Efficacy of Multidisciplinary Clinical Pathway for the Management of Postpartum Hemorrhage
- Affiliations
-
- 1Department of Obstetrics and Gynecology, Chonnam National University Medical School, Gwangju, Korea. kimyh@jnu.ac.kr
- KMID: 2468542
- DOI: http://doi.org/10.14734/PN.2019.30.4.214
Abstract
OBJECTIVE
To evaluate the efficacy of the clinical pathway known as the best linkage for expeditious expert decision (BLEED) system that we newly developed for the effective management of postpartum bleeding.
METHODS
This study was designed as a retrospective analysis. From January 2015 to May 2019, 155 patients who were treated for postpartum hemorrhage were included in our study. The non-BLEED group included 86 patients who admit with postpartum hemorrhage before the introduction of BLEED system, and the BLEED group included 69 patients who were applied with BLEED system. We compared the outcomes between two groups including duration of hospital stay and amount of transfusion.
RESULTS
Duration of hospital stay was shorter in BLEED group than in non-BLEED group (4.0±1.9 vs. 4.7±2.7 days, P < 0.05). Amount of red blood cell transfusion was less in BLEED group than in non-BLEED group (4.7±3.3 vs. 6.4±5.4 units, P < 0.05). There were no difference in clinical characteristics, initial laboratory value, time to get a blood transfusion between the two groups. There were no difference between the two groups in terms of management techniques, such as uterotonics, intrauterine balloon tamponade, pelvic artery embolization and cesarean hysterectomy.
CONCLUSION
BLEED system can be helpful method for the management of patients with postpartum hemorrhage.
Keyword
MeSH Terms
Figure
-

Fig. 1 Patient information check list. BP, blood pressure; BW, body weight; Ht, height; P/I, present illness; CS, caesarean section; VD, vaginal delivery; NPO, nothing by mouth; P/Hx, past history; PR, pulse rate; Hb, hemoglobin; ABO, ABO blood type.

Fig. 2 (A) Initial protocol when patient occurred. (B) Protocol when BLEED system activation after patient arrival. OB, obstetrics and gynecology; BLEED, best linkage for expeditious expert decision; IV, intra-venous; ER, emergency.
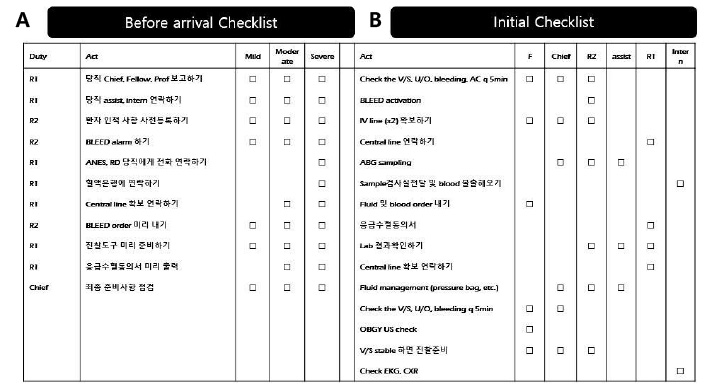
Fig. 3 (A) Before arrival check list. (B) Initial check list. BLEED, best linkage for expeditious expert decision; ANES, anesthesiology; RD, radiology; F, fellow; V/S, vital sign; U/O, urine output; AC, abdominal circumference; IV, intra-venous; ABG, arterial blood gas; OBGY, obstetrics and gynecology; US, ultrasonography; EKG, electrocardiography; CXR, chest x-ray.
Reference
-
1. Khan KS, Wojdyla D, Say L, Gülmezoglu AM, Van Look PF. WHO analysis of causes of maternal death: a systematic review. Lancet. 2006; 367:1066–1074.
Article2. Dildy GA 3rd. Postpartum hemorrhage: new management options. Clin Obstet Gynecol. 2002; 45:330–344.
Article3. Higgins S. Obstetric haemorrhage. Emerg Med (Fremantle). 2003; 15:227–231.
Article4. Pahlavan P, Nezhat C, Nezhat C. Hemorrhage in obstetrics andgynecology. Curr Opin Obstet Gynecol. 2001; 13:419–424.5. Mason BA. Postpartum hemorrhage and arterial embolization. Curr Opin Obstet Gynecol. 1998; 10:475–479.
Article6. Wise A, Clark V. Challenges of major obstetric haemorrhage. Best Pract Res Clin Obstet Gynaecol. 2010; 24:353–365.
Article7. Cameron CA, Roberts CL, Bell J, Fischer W. Getting an evidence-based post-partum haemorrhage policy into practice. Aust N Z J Obstet Gynaecol. 2007; 47:169–175.
Article8. Deneux-Tharaux C, Dupont C, Colin C, Rabilloud M, Touzet S, Lansac J, et al. Multifaceted intervention to decrease the rate of severe postpartum haemorrhage: the PITHAGORE6 cluster-randomised controlled trial. BJOG. 2010; 117:1278–1287.
Article9. Cho HY, Na S, Kim MD, Park I, Kim HO, Kim YH, et al. Implementation of a multidisciplinary clinical pathway for the management of postpartum hemorrhage: a retrospective study. Int J Qual Health Care. 2015; 27:459–465.
Article10. Seo K, Park MI, Kim SY, Park JS, Han YJ. Changes of maternal mortality ratio and the causes of death in Korea during 1995-2000. Korean J Obstet Gynecol. 2004; 47:2345–2350.11. Callaghan WM, Kuklina EV, Berg CJ. Trends in postpartum hemorrhage: United States, 1994-2006. Am J Obstet Gynecol. 2010; 202:353.e1–353.e16.
Article12. Knight M, Callaghan WM, Berg C, Alexander S, Bouvier-Colle MH, Ford JB, et al. Trends in postpartum hemorrhagein high resource countries: a review and recommendations from the International Postpartum Hemorrhage Collaborative Group. BMC Pregnancy Childbirth. 2009; 9:55.
Article13. Kang CS, Park SY, Lee JY, Oh JY, Ju WD, Kim SK, et al. Applicable indications and effectiveness of the selective arterial embolization in the management of obstetrical hemorrhage. Korean J Obstet Gynecol. 2004; 47:51–59.14. Gutierrez MC, Goodnough LT, Druzin M, Butwick AJ. Postpartum hemorrhage treated with a massive transfusion protocol at a tertiary obstetric center: a retrospective study. Int J Obstet Anesth. 2012; 21:230–235.
Article
