-vector/MDA-MB-231 and 3×Flag-AGR3-HA/MDA-MB-231 cells (upper panel). Migration ability was detected by wound healing assays in scr/T47D and siAGR3/T47D cells (lower panel). Bars are mean±SD. All experiments were performed 3 times independently (*p < 0.05, ***p < 0.001). (D) Invasion ability was detected by Matrigel Boyden chamber assays in 3×Flag-vector/MDA-MB-231 and 3×Flag-AGR3-HA/MDA-MB-231 cells (upper panel). Invasion ability was detected by Matrigel Boyden chamber assays in scr/T47D and siAGR3/T47D cells (lower panel). Bars are mean±SD. All experiments were performed 3 times independently (*p < 0.05, ***p < 0.001).

Fig. 5. Anterior gradient 3 (AGR3)’s indication role for therapeutic response of taxane and 5-fluoropyrimidines in luminal patients of grade I-II. (A) Overall survival (OS) and progression-free survival (PFS) curves of AGR3 highly expressed invasive ductal carcinoma (IDC) patients with different chemotherapy regimens were shown, respectively. TE, taxane+epirubicin; CEF, cyclophosphamide, epirubicin and 5-fluoropyrimidines; CMF, cyclophosphamide, methotrexate and 5-fluoropyrimidines. (B) OS and PFS curves of AGR3 low expressed IDC patients with different chemotherapy regimens were shown, respectively. (C) OS and PFS curves of AGR3 highly expressed IDC patients with taxane treatment were shown, respectively (upper panel). OS and PFS curves of AGR3 low expressed IDC patients with taxane treatment were shown, respectively (lower panel). T, taxane. (D) OS and PFS curves of AGR3 highly expressed IDC patients with 5-fluoropyrimidines treatment were shown, respectively (upper panel). OS and PFS curves of AGR3 low expressed IDC patients with 5-fluoropyrimidines treatment were shown, respectively (lower panel). F, 5-fluoropyrimidine. (E) OS and PFS curves of AGR3 highly expressed luminal patients with taxane treatment were shown, respectively (upper panel). OS and PFS curves of AGR3 low expressed luminal patients with taxane treatment were shown, respectively (lower panel). (F) OS and PFS curves of AGR3 highly expressed luminal patients with 5-fluoropyrimidines treatment were shown, respectively (upper panel). OS and PFS curves of AGR3 low expressed luminal patients with 5-fluoropyrimidines treatment were shown, respectively (lower panel). (G) OS and PFS curves of AGR3 highly expressed IDC patients of grade Ⅰ-Ⅱ with taxane treatment were shown, respectively (upper panel). OS and PFS curves of AGR3 low expressed IDC patients of grade Ⅰ-Ⅱ with taxane treatment were shown, respectively (lower panel). (H) OS and PFS curves of AGR3 highly expressed IDC patients of grade Ⅰ-Ⅱ with 5-fluoropyrimidines treatment were shown, respectively (upper panel). OS and PFS curves of AGR3 low expressed IDC patients of grade Ⅰ-Ⅱ with 5-fluoropyrimidines treatment were shown, respectively (lower panel). (I) OS and PFS curves of AGR3 highly expressed luminal patients of grade Ⅰ-Ⅱ with taxane treatment were shown, respectively (upper panel). OS and PFS curves of AGR3 low expressed luminal patients of grade Ⅰ-Ⅱ with taxane treatment were shown, respectively (lower panel). (J) OS and PFS curves of AGR3 highly expressed luminal patients of grade Ⅰ-Ⅱ with 5-fluoropyrimidines treatment were shown, respectively (upper panel). OS and PFS curves of AGR3 low expressed luminal patients of grade Ⅰ-Ⅱ with 5-fluoropyrimidines treatment were shown, respectively (lower panel).
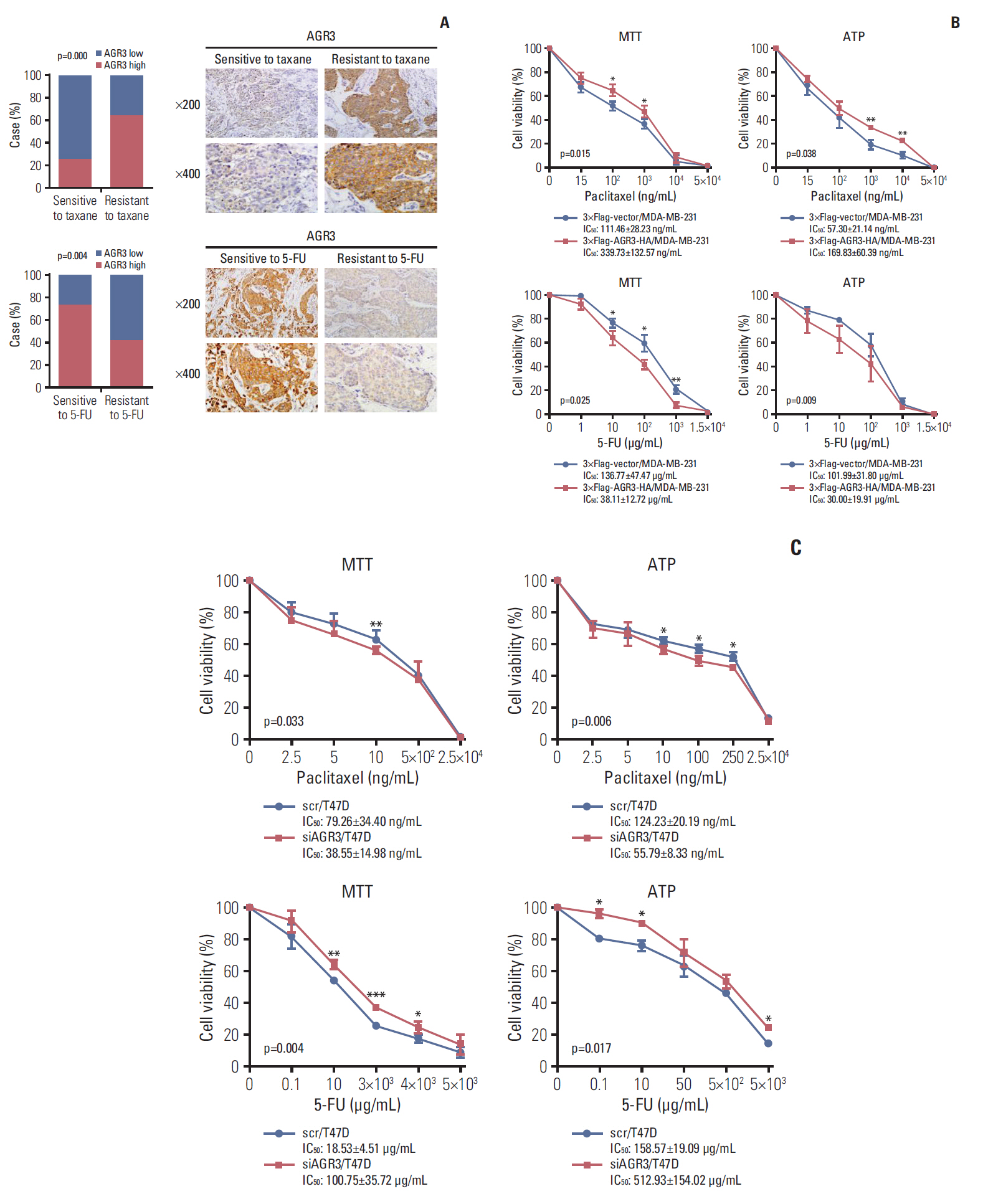
Fig. 6. Breast cancer cells with anterior gradient 3 (AGR3) high expression were resistant to taxane but sensitive to 5-fluoropyrimidines (5-FU). (A) Compared the proportion of AGR3 highly expressed patients in groups with different drug sensitivities. Taxane sensitive group was 25% and resistant group was 64.1% (p=0.000, upper panel in left). Upper panel in right was representative immunohistochemistry (IHC) images of AGR3 expression in taxane sensitive and resistant group. 5-FU sensitive group was 73.3% and resistant group was 42.1% (p=0.004, lower panel in left). Lower panel in right were representative IHC images of AGR3 expression in 5-FU sensitive and resistant group. (B) With the treatment of taxane, cell viability of 3×Flag-AGR3-HA/MDA-MB-231 cells was much higher than 3×Flag-vector/MDA-MB-231 cells (*p < 0.05, ** p < 0.01, upper panel). Taxane IC50 values of 3×Flag-AGR3-HA/MDA-MB-231 cells in MTT and ATP assay were much higher than 3×Flag-vector/MDA-MB-231 cells (MTT, p=0.015; ATP, p=0.038, upper panel). With the treatment of 5-FU, cell viability of 3×Flag-AGR3-HA/MDA-MB-231 cells was much lower than 3×Flag-vector/MDA-MB-231 cells (*p < 0.05, **p < 0.01, lower panel). 5-FU IC50 value of 3×Flag-AGR3-HA/MDA-MB-231 cells in MTT and ATP assay were much lower than 3×Flag-vector/MDA-MB-231 cells (MTT, p=0.025; ATP, p=0.009, lower panel). (C) With the treatment of taxane, cell viability of siAGR3/T47D cells was much lower than scr/T47D cells (*p < 0.05, ** p < 0.01, upper panel). Taxane IC50 values of siAGR3/T47D cells in MTT and ATP assay were much lower than scr/T47D cells (MTT, p=0.033; ATP, p=0.006, upper panel). With the treatment of 5-FU, cell viability of siAGR3/T47D cells was much higher than scr/T47D cells (*p < 0.05, **p < 0.01, ***p < 0.001, lower panel). 5-FU IC50 value of siAGR3/T47D cells in MTT and ATP assay were much higher than scr/T47D cells (MTT, p=0.004; ATP, p=0.017, lower panel).
Reference
-
References
1. Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin. 2013; 63:11–30.
Article2. Mendes TF, Kluskens LD, Rodrigues LR. Triple negative breast cancer: nanosolutions for a big challenge. Adv Sci (Weinh). 2015; 2:1500053.
Article3. Abdel-Hafiz HA. Epigenetic mechanisms of tamoxifen resistance in luminal breast cancer. Diseases. 2017; 5:E16.
Article4. Hart CD, Sanna G, Siclari O, Biganzoli L, Di Leo A. Defining optimal duration and predicting benefit from chemotherapy in patients with luminal-like subtypes. Breast. 2015; 24 Suppl 2:S136–42.
Article5. Tran B, Bedard PL. Luminal-B breast cancer and novel therapeutic targets. Breast Cancer Res. 2011; 13:221.
Article6. Ivanova AS, Tereshina MB, Ermakova GV, Belousov VV, Zaraisky AG. Agr genes, missing in amniotes, are involved in the body appendages regeneration in frog tadpoles. Sci Rep. 2013; 3:1279.
Article7. Thompson DA, Weigel RJ. hAG-2, the human homologue of the Xenopus laevis cement gland gene XAG-2, is coexpressed with estrogen receptor in breast cancer cell lines. Biochem Biophys Res Commun. 1998; 251:111–6.8. Fletcher GC, Patel S, Tyson K, Adam PJ, Schenker M, Loader JA, et al. hAG-2 and hAG-3, human homologues of genes involved in differentiation, are associated with oestrogen receptor-positive breast tumours and interact with metastasis gene C4.4a and dystroglycan. Br J Cancer. 2003; 88:579–85.
Article9. Wilson CL, Sims AH, Howell A, Miller CJ, Clarke RB. Effects of oestrogen on gene expression in epithelium and stroma of normal human breast tissue. Endocr Relat Cancer. 2006; 13:617–28.
Article10. Hrstka R, Nenutil R, Fourtouna A, Maslon MM, Naughton C, Langdon S, et al. The pro-metastatic protein anterior gradient-2 predicts poor prognosis in tamoxifen-treated breast cancers. Oncogene. 2010; 29:4838–47.
Article11. Park K, Chung YJ, So H, Kim K, Park J, Oh M, et al. AGR2, a mucinous ovarian cancer marker, promotes cell proliferation and migration. Exp Mol Med. 2011; 43:91–100.
Article12. Zhang JS, Gong A, Cheville JC, Smith DI, Young CY. AGR2, an androgen-inducible secretory protein overexpressed in prostate cancer. Genes Chromosomes Cancer. 2005; 43:249–59.
Article13. Pohler E, Craig AL, Cotton J, Lawrie L, Dillon JF, Ross P, et al. The Barrett’s antigen anterior gradient-2 silences the p53 transcriptional response to DNA damage. Mol Cell Proteomics. 2004; 3:534–47.
Article14. Fritzsche FR, Dahl E, Dankof A, Burkhardt M, Pahl S, Petersen I, et al. Expression of AGR2 in non small cell lung cancer. Histol Histopathol. 2007; 22:703–8.15. Ramachandran V, Arumugam T, Wang H, Logsdon CD. Anterior gradient 2 is expressed and secreted during the development of pancreatic cancer and promotes cancer cell survival. Cancer Res. 2008; 68:7811–8.
Article16. Adam PJ, Boyd R, Tyson KL, Fletcher GC, Stamps A, Hudson L, et al. Comprehensive proteomic analysis of breast cancer cell membranes reveals unique proteins with potential roles in clinical cancer. J Biol Chem. 2003; 278:6482–9.
Article17. Garczyk S, von Stillfried S, Antonopoulos W, Hartmann A, Schrauder MG, Fasching PA, et al. AGR3 in breast cancer: prognostic impact and suitable serum-based biomarker for early cancer detection. PLoS One. 2015; 10:e0122106.
Article18. Li H, Narahara H. 15-Deoxy-Δ(12,14)-prostaglandin J(2) induces growth inhibition, cell cycle arrest and apoptosis in human endometrial cancer cell lines. Int J Mol Med. 2013; 31:778–88.
Article19. Pascal LE, Vencio RZ, Page LS, Liebeskind ES, Shadle CP, Troisch P, et al. Gene expression relationship between prostate cancer cells of Gleason 3, 4 and normal epithelial cells as revealed by cell type-specific transcriptomes. BMC Cancer. 2009; 9:452.
Article20. Gray TA, MacLaine NJ, Michie CO, Bouchalova P, Murray E, Howie J, et al. Anterior Gradient-3: a novel biomarker for ovarian cancer that mediates cisplatin resistance in xenograft models. J Immunol Methods. 2012; 378:20–32.
Article21. Vaarala MH, Hirvikoski P, Kauppila S, Paavonen TK. Identification of androgen-regulated genes in human prostate. Mol Med Rep. 2012; 6:466–72.
Article22. Bu H, Schweiger MR, Manke T, Wunderlich A, Timmermann B, Kerick M, et al. Anterior gradient 2 and 3: two prototype androgen-responsive genes transcriptionally upregulated by androgens and by oestrogens in prostate cancer cells. FEBS J. 2013; 280:1249–66.23. Obacz J, Brychtova V, Podhorec J, Fabian P, Dobes P, Vojtesek B, et al. Anterior gradient protein 3 is associated with less aggressive tumors and better outcome of breast cancer patients. Onco Targets Ther. 2015; 8:1523–32.24. King ER, Tung CS, Tsang YT, Zu Z, Lok GT, Deavers MT, et al. The anterior gradient homolog 3 (AGR3) gene is associated with differentiation and survival in ovarian cancer. Am J Surg Pathol. 2011; 35:904–12.
Article25. Welboren WJ, van Driel MA, Janssen-Megens EM, van Heeringen SJ, Sweep FC, Span PN, et al. ChIP-Seq of ERalpha and RNA polymerase II defines genes differentially responding to ligands. EMBO J. 2009; 28:1418–28.26. Mhaidat NM, Thorne R, Zhang XD, Hersey P. Involvement of endoplasmic reticulum stress in Docetaxel-induced JNK-dependent apoptosis of human melanoma. Apoptosis. 2008; 13:1505–12.
Article27. McGrath EP, Logue SE, Mnich K, Deegan S, Jager R, Gorman AM, et al. The unfolded protein response in breast cancer. Cancers (Basel). 2018; 10:E344.
Article28. Ryu J, Park SG, Lee PY, Cho S, Lee DH, Kim GH, et al. Dimerization of pro-oncogenic protein Anterior Gradient 2 is required for the interaction with BiP/GRP78. Biochem Biophys Res Commun. 2013; 430:610–5.
Article29. Kim JK, Kang KA, Piao MJ, Ryu YS, Han X, Fernando PM, et al. Endoplasmic reticulum stress induces 5-fluorouracil resistance in human colon cancer cells. Environ Toxicol Pharmacol. 2016; 44:128–33.
Article30. Yun S, Han YS, Lee JH, Kim S, Lee SH. Enhanced susceptibility to 5-fluorouracil in human colon cancer cells by silencing of GRP78. Anticancer Res. 2017; 37:2975–84.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comment on “Histomorphological Factors Predicting the Response to Neoadjuvant Chemotherapy in Triple-Negative Breast Cancerâ€
- Correlation between Tumor Response to Neoadjuvant Chemotherapy and Patient Outcome in Breast Cancer
- Correlation between Tumor Response to Neoadjuvant Chemotherapy and Patient Outcome in Breast Cancer
- Treatment with Cisplatin and Etoposide Chemotherapy in Patient with Metastatic Breast Cancer
- Chemotherapy in Breast Cancer
