Anesth Pain Med.
2020 Jan;15(1):73-77. 10.17085/apm.2020.15.1.73.
Successful wire-guided fiberoptic nasotracheal intubation in a patient with hemifacial microsomia - A case report -
- Affiliations
-
- 1Department of Anesthesiology and Pain Medicine, National Health Insurance Service Ilsan Hospital, Goyang, Korea
- 2Department of Anesthesiology and Pain Medicine, Yonsei University College of Medicine, Seoul, Korea
- KMID: 2500458
- DOI: http://doi.org/10.17085/apm.2020.15.1.73
Abstract
- Background
Patients with hemifacial microsomia may have a difficult airway due to the accompanying mandibular deformity. Fiberoptic bronchoscope-guided intubation is commonly used method for difficult airway management. However, awake fiberoptic nasotracheal intubation has several disadvantages, including difficulty in advancement of the endotracheal tube (ETT) due to the resistance between the ETT and bronchoscope. Wire-guided fiberoptic nasotracheal intubation may help to overcome the drawbacks of the conventional method. Case: An 18-year-old man with hemifacial microsomia was scheduled for double-jaw surgery. In preoperative evaluation, he had severe retrognathia and expected difficult airway. We successfully performed wire-guided fiberoptic nasotracheal intubation combined with high-flow nasal cannula and deep sedation without any complications.
Conclusions
A guidewire may be useful, in case of difficultly in advancing the ETT or if a smaller tube is required, while performing intubation with FOB in patients with difficult airways.
Keyword
Figure
-
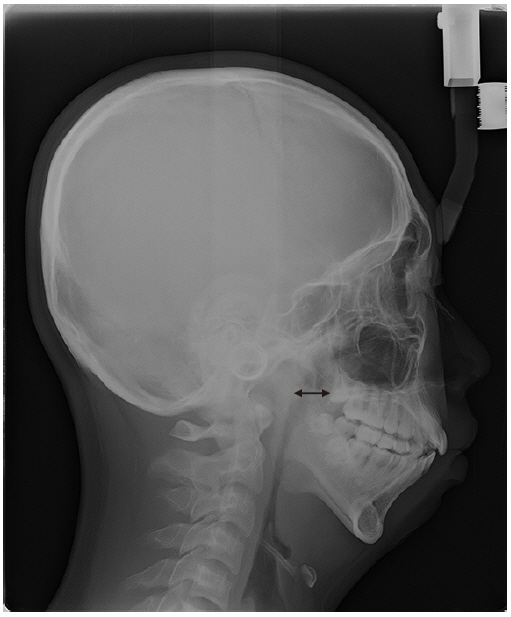
Fig. 1 Narrowing of the nasopharyngeal airway seen on the oral panoramic view X-ray (double-headed arrow).
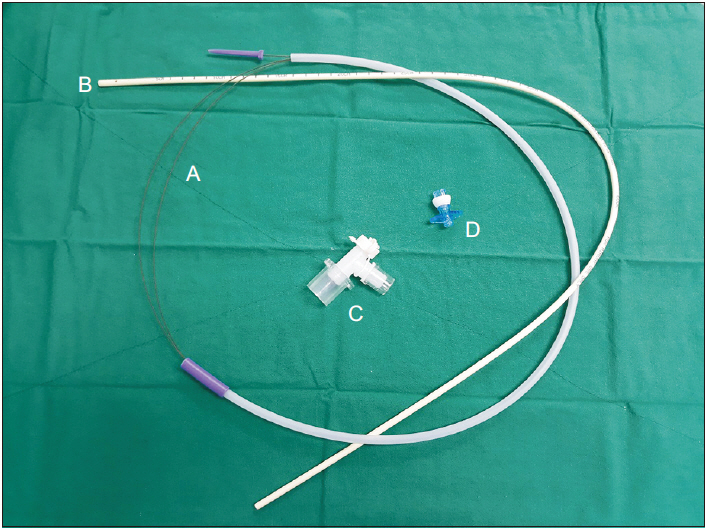
Fig. 2 Angio Guidewire and airway exchange catheter set A: straighttipped Angio Guidewire (Lunderquist-ring, Cook Critical Care), B: exchange catheter (CAEC, Cook Critical Care), C: bronchoscope airway adapter, D: Rapi-Fit® adapter.
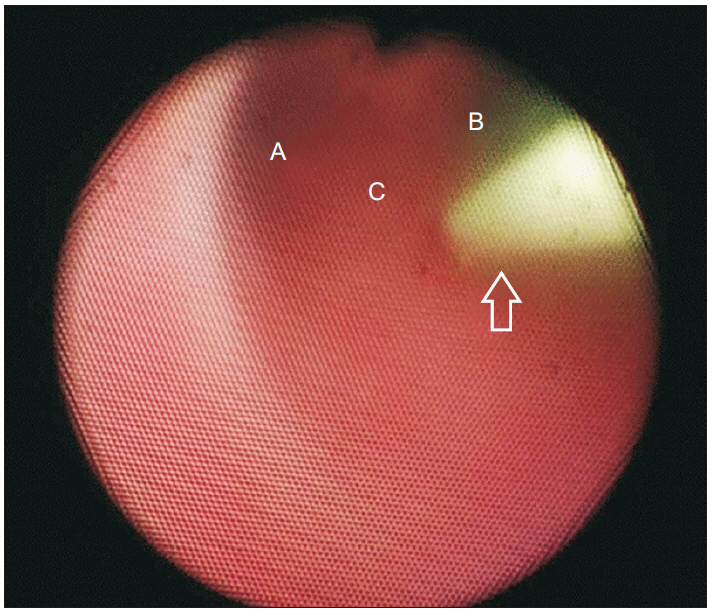
Fig. 3 The fiberoptic bronchoscope showing that the guidewire is positioned in the trachea A: left main bronchus, B: right main bronchus, C: carina, Empty arrow: guide wire.
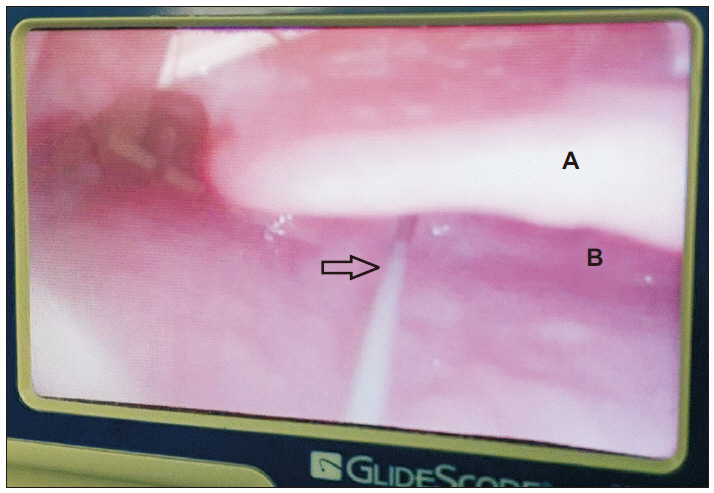
Fig. 4 The guidewire passing through the vocal cord and into the trachea as seen with the Glidescope® A: epiglottis, B: arytenoid cartilage, Empty arrow: guide wire.
Reference
-
Mielnik-Błaszczak M., Olszewska K. 2011. Hemifacial microsomia-review of the literature. Dent Med Probl. 48:80–5.Nargozian C. 2004. The airway in patients with craniofacial abnormalities. Paediatr Anaesth. 14:53–9. DOI: 10.1046/j.1460-9592.2003.01200.x. PMID: 14717875.Heier JM., Schroeder KM., Galgon RE., Arndt GA. 2012. Wire-guided (Seldinger technique) intubation through a face mask in urgent, difficult and grossly distorted airways. Saudi J Anaesth. 6:292–4. DOI: 10.4103/1658-354X.101226. PMID: 23162408. PMCID: PMC3498673.Arndt GA., Topp J., Hannah J., McDowell TS., Lesko A. 1998. Intubation via the LMA using a Cook retrograde intubation kit. Can J Anaesth. 45:257–60. DOI: 10.1007/BF03012912. PMID: 9579265.Cooper JR Jr Jr. 2002. Use of a LMA and a sequential technique for unanticipated difficult intubations. Anesthesiology. 97:1326. DOI: 10.1097/00000542-200211000-00050. PMID: 12411829.Rajan GR. 2005. Fiberoptic wire-guided transoral and through the LMA intubation technique using modified gum elastic bougie. Anesth Analg. 100:599–600. DOI: 10.1213/01.ANE.0000144080.77294.4E. PMID: 15673908.Warrillow S. 2005. Difficult intubation managed using standard laryngeal mask airway, flexible fibreoptic bronchoscope and wire guided enteral feeding tube. Anaesth Intensive Care. 33:659–61. DOI: 10.1177/0310057X0503300518. PMID: 16235488.Joffe AM., Arndt G., Willmann K. 2010. Wire-guided catheter exchange after failed direct laryngoscopy in critically ill adults. J Clin Anesth. 22:93–6. DOI: 10.1016/j.jclinane.2009.02.017. PMID: 20304349.El-Anwar MW., Ali AH., Elnashar I., Elfiki IM., Ahmed AF., Abdulmonaem G. 2017. Normal nasopharyngeal measurement by computed tomography in adult. J Craniofac Surg. 28:e395–8. DOI: 10.1097/SCS.0000000000003764. PMID: 28590397.Apfelbaum JL., Hagberg CA., Caplan RA., Blitt CD., Connis RT., Nickinovich DG, et al. 2013. Practice guidelines for management of the difficult airway: an updated report by the American Society of Anesthesiologists Task Force on Management of the Difficult Airway. Anesthesiology. 118:251–70. DOI: 10.1097/ALN.0b013e31827773b2. PMID: 23364566.Paul A., Nathroy A. 2017. Awake fiberoptic nasal intubation in a patient scheduled for commando's operation. Int J Health Allied Sci. 6:123–6.Naithani M., Jain A. 2011. Failed nasal intubation after successful flexible bronchoscopy: guide wire to the rescue. J Anaesthesiol Clin Pharmacol. 27:395–7. DOI: 10.4103/0970-9185.83692. PMID: 21897518. PMCID: PMC3161472.Badiger S., John M., Fearnley RA., Ahmad I. 2015. Optimizing oxygenation and intubation conditions during awake fibre-optic intubation using a high-flow nasal oxygen-delivery system. Br J Anaesth. 115:629–32. DOI: 10.1093/bja/aev262. PMID: 26253608.Berlin D., Singh I., Barjaktarevic I., Friedman O. 2016. A technique for bronchoscopic intubation during high-flow nasal cannula oxygen therapy. J Intensive Care Med. 31:213–5. DOI: 10.1177/0885066615582020. PMID: 25911299.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Use of the Airtraq(R) optical laryngoscope as a rescue airway device following failed awake flexible fiberoptic nasotracheal intubation of a patient with severe microsomia: A case report
- Effective removal of epistaxis during nasotracheal intubation utilizing a fiberoptic scope in a difficult airway: A case report
- Blind Intubation Using Fiberoptic Bronchoscope in Epistaxis
- Nasotracheal Intubation Using Fiberoptic Bronchoscope and Guidewire in a Pediatric Mandibular Fracture Patient: A case report
- Orotracheal intubation in a patient with difficult airway by using fiberoptic nasotracheal intubation: A case report
