Comparison of Visual Acuity and Retinal Thickness According to Membranectomy in Idiopathic Epiretinal Membrane
- Affiliations
-
- 1Department of Ophthalmology, Soonchunhyang University Seoul Hospital, Soonchunhyang University College of Medicine, Korea. ckseek@naver.com
- KMID: 2468477
- DOI: http://doi.org/10.3341/jkos.2020.61.1.59
Abstract
- PURPOSE
To compare the visual acuity and retinal thickness in patients with an idiopathic epiretinal membrane (ERM) after vitrectomy and membranectomy using two different methods.
METHODS
This retrospective observational study included 77 eyes (32 eyes in the diamond-dusted membrane scraper [DDMS] group, and 45 eyes in the intraocular forceps [IOF] group) of 77 patients with idiopathic ERM who underwent pars plana vitrectomy and membranectomy. The main outcome measures were best-corrected visual acuity (BCVA, logMAR) and mean retinal thickness.
RESULTS
In the IOF group, the BCVA at postoperative 1 week was significantly lower than at baseline and had improved at 12 weeks after surgery. In the DDMS group, the BCVA at postoperative 1 week showed no significant difference at baseline and had improved at 4 weeks after surgery. The central macular thickness at postoperative 6 months was significantly lower than at baseline (all, p < 0.001); there was no significant difference between the two groups (p = 0.400). The postoperative macular thickness of the DDMS group was significantly lower than that of the IOF group in the inner inferior and outer inferior areas at postoperative 12 weeks and 4 weeks (p = 0.046 and p = 0.039, respectively). Five eyes of the DDMS group and 15 eyes of the IOF group developed cystoid macular edema, 14 eyes of that improved without treatment.
CONCLUSIONS
In patients with ERM, the use of DDMS or IOF for vitrectomy and membranectomy both resulted in improved visual acuity and decreased mean retinal thicknesses.
MeSH Terms
Figure
-

Figure 1 Early treatment of diabetic retinopathy study subfield. Sector 1: C0, Sector 2: IS, Sector 3: IN, Sector 4: II, Sector 5: IT, Sector 6: OS, Sector 7: ON, Sector 8: OI, Sector 9: OT. C0 = central fovea; IS = inner superior; IN = inner nasal; II = inner inferior; IT = inner temporal; OS = outer superior; ON = outer nasal; OI = outer inferior; OT = outer temporal.
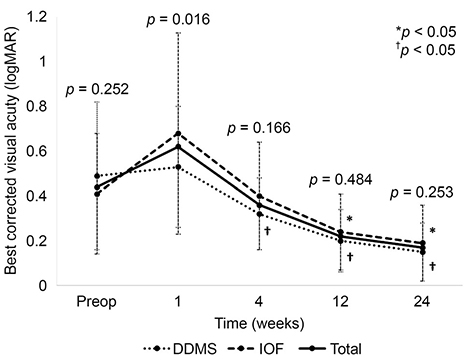
Figure 2 Preoperative and postoperative best corrected cisual acuity (BCVA, logMAR). BCVA in the DDMS groups were improved at postoperative 4 weeks, but BCVA in the IOF groups were deteriotating until postoperative 4 weeks and then improved at 12 weeks after surgery. LogMAR = logarithm of minimal angle of resolution; DDMS = diamond dusted membrane scraper; IOF = intraocular forcep. *,†p-value were analyzed by Wilcoxon singed rank test. Each postoperative BCVA were compared with preoperative BCVA.

Figure 3 Preoperative and postoperative best corrected cisual acuity (logMAR) by combined cataract surgery. (A) Patients of phakic eyes, vitrectomy combined cataract surgery. (B) Patients of pseudophakic eyes, only vitrectomy. p-value were analyzed by Mann-Whitney U test. DDMS = diamond dusted membrane scraper; IOF = intraocular forcep.
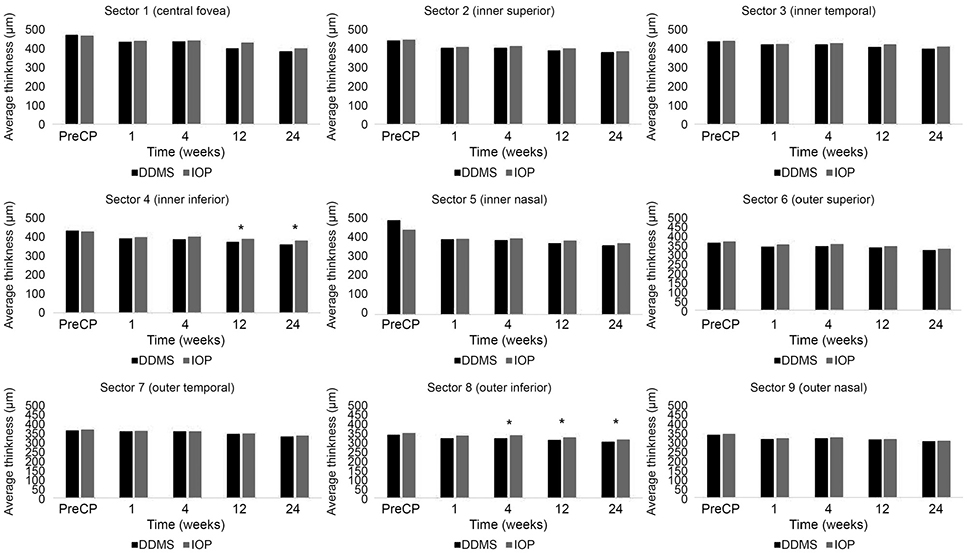
Figure 4 Average retinal thickness of early treatment of diabetic retinopathy study subfield (ETDRS) 9 sectors at preoperative and postoperative time. Preoperative mean retinal thickness was not significantly different between the two groups in all sectors of ETDRS. The averge retinal thickness in the sector 4 (inferior) was significantly lower in the diamond dusted membrane scraper (DDMS) group than in the intraocular forcep (IOF) group after 12 and 24 weeks postoperatively. The average retinal thickness at 4, 12, and 24 weeks after surgery was significantly lower in the DDMS group than in the IOF group. IOP = intraocular pressure. *p-value were analyzed by Mann Whitney U test. Each mean retinal thickness were compared DDMS group with IOF group.
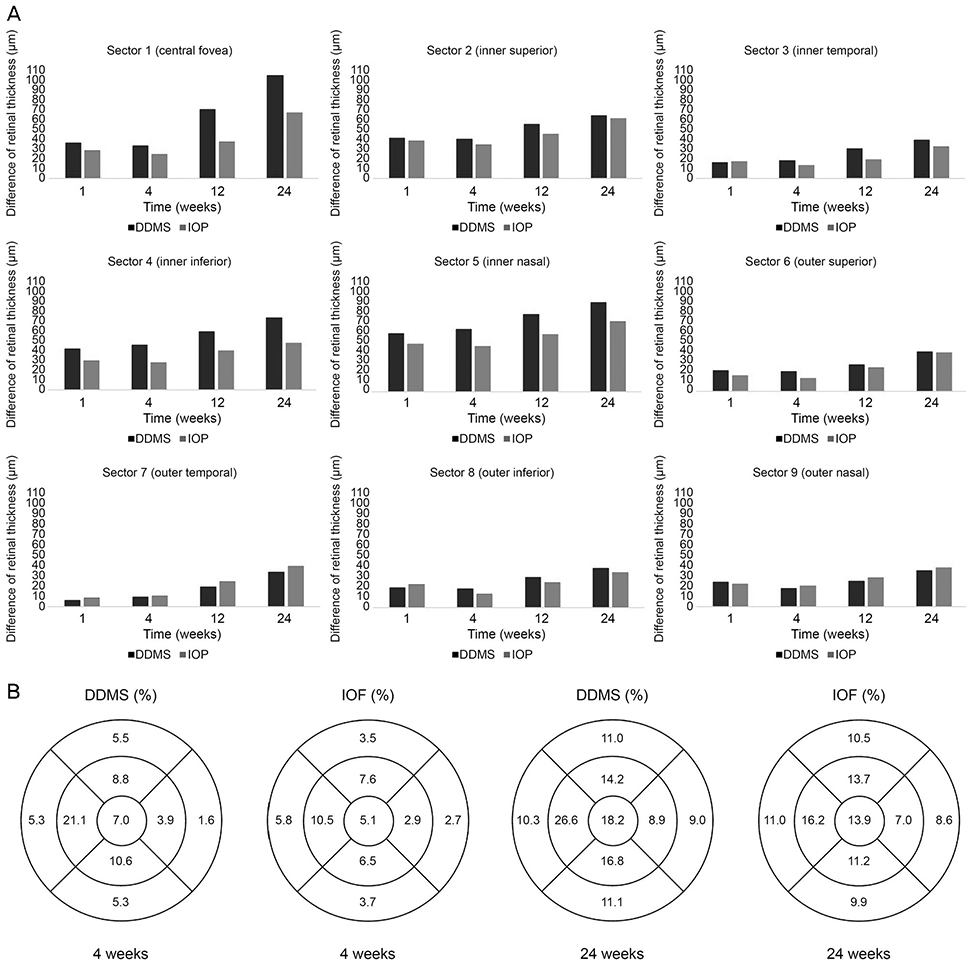
Figure 5 Difference of average retinal thckness of early treatment of diabetic retinopathy study subfield (ETDRS) 9 sectors compared preoperative time with each postoperative time. (A) The diamond dusted membrane scraper group showed more decrease than the intraocular forcep group in sector 1, 2, 3, 4, 5 and 6 postoperatively, but not significant statistically. (B) At 4, 12 weeks postoperatively, changes in retinal thickness were presented as a percentage of the ETDRS area. DDMS = diamond dusted membrane scraper; IOP = intraocular pressure; IOF = intraocular forcep.
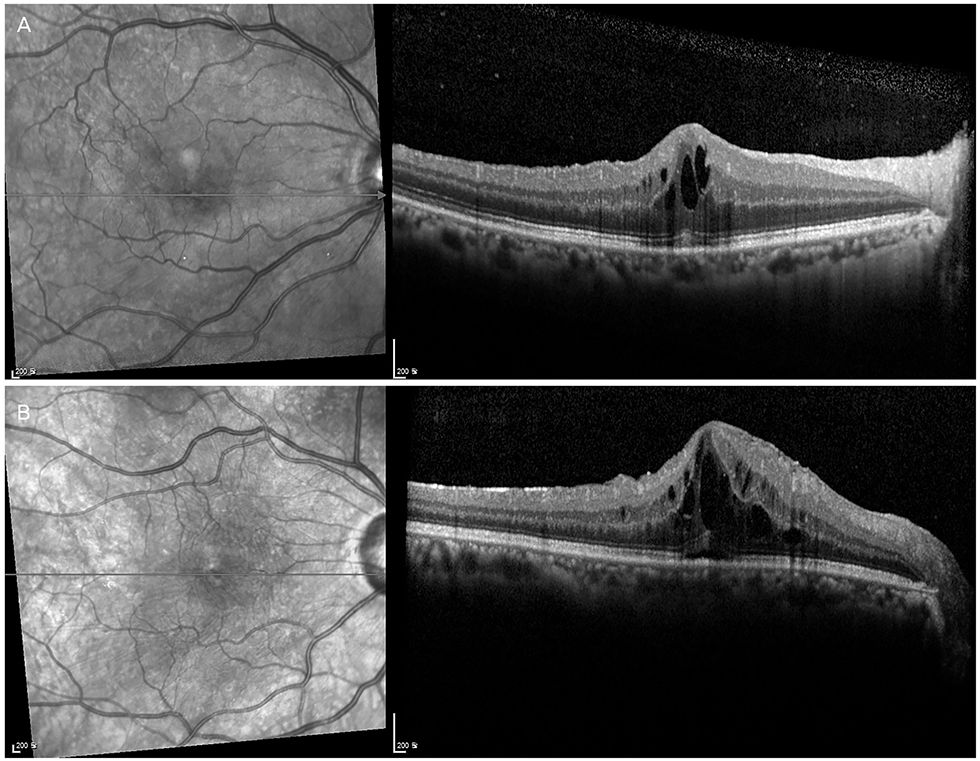
Figure 6 Postoperative optical coherence tomography finding of cystoid macular edema. (A) After 6 weeks, cystoid macular edema was developed in the diamond dusted membrane scraper groups. (B) After 6 weeks, cystoid macular edema was developed in the intraocular forcep groups.
Reference
-
1. Koutsandrea CN, Apostolopoulos MN, Alonistiotis DA, et al. Indocyanine green-assisted epiretinal membrane peeling evaluated by optical coherence tomography and multifocal electroretinography. Clin Ophthalmol. 2007; 1:535–544.2. Klein R, Klein BE, Wang Q, Moss SE. The epidemiology of epiretinal membranes. Trans Am Ophthalmol Soc. 1994; 92:403–425.3. Mitchell P, Smith W, Chey T, et al. Prevalence and associations of epiretinal membranes. The Blue Mountains Eye Study, Australia. Ophthalmology. 1997; 104:1033–1040.4. Machemer R. The surgical removal of epiretinal macular membranes (macular puckers) (author's transl). Klin Monbl Augenheilkd. 1978; 173:36–42.5. Margherio RR, Cox MS Jr, Trese MT, et al. Removal of epimacular membranes. Ophthalmology. 1985; 92:1075–1083.
Article6. McDonald HR, Verre WP, Aaberg TM. Surgical management of idiopathic epiretinal membranes. Ophthalmology. 1986; 93:978–983.
Article7. Yooh HS, Brooks HL Jr, Capone A Jr, et al. Ultrastructural features of tissue removed during idiopathic macular hole surgery. Am J Ophthalmol. 1996; 122:67–75.8. Kim TW, Song SJ, Chung H, Yu HG. Internal limiting membrane peeling in surgical treatment of macular epiretinal membrane. J Korean Ophthalmol Soc. 2005; 46:989–994.9. Park DW, Dugel PU, Garda J, et al. Macular pucker removal with and without internal limiting membrane peeling: pilot study. Ophthalmology. 2003; 110:62–64.
Article10. Kim SH, Chung JW, Chung H, Yu HG. Phacoemulsification and foldable intraocular lens implantation combined with vitrectomy and silicone oil tamponade for severe proliferative diabetic retinopathy. J Cataract Refract Surg. 2004; 30:1721–1726.
Article11. Kuhn F, Mester V, Berta A. The Tano Diamond Dusted Membrane Scraper: indications and contraindications. Acta Ophthalmol Scand. 1998; 76:754–755.
Article12. Hattenbach LO, Springer-Wanner C, Hoerauf H, et al. Intravitreal sustained-release steroid implants for the treatment of macular edema following surgical removal of epiretinal membranes. Ophthalmologica. 2017; 237:232–237.
Article13. Chylack LT Jr, Wolfe JK, Singer DM, et al. The Lens Opacities Classification System III. The Longitudinal Study of Cataract Study Group. Arch Ophthalmol. 1993; 111:831–836.14. Kawasaki R, Wang JJ, Mitchell P, et al. Racial difference in the prevalence of epiretinal membrane between Caucasians and Asians. Br J Ophthalmol. 2008; 92:1320–1324.
Article15. Kwok AK, Lai TY, Li WW, et al. Indocyanine green-assisted internal limiting membrane removal in epiretinal membrane surgery: a clinical and histologic study. Am J Ophthalmol. 2004; 138:194–199.
Article16. Sivalingam A, Eagle RC Jr, Duker JS, et al. Visual prognosis correlated with the presence of internal-limiting membrane in histopathologic specimens obtained from epiretinal membrane surgery. Ophthalmology. 1990; 97:1549–1552.17. Jang SY, Choi KS, Lee SJ. Remained macular edema after surgical treatment in patients with epiretinal membrane. J Korean Ophthalmol Soc. 2009; 50:1657–1660.
Article18. Lewis JM, Park I, Ohji M, et al. Diamond-dusted silicone cannula for epiretinal membrane separation during vitreous surgery. Am J Ophthalmol. 1997; 124:552–554.
Article19. Ray S, D'Amico DJ. Pseudophakic cystoid macular edema. Semin Ophthalmol. 2002; 17:167–180.
Article20. Kim SJ, Martin DF, Hubbard GB 3rd, et al. Incidence of postvitrectomy macular edema using optical coherence tomography. Ophthalmology. 2009; 116:1531–1537.
Article21. Johnson MW. Tractional cystoid macular edema: a subtle variant of the vitreomacular traction syndrome. Am J Ophthalmol. 2005; 140:184–192.
Article22. Johnson MW. Etiology and treatment of macular edema. Am J Ophthalmol. 2009; 147:11–21.
Article23. Hattenbach LO, Kuhli-Hattenbach C, Springer C, et al. Intravitreal dexamethasone implant for treatment of persistent postoperative macular edema after vitrectomy. Ophthalmologe. 2016; 113:581–588.24. Klamann A, Böttcher K, Ackermann P, et al. Intravitreal dexamethasone implant for the treatment of postoperative macular edema. Ophthalmologica. 2016; 236:181–185.
Article25. Miyake K, Ibaraki N. Prostaglandins and cystoid macular edema. Surv ophthalmology. 2002; 47 Suppl 1:S203–S218.
Article26. Xu H, Chen M, Forrester JV, Lois N. Cataract surgery induces retinal pro-inflammatory gene expression and protein secretion. Invest Ophthalmol Vis Sci. 2011; 52:249–255.
Article27. Tranos PG, Wickremasinghe SS, Stangos NT, et al. Macular edema. Surv ophthalmology. 2004; 49:470–490.
Article28. Arevalo JF, Maia M, Garcia-Amaris RA, et al. Intravitreal bevacizumab for refractory pseudophakic cystoid macular edema: the Pan-American Collaborative Retina Study Group results. Ophthalmology. 2009; 116:1481–1487. 1487.e129. Daruich A, Matet A, Moulin A, et al. Mechanisms of macular edema: beyond the surface. Prog Retin Eye Res. 2018; 63:20–68.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Analysis of Leading Diseases Causing Epiretinal Membrane and Comparison of Prognosis after Epiretinal Membrane Peeling
- The Thickness of Each Retinal Layer and Visual Acuity after Vitrectomy in Idiopathic Epiretinal Membrane
- Evaluation of Each Retinal Layer Thickness According to Preoperative OCT Patterns after Idiopathic ERM Removal
- Spontaneous Disappearance of A Traumatic Macular Hole
- Long-Term Changes in Visual Acuity and Foveal Thickness after Vitrectomy for Idiopathic Epiretinal Membrane
