Risk Factors Associated with Failure of Cephalomedullary Nail Fixation in the Treatment of Trochanteric Hip Fractures
- Affiliations
-
- 1Department of Orthopaedic Surgery, Hallym University Sacred Heart Hospital, Hallym University College of Medicine, Anyang, Korea.
- 2Department of Orthopaedic Surgery, Hallym University Dongtan Sacred Heart Hospital, Hallym University College of Medicine, Hwasung, Korea.
- 3Department of Orthopaedic Surgery, Hallym University Gangnam Sacred Heart Hospital, Hallym University College of Medicine, Seoul, Korea. hwangjihyo7309@gmail.com
- KMID: 2470047
- DOI: http://doi.org/10.4055/cios.2020.12.1.29
Abstract
- BACKGROUND
Intramedullary (IM) nailing is widely performed in elderly patients with trochanteric fractures. Thus, it is important to identify causative factors associated with fixation failure. We investigated fixation failures after IM nailing in elderly patients with trochanteric fractures and compared the failure group with nonfailure group to identify risk factors of fixation failure.
METHODS
A total of 396 patients aged 65 years or older underwent IM nailing for trochanteric fractures between January 2012 and August 2016 at our institution. Of those, 194 patients who were followed up for more than 12 months were enrolled in this study; 202 patients were excluded due to death during follow-up, bedridden status before injury, and loss to follow-up. All patients underwent plain radiography and preoperative computed tomography (CT).
RESULTS
Fixation failure occurred in 11 patients (5.7%). Seven patients had stable fractures (AO/OTA); eight patients had basicervical fractures (confirmed by CT). Five patients had comminution in the greater trochanter (confirmed by CT). Regarding fracture reduction, eight patients showed discontinuity in the anterior cortex. The position of the lag screw on the lateral view was in the center in six patients and in a posterior area in the other five patients. On the basis of comparison with the 183 patients without fixation failure, risk factors of fixation failure were higher body mass index (BMI; p = 0.003), basicervical type of fracture (p = 0.037), posterior placement of the lag screw on the lateral view (p < 0.001), and inaccurate reduction of the anterior cortex (p = 0.011).
CONCLUSIONS
Among the risk factors of fixation failure after IM nailing in elderly patients with trochanteric fractures, discontinuity of the anterior cortex and posterior position of the lag screw are modifiable surgeon factors, whereas higher BMI and basicervical type of fracture are nonmodifiable patient factors. Therefore, care should be taken to avoid fixation failure in IM nailing for patients with a basicervical type of fracture or higher BMI or both.
MeSH Terms
Figure
-
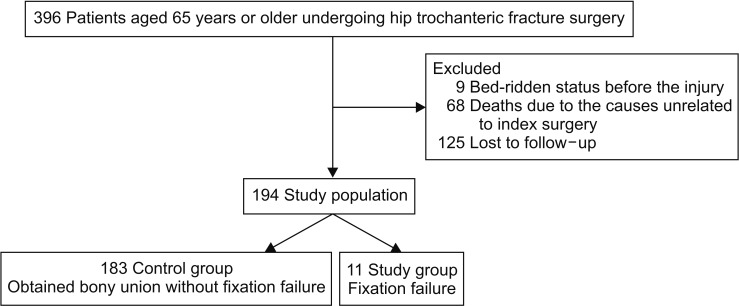
Fig. 1 Flowchart of patient inclusion and exclusion.
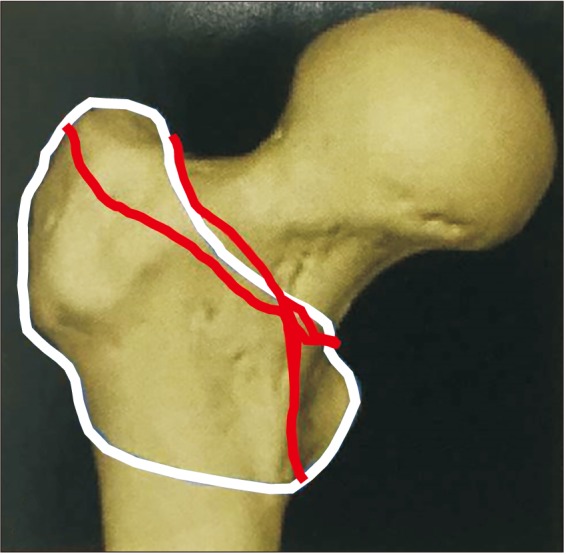
Fig. 2 Illustration of basicervical type of fracture on a computed tomographic scan. The continuous white line represents the area of typical trochanteric fractures and two interuppted gray lines represent the area of basicervical type of fractures.

Fig. 3 (A) An 88-year-old woman showed basicervical type of fracture with varus angulation before surgery. (B) The fracture was OTA A12 type fracture with greater trochanter comminution. (C) Surgery was performed by using Zimmer natural nail. (D) The lag screw was pulled out at 2 weeks after surgery. (E) The lag screw was cut out of the femoral head at 6 weeks after surgery.
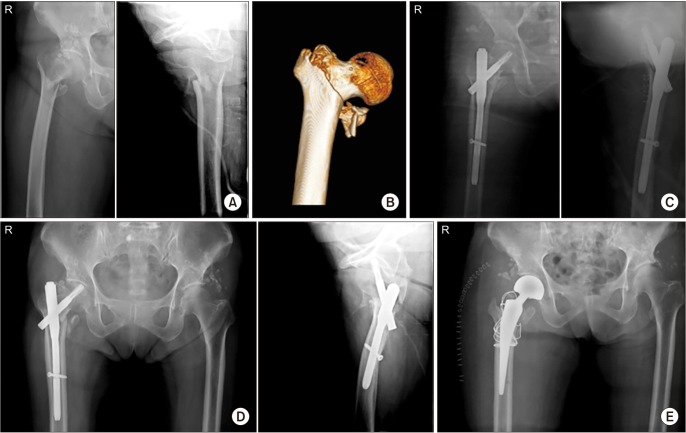
Fig. 4 (A) An 81-year-old woman fell on the ground. The proximal fragment was short and varus angulated before surgery. (B) The three-dimensional computed tomographic scan shows the OTA-A21 fracture. (C) The fracture was reduced by the Proximal Femoral Nail Anti-rotation. (D) The lag screw was cutting through at 3 months after surgery. (E) Conversion to hemiarthroplasty with wiring was performed.
Reference
-
1. Park SR, Kang JS, Kim HS, Lee WH, Kim YH. Treatment of intertrochanteric fracture with the Gamma AP locking nail or by a compression hip screw: a randomised prospective trial. Int Orthop. 1998; 22(3):157–160. PMID: 9728307.2. Eberle S, Bauer C, Gerber C, von Oldenburg G, Augat P. The stability of a hip fracture determines the fatigue of an intramedullary nail. Proc Inst Mech Eng H. 2010; 224(4):577–584. PMID: 20476505.
Article3. Ciufo DJ, Zaruta DA, Lipof JS, Judd KT, Gorczyca JT, Ketz JP. Risk factors associated with cephalomedullary nail cutout in the treatment of trochanteric hip fractures. J Orthop Trauma. 2017; 31(11):583–588. PMID: 28827502.
Article4. Bojan AJ, Beimel C, Taglang G, Collin D, Ekholm C, Jonsson A. Critical factors in cut-out complication after Gamma Nail treatment of proximal femoral fractures. BMC Musculoskelet Disord. 2013; 14:1. PMID: 23281775.
Article5. Davis TR, Sher JL, Horsman A, Simpson M, Porter BB, Checketts RG. Intertrochanteric femoral fractures: mechanical failure after internal fixation. J Bone Joint Surg Br. 1990; 72(1):26–31. PMID: 2298790.
Article6. Matre K, Vinje T, Havelin LI, et al. TRIGEN INTERTAN intramedullary nail versus sliding hip screw: a prospective, randomized multicenter study on pain, function, and complications in 684 patients with an intertrochanteric or subtrochanteric fracture and one year of follow-up. J Bone Joint Surg Am. 2013; 95(3):200–208. PMID: 23389782.7. Fogagnolo F, Kfuri M Jr, Paccola CA. Intramedullary fixation of pertrochanteric hip fractures with the short AOASIF proximal femoral nail. Arch Orthop Trauma Surg. 2004; 124(1):31–37. PMID: 13680275.
Article8. Bess RJ, Jolly SA. Comparison of compression hip screw and gamma nail for treatment of peritrochanteric fractures. J South Orthop Assoc. 1997; 6(3):173–179. PMID: 9322196.9. Butt MS, Krikler SJ, Nafie S, Ali MS. Comparison of dynamic hip screw and gamma nail: a prospective, randomized, controlled trial. Injury. 1995; 26(9):615–618. PMID: 8550169.
Article10. Baumgaertner MR, Curtin SL, Lindskog DM. Intramedullary versus extramedullary fixation for the treatment of intertrochanteric hip fractures. Clin Orthop Relat Res. 1998; (348):87–94. PMID: 9553538.
Article11. Evans EM. The treatment of trochanteric fractures of the femur. J Bone Joint Surg Br. 1949; 31B(2):190–203. PMID: 18150534.
Article12. Siddiqui SA, Rocco J, McKechnie A, Meyerson RI, Sands AK. Technique for percutaneous insertion of intramedullary nail for intertrochanteric hip fracture. Am J Orthop (Belle Mead NJ). 2004; 33(3):117–120. PMID: 15074458.13. Siegel RS. The value of the tip-apex distance in predicting failure of fixation of peritrochanteric fractures of the hip. J Bone Joint Surg Am. 1996; 78(9):1447.14. Cool P. The value of the tip-apex distance in predicting failure of fixation of peritrochanteric fractures of the hip. J Bone Joint Surg Am. 1996; 78(9):1447.15. Cleveland M, Bosworth DM, Thompson FR. Management of the trochanteric fracture of the femur. J Am Med Assoc. 1948; 137(14):1186–1190. PMID: 18871864.
Article16. Jung EY, Oh IT, Shim SY, Yoon BH, Sung YB. The effect of valgus reduction on the position of the blade of the proximal femoral nail antirotation in intertrochanteric hip fractures. Clin Orthop Surg. 2019; 11(1):36–42. PMID: 30838106.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- New Approach in the Treatment of Intertrochanteric Fracture Using a Cephalomedullary Nail
- Internal Fixation of Pauwels Type-3 Undisplacedincomplete Insufficiency Femoral Neck Fractures with Cephalomedullary Nails
- Treatment of Trochanteric Fractures of the Femur with Compression Hip Screw-Analysis of Factors associated with Failure of Fixation-
- Risk Factors Associated with Fixation Failure in Intertrochanteric Fracture Treated with Cephalomedullary Nail
- Clinical and Radiologic Outcome of Intertrochanteric Fracture Treatment Using TFNA (Trochanteric Fixation Nail-Advanced)
