The ABCs of Voiding Cystourethrography
- Affiliations
-
- 1Department of Radiology, Chungbuk National University Hospital, Cheongju, Korea. youkio97@naver.com
- 2Department of Radiology, College of Medicine, Chungbuk National University, Cheongju, Korea.
- KMID: 2469185
- DOI: http://doi.org/10.3348/jksr.2020.81.1.101
Abstract
- Voiding cystourethrography (VCUG) demonstrates the anatomy of the urinary system and is used to detect the presence/absence of vesicoureteral reflux. It is the most important modality for urological fluoroscopic examination in children. For improved patient care, it is important to understand and perform VCUG appropriately. Therefore, an in-depth review of VCUG protocols and techniques has been presented herein. In addition, tips, tricks, and pitfalls associated with the technique have also been addressed.
Figure
-
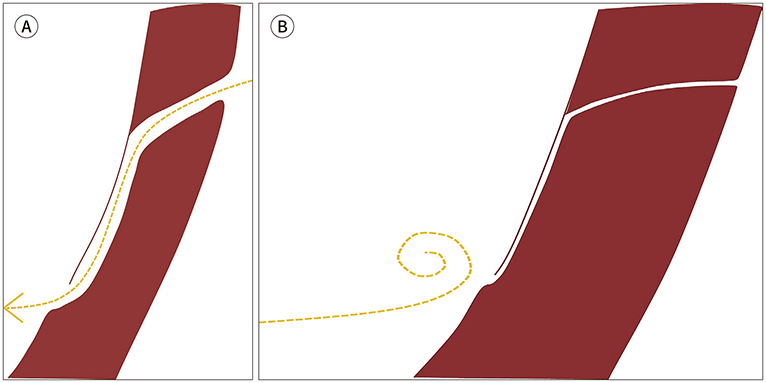
Fig. 1 Normal configuration of the vesicoureteral junction and antireflux action of the vesicoureteral reflux. A. Slanted entering and submucosal tunneling of the ureter of sufficient length is the normal configuration of the vesicoureteral junction. The yellow dotted line represents a downstream flow of the urine. B. The normal ureterovesical junction is closed during contracture on voiding by constriction and compression of the intramural ureter to protect the upper urinary tract from reflux, which is called the antireflux action of the vesicoureteral junction. The yellow dotted line represents a blocked urine flow without reflux.

Fig. 2 Psychological preparation necessary for both patients and parents.
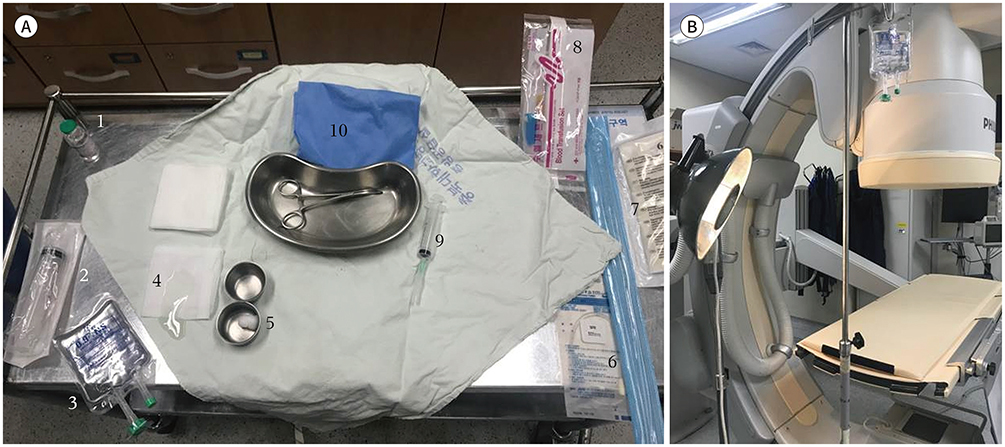
Fig. 3 Supplies for voiding cystourethrography. A. From the left upper corner in a counterclockwise direction: 1) iodine-containing contrast (300 or 350 mg/mL); 2) syringe for contrast mixing; 3) saline bag; 4) sterile lubricant gel; 5) chlorhexidine balls; 6) 5- and 8-French catheters; 7) sterile surgical gloves; 8) plastic extension tubing; 9) syringe for regurgitation of urine; and (10) sterile surgical drape with a hole. B. Warmer for maintaining the body temperature in young infants and light for better visibility during catheter insertion.

Fig. 4 Standardized evaluation of voiding cystourethrography in critical areas and conditions. A. AP projection of the urinary bladder in the early filling phase. B. AP projection of the urinary bladder in the late filling phase. C, D. Oblique projection of the urinary bladder focusing on the vesicoureteral junction. E. AP projection of the urinary bladder during voiding. F. Renal collecting system with and without the presence of reflux. G. AP projection of the urinary bladder after voiding. AP = anteroposterior

Fig. 5 Anteroposterior image of the urinary bladder demonstrating ureteroceles (arrow) in the early filling phase.
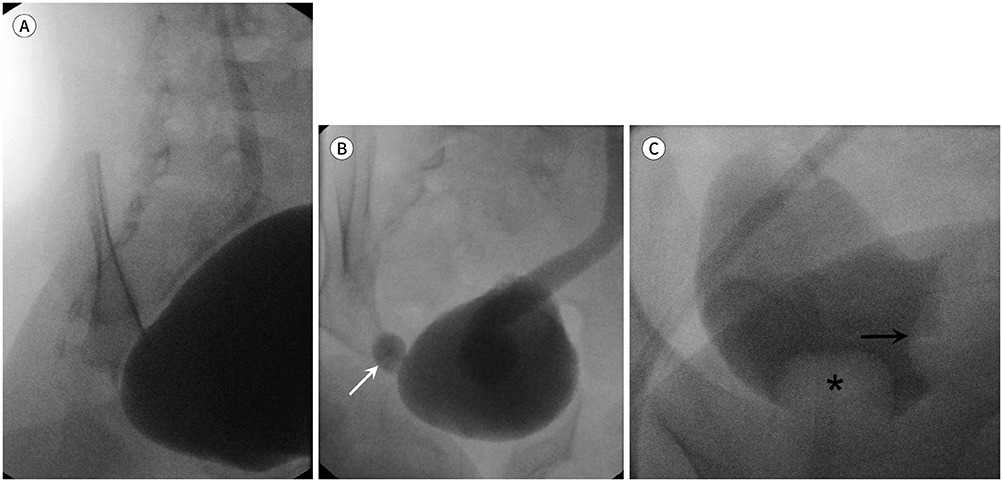
Fig. 6 Value of the oblique projection of the urinary bladder focusing on the vesicoureteral junction. A. The vesicoureteral reflux is well-demonstrated on oblique projection. B. The presence of ureteroceles with eversion (arrow) is well-demonstrated on oblique projection. C. The intravesical simple ureterocele (arrow) is well-demonstrated on oblique projection. The filling defect at the bladder apex (asterisk) is ballooning of the Foley catheter.
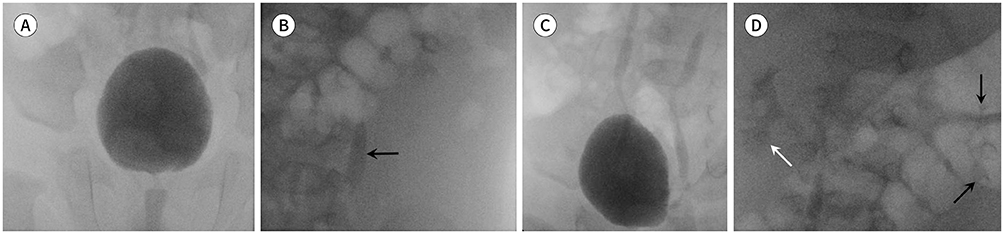
Fig. 7 Value of cyclic VCUG. A, B. Grade I (arrow, B) of the left VUR is demonstrated in the first session of VCUG. VUR is absent in the right urinary system. C, D. In the second session of VCUG, the left VUR grade changes from I to II (black arrows, D). The newly developed grade II of the right VUR (white arrow) is demonstrated. Finally, bilateral grade II VUR (white and black arrows) is demonstrated in the second session of VCUG. VCUG = voiding cystourethrography, VUR = vesicoureteral reflux

Fig. 8 Vesicoureteral reflux grade I. A. Vesicoureteral reflux grade I: ureter. B. The border of refluxed contrast is marked with yellow line.

Fig. 9 Vesicoureteral reflux grade II. A, B. Vesicoureteral reflux grade II: ureter, pelvis, and calyces; no dilatation; normal calyceal fornices.
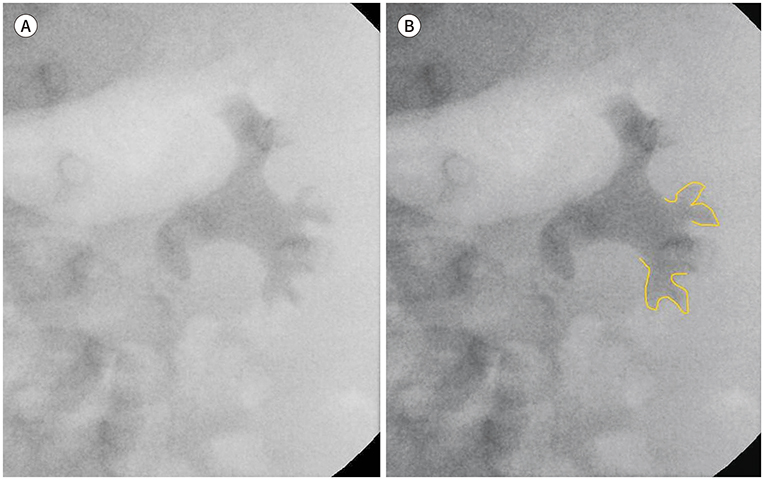
Fig. 10 Vesicoureteral reflux grade III. A, B. Vesicoureteral reflux grade III: mild to moderate dilatation and/or tortuosity of the ureter and mild to moderate dilatation of the renal pelvis; no or slight blunting of the fornices.
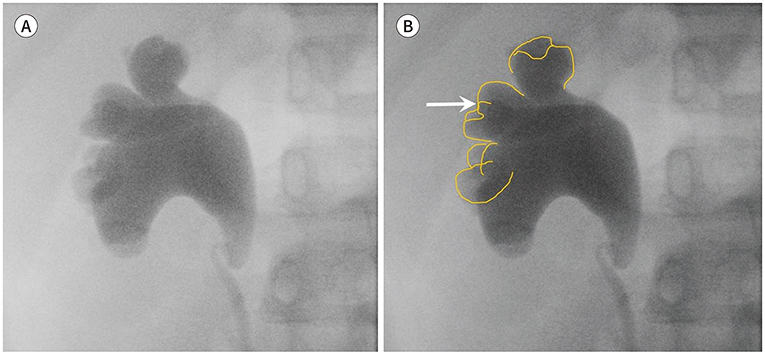
Fig. 11 Vesicoureteral reflux grade IV. A, B. Vesicoureteral reflux grade IV: moderate dilatation and/or tortuosity of the ureter and moderate dilatation of the renal pelvis and calyces; complete obliteration of the sharp angle of the fornices but maintenance of the papillary impressions (arrow, B) in most calyces.

Fig. 12 Vesicoureteral reflux grade V. A, B. Gross dilatation and tortuosity of the ureter and gross dilatation of the renal pelvis and calyces; papillary impressions are no longer visible in most calyces.
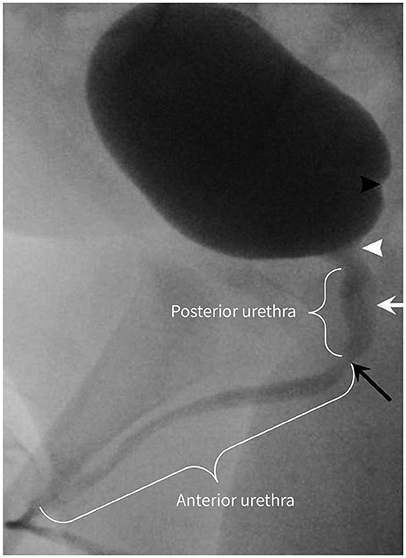
Fig. 13 Lateral anatomy of the urinary bladder and urethra. The interureteric ridge (black arrowhead) is the elevated border of the trigone toward the head. It is visible on lateral projection in approximately the distal one-quarter of the posteroinferior urinary bladder. The cone-shaped portion is the bladder neck (white arrowhead), which is continuous with the bladder apex. The elongated, faint filling defect below the bladder neck is the verumontanum (white arrow), which is the rounded eminence of the urethral crest in the posterior wall of the mid prostatic urethra. The shortest (about 1 cm long) and narrowest portion of the urethra is the membranous urethra (black arrow). The urethra is divided into the anterior and posterior urethra at the lower end of the membranous urethra; distal to the lower end of the membranous urethra is the anterior urethra, while proximal to the lower end of the membranous urethra is the posterior urethra.

Fig. 14 Low-pressure vesicoureteral reflux. The vesicoureteral reflux occurred in the early phase of bladder filling. Vesicoureteral reflux with low-pressure and early filling is associated with poor resolution and increased risk for acute pyelonephritis.
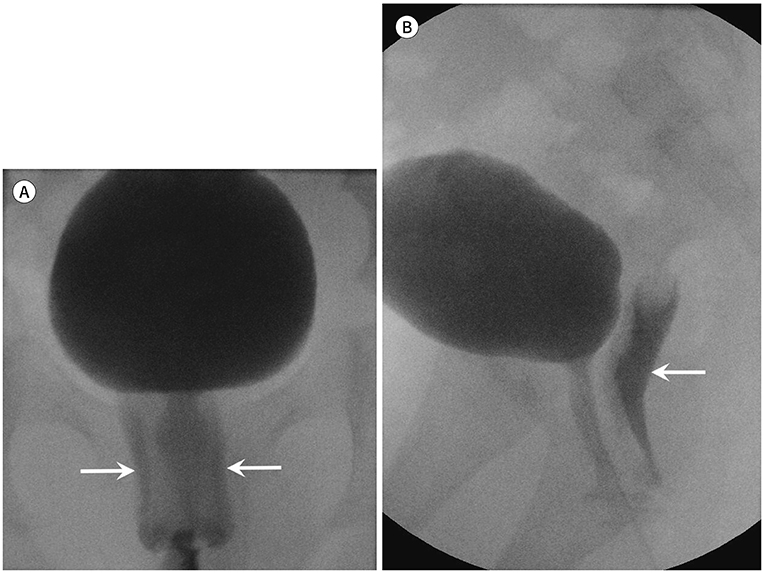
Fig. 15 Contrast reflux in the vagina. A, B. Contrast reflux in the vagina (arrows), which is common in girls during voiding, is noted on anteroposterior (A) and lateral (B) projections.

Fig. 16 Intra-renal reflux. The intra-renal reflux refers to the reflux of contrast in the renal papilla via the ducts of Bellini (arrows). It is not included in the international criteria for grading of vesicoureteral reflux; however, it should be described, as it is an important factor for renal scarring in ascending infection.

Fig. 17 Paraureteral (Hutch) diverticulum. Diverticulum at the ureterovesical junction is called the paraureteral or Hutch diverticulum (arrow). The vesicoureteral reflux is associated with the Hutch diverticulum. The vesicoureteral reflux from the Hutch diverticulum does not resolve without surgical correction and leaves causes renal scarring.
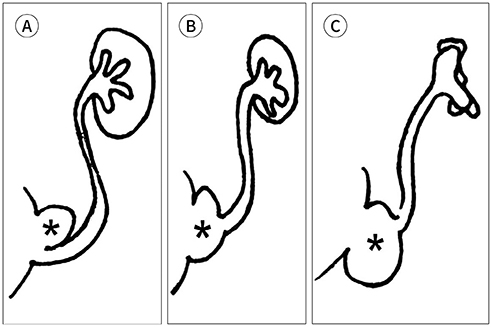
Fig. 18 Physiology and time course of the vesicoureteral reflux associated with the paraureteral diverticulum (asterisks). A. When the ureter opens on the rim of the diverticulum, and the bladder is completely distended, the ureteral orifice is incorporated transiently in the bladder diverticulum. B. When the ureter enters the diverticulum directly, the ureteral orifice is incorporated permanently in the bladder diverticulum. C. In both A and B, the antireflux ureterovesical mechanism is rendered incompetent and leads to secondary vesicoureteral reflux and endstage renal disease.

Fig. 19 Erroneous performance. A. Obtaining images without collimation. B. Obtaining excessive number of images (arrow) and taking excessive fluoroscopic time (arrowhead).

Fig. 20 Contrast diluted with the remaining urine. A. Although the contrast mixture was strictly made using the standard recipe, insufficient opacification of the contrast may be associated with dilution with the remaining urine in the bladder. B. Emptying the bladder through natural drainage or regurgitation with a syringe after the anchoring catheter renders sufficient opacification.
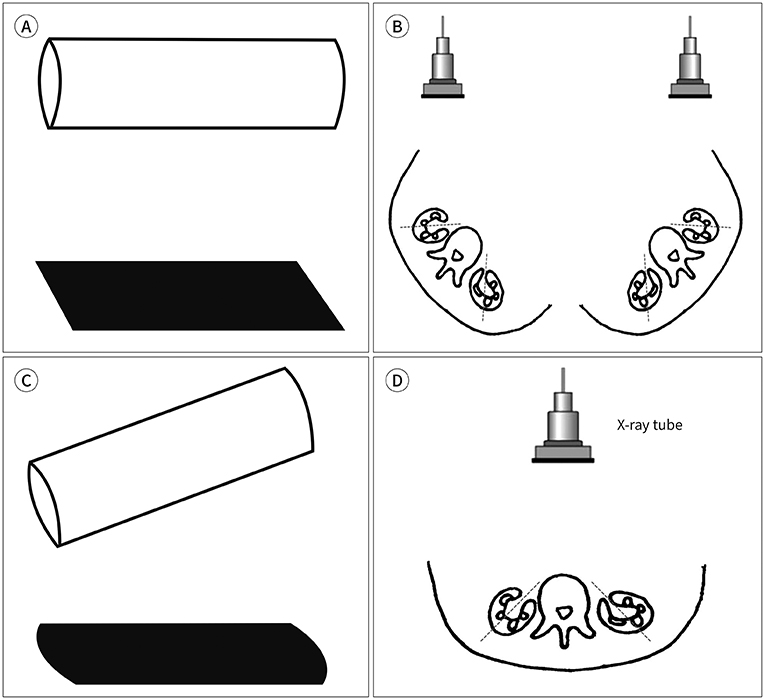
Fig. 21 Value of the orthographic projection and application on calyceal evaluation. A. In the orthographic projection, objects are represented on parallel projection to the principal axes. An accurate evaluation of the actual contour of objection is demonstrated by the orthogonal plane. B. The orthogonal plane for calyceal evaluation is tangential to the renal hilar axis, which is directed anteromedially. It is recommended to prepare the patient's body for the tangential projection of the expected renal hilum. C. The actual contour of the object can be altered using the oblique projection. D. Calyceal blunting can be distorted in the anteroposterior projection to the body which is oblique projection to calyces.
Reference
-
1. Kirks DR, Griscom NT. Practical pediatric imaging: diagnostic radiology of infants and children. 3rd ed. Philadelphia: Lippincott-Raven;1998. p. 1009–1160.2. Swischuk LE. Imaging of the newborn, infant, and young child. 5th ed. Philadelphia: Lippincott Williams & Wilkins;2004. p. 590–723.3. Coley BD. Caffey's pediatric diagnostic imaging. 12th ed. Philadelphia: Saunders;2013. p. 1243.4. American College of Radiology. ACR–SPR practice parameter for the performance of voiding cystourethrography in children. Accessed Jan 31, 2019. Available at. https://www.acr.org/-/media/ACR/Files/Practice-Parameters/VoidingCysto.pdf. Published 1995.5. Arena S, Iacona R, Impellizzeri P, Russo T, Marseglia L, Gitto E, et al. Physiopathology of vesico-ureteral reflux. Ital J Pediatr. 2016; 42:103.
Article6. Williams G, Fletcher JT, Alexander SI, Craig JC. Vesicoureteral reflux. J Am Soc Nephrol. 2008; 19:847–862.
Article7. Brereton RJ, Narayanan R, Ratnatunga C. Ureteric re-implantation in the neuropathic bladder. Br J Surg. 1987; 74:1107–1110.
Article8. Hernandez RJ, Goodsitt MM. Reduction of radiation dose in pediatric patients using pulsed fluoroscopy. AJR Am J Roentgenol. 1996; 167:1247–1253.
Article9. Hernanz-Schulman M, Goske MJ, Bercha IH, Strauss KJ. Pause and pulse: ten steps that help manage radiation dose during pediatric fluoroscopy. AJR Am J Roentgenol. 2011; 197:475–481.
Article10. Lachenmyer LL, Anderson JJ, Clayton DB, Thomas JC, Pope JC 4th, Adams MC, et al. Analysis of an intervention to reduce parental anxiety prior to voiding cystourethrogram. J Pediatr Urol. 2013; 9:1223–1228.
Article11. Riccabona M. Pediatric urogenital radiology-medical radiology. Diagnostic imaging. 3rd ed. New York: Springer International Publishing;2018. p. 20–23.12. Lebowitz RL, Olbing H, Parkkulainen KV, Smellie JM, Tamminen-Möbius TE. International system of radiographic grading of vesicoureteric reflux. International reflux study in children. Pediatr Radiol. 1985; 15:105–110.13. Ward VL. Patient dose reduction during voiding cystourethrography. Pediatr Radiol. 2006; 36 Suppl 2:168–172.
Article14. Domina JG, Sanchez R, Meesa IR, Christodoulou E. Evaluation of pediatric VCUG at an academic children’s hospital: is the radiographic scout image necessary? Pediatr Radiol. 2015; 45:855–861.
Article15. Paltiel HJ, Rupich RC, Kiruluta HG. Enhanced detection of vesicoureteral reflux in infants and children with use of cyclic voiding cystourethrography. Radiology. 1992; 184:753–755.
Article16. Papadopoulou F, Efremidis SC, Oiconomou A, Badouraki M, Panteleli M, Papachristou F, et al. Cyclic voiding cystourethrography: is vesicoureteral reflux missed with standard voiding cystourethrography? Eur Radiol. 2002; 12:666–670.
Article17. Wyly JB, Lebowitz RL. Refluxing urethral ectopic ureters: recognition by the cyclic voiding cystourethrogram. AJR Am J Roentgenol. 1984; 142:1263–1267.
Article18. Hodson CJ, Maling TM, McManamon PJ, Lewis MG. The pathogenesis of reflux nephropathy (chronic atrophic pyelonephritis). Br J Radiol. 1975; Suppl 13:1–26.19. Papachristou F, Printza N, Doumas A, Koliakos G. Urinary bladder volume and pressure at reflux as prognostic factors of vesicoureteral reflux outcome. Pediatr Radiol. 2004; 34:556–559.
Article20. Alexander SE, Arlen AM, Storm DW, Kieran K, Cooper CS. Bladder volume at onset of vesicoureteral reflux is an independent risk factor for breakthrough febrile urinary tract infection. J Urol. 2015; 193:1342–1346.
Article21. Snyder EM, Nguyen RA, Young KJ, Coley BD. Vesicovaginal reflux mimicking obstructive hydrocolpos. J Ultrasound Med. 2007; 26:1781–1784.
Article22. Maynard P. Drawing distinctions: the varieties of graphic expression. Ithaca: Cornell University Press;2005. p. 22.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Significance of Mild Fetal Pelviectasia and The Role of Postnatal Voiding Cystourethrography
- Significance of Bethanechol Chloride Induced Voiding Cystourethrography in the Detection of Subclinical Vesicoureteral Reflux
- A New Diagnostic Method for Urethral Stricture in Concomitant Retrograde and Voiding Cystourethrography Using Alpha Adrenoceptor Blocker
- Clinical Value of Voiding Cystourethrography in Complete Urethral Stricture
- Sensitivity of Transrectal Ultrasonography and Voiding Cystourethrography for Appearing of the Opening of Bladder Neck or External Sphincter
