J Korean Orthop Assoc.
2020 Feb;55(1):78-84. 10.4055/jkoa.2020.55.1.78.
Comparison of the Clinical Outcomes of an Ultrasound-Guided and C-Arm Guided Cervical Nerve Root Block
- Affiliations
-
- 1Department of Orthopedic Surgery, Institute of Wonkwang Medical Science, School of Medicine, Wonkwang University, Iksan, Korea. niceo@hanmail.net
- 2Department of Orthopedic Surgery, Sanbon Hospital, School of Medicine, Wonkwang University, Gunpo, Korea.
- KMID: 2470772
- DOI: http://doi.org/10.4055/jkoa.2020.55.1.78
Abstract
- PURPOSE
This paper compares the clinical outcomes of patients who were treated with a cervical nerve block by ultrasound and C-arm and reports the complication.
MATERIALS AND METHODS
A total of 97 patients were treated with an ultrasound-guided nerve root block from May 1, 2015 to February 8, 2018. On the other hand, 94 patients were treated with a C-arm guided nerve root block. The consequences of the cervical pain and the radiating pain before and after the procedures were reviewed using the verbal numeric rating scale (VNRS). In addition, the complications related to the procedures from the daily notes from the chart were inspected.
RESULTS
Sixty-six cases out of 97 cases of ultrasound-guided nerve root block were enrolled in the study. The average age of the patients was 57 years, including 41 males and 25 females. Seventy seven out of 94 cases by a C-arm guided root block were included in the study. The average age of the patients was 55 years, including 40 males and 37 females. Before the nerve root block, the mean numeric rating pain scale (NRS) of the cervical pain in ultrasound-guided block decreased from 5.4 points to 2.7 points at three weeks and 1.4 points at six weeks (p=0.0023, p<0.001), and 3.1 points in the C-arm (p<0.001, p<0.001) at three weeks and 1.5 points at six weeks (p<0.001, p<0.001). In the case of radiating pain, the mean NRS in the ultrasound-guided nerve root block group improved from 6.3 points after the procedure to 2.8 points at three weeks and 1.5 points at six weeks (p<0.001, p<0.001). In the C-arm guided nerve root block group, the NRS improved from 7.4 points after the procedure to 3.3 points at three weeks and 1.9 points at six weeks. In the case of complications, Horner's syndrome and propriospinal myoclonus were observed in one case of C-arm guided block group.
CONCLUSION
The clinical results of the patients who underwent ultrasound-guided cervical nerve root block were not significantly different from those who underwent a C-arm guided cervical nerve root block.
MeSH Terms
Figure
-
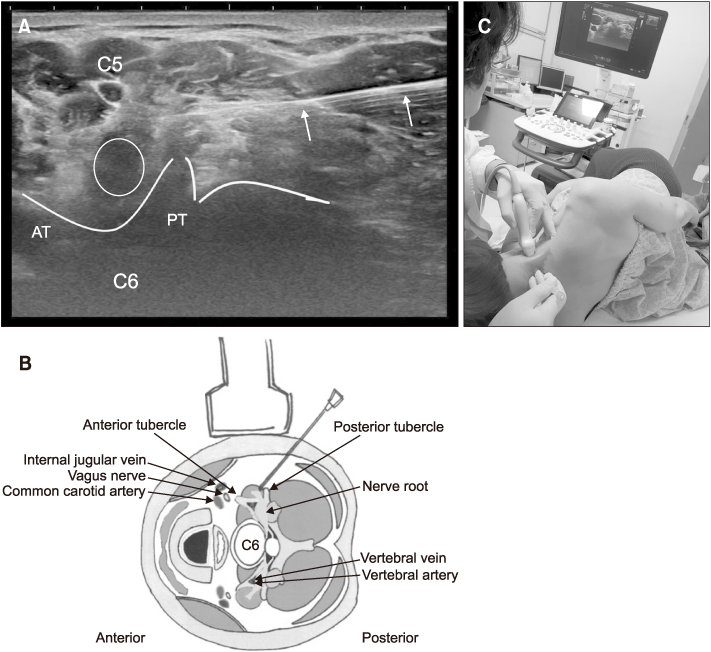
Figure 1 (A) Axial transverse ultrasound image showing a needle approaching the C6 root between the anterior and posterior tubercles. Round circle indicates C6 root, white lines indicate bony margin around tubercle. (B) Illustration showing the anatomic structures at the C6 level and the orientation of the transducer. (C) Picture shows the patient's position and the transducer for the axial view. AT, anterior tubercle; PT, posterior tubercle.
Reference
-
1. Rao R. Neck pain, cervical radiculopathy, and cervical myelopathy: pathophysiology, natural history, and clinical evaluation. J Bone Joint Surg Am. 2002; 84:1872–1881.2. Antoniadis A, Dietrich TJ, Farshad M. Does pain relief by CT-guided indirect cervical nerve root injection with local anesthetics and steroids predict pain relief after decompression surgery for cervical nerve root compression? Acta Neurochir (Wien). 2016; 158:1869–1874.
Article3. House LM, Barrette K, Mattie R, McCormick ZL. Cervical epidural steroid injection: techniques and evidence. Phys Med Rehabil Clin N Am. 2018; 29:1–17.4. Jee H, Lee JH, Kim J, Park KD, Lee WY, Park Y. Ultrasound-guided selective nerve root block versus fluoroscopy-guided transforaminal block for the treatment of radicular pain in the lower cervical spine: a randomized, blinded, controlled study. Skeletal Radiol. 2013; 42:69–78.
Article5. Narouze SN, Vydyanathan A, Kapural L, Sessler DI, Mekhail N. Ultrasound-guided cervical selective nerve root block: a fluoroscopy-controlled feasibility study. Reg Anesth Pain Med. 2009; 34:343–348.6. Park KD, Lee WY, Nam SH, Kim M, Park Y. Ultrasound-guided selective nerve root block versus fluoroscopy-guided interlaminar epidural block for the treatment of radicular pain in the lower cervical spine: a retrospective comparative study. J Ultrasound. 2019; 22:167–177.
Article7. Sun SD, Chang BK, Moon SH. Ultrasound-guided intervention in cervical spine. J Korean Orthop Assoc. 2015; 50:77–92.
Article8. Schneider BJ, Maybin S, Sturos E. Safety and complications of cervical epidural steroid injections. Phys Med Rehabil Clin N Am. 2018; 29:155–169.
Article9. Cheon BK, Kim CL, Kim KR, et al. Radiation safety: a focus on lead aprons and thyroid shields in interventional pain management. Korean J Pain. 2018; 31:244–252.
Article10. Hyun SJ, Kim KJ, Jahng TA, Kim HJ. Efficiency of lead aprons in blocking radiation - how protective are they? Heliyon. 2016; 2:e00117.
Article11. Cristante AF, Barbieri F, da Silva AAR, Dellamano JC. Radiation exposure during spine surgery using C-ARM fluoroscopy. Acta Ortop Bras. 2019; 27:46–49.
Article12. Ryu HK, Lee SG, Min BW, Ban JS, Lee JH, Kim EJ. Propriospinal myoclonus after cervical epidural blockade: a case report. Korean J Anesthesiol. 2008; 55:391–394.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Ultrasound-Guided Selective Cervical Root Block in Spondylotic Radiculopathy: Advantages and Safety
- Essential Clinical Tips about Ultrasound Guided Cervical Intervention
- Ultrasound-Guided Intervention in Lumbar Spine
- Spinal interventions under ultrasound guidance
- Ultrasound Guided Nerve Block at Vertebra and Lower Extremity
