Massive Hemorrhage Caused by a Non-Displaced Pubic Ramus Fracture from Low-Energy Trauma
- Affiliations
-
- 1Department of Orthopedic Surgery, Bundang Jesaeng Hospital, Seongnam, Korea. korsky21@hanmail.net
- KMID: 2469887
- DOI: http://doi.org/10.4055/jkoa.2019.54.6.557
Abstract
- Most low-energy pelvic ring fractures in elderly patients are treated conservatively so that an initial evaluation for complications such as vascular injury is usually overlooked. An 81-year-old female, who was taking regular aspirin, visited the emergency room and was diagnosed with a simple non-displaced pubic ramus fracture from a low-energy fall from standing, which was complicated by massive hemorrhage from the overlooked injury of the corona mortis. Elderly patients with pelvic ring fractures can have a delayed presentation of vascular injuries, regardless of the degree of displacement of the fractures, which highlights the need for a careful physical examination and close monitoring.
MeSH Terms
Figure
-

Figure 1 Anteroposterior pelvic radiograph showing a non-displaced left superior and inferior pubic ramus fracture without a posterior pelvic ring injury (arrows).
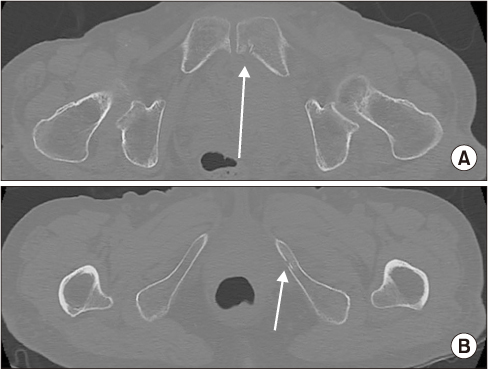
Figure 2 Axial pelvic bone computed tomography scan showing a non-displaced left superior (arrow) (A) and inferior (arrow) (B) pubic ramus fracture. No sacral fracture or sacroiliac joint widening was observed.

Figure 3 Contrast-enhanced axial pelvic computed tomography scan showing an active contrast extravasation adjacent fracture site (arrow). An approximately 12-cm-sized hematoma in the extraperitoneal space of left pelvic wall is seen.

Figure 4 Pelvic angiography with a left internal iliac angiogram showing active extravasation of contrast media from the corona mortis near the left pubic body fracture site (arrows).
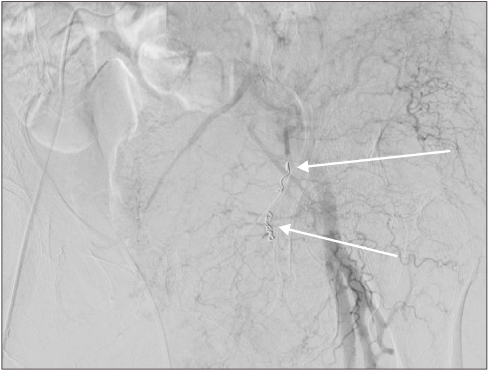
Figure 5 No active arterial bleeding was observed on the left internal iliac angiogram after successful embolization of the corona mortis (arrows).
Reference
-
1. Krappinger D, Kammerlander C, Hak DJ, Blauth M. Low-energy osteoporotic pelvic fractures. Arch Orthop Trauma Surg. 2010; 130:1167–1175.
Article2. Pick JW, Anson BJ, Ashley FL. The origin of the obturator artery: a study of 640 body-halves. Am J Anat. 1942; 70:317–343.
Article3. Henning P, Brenner B, Brunner K, Zimmermann H. Hemodynamic instability following an avulsion of the corona mortis artery secondary to a benign pubic ramus fracture. J Trauma. 2007; 62:E14–E17.
Article4. Solarz MK, Kistler JM, Rehman S. Obturator artery injury resulting in massive hemorrhage from a low-energy pubic ramus fracture. Orthopedics. 2017; 40:e546–e548.
Article5. Ten Broek RP, Bezemer J, Timmer FA, Mollen RM, Boekhoudt FD. Massive haemorrhage following minimally displaced pubic ramus fractures. Eur J Trauma Emerg Surg. 2014; 40:323–330.
Article6. Kong WM, Sun CK, Tsai IT. Delayed presentation of hypovolemic shock after a simple pubic ramus fracture. Am J Emerg Med. 2012; 30:2090.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Combined Injuries of Pubic Ramus Fracture : The Role of Computerized Tomography
- Stress Fractures in Pubic Bone: Report of 3 Cases
- Sequential Sacral Insufficiency Fracture After Unilateral Pubic Fractures: A Case Report
- Percutaneous Screw Fixation in a Displaced Pubic Fracture: Technical Note
- A roentgenographic study of the posterior urethral injury associated with pelvic bone fracture in male
