Clinical Significance of beta-Tricalcium Phosphate and Polyphosphate for Mastoid Cavity Obliteration during Middle Ear Surgery: Human and Animal Study
- Affiliations
-
- 1Department of Otolaryngology, Ajou University School of Medicine, Suwon, Korea. yhc@ajou.ac.kr
Abstract
OBJECTIVES
Mastoid obliteration is used to obliterate the mastoid cavity following a mastoidectomy or to prevent the formation of a retraction pocket. This study evaluated the effectiveness of beta-tricalcium phosphate and polyphosphate (beta-TPP) for mastoid obliteration in middle ear surgeries in prospective human and animal studies.
METHODS
Twenty patients with chronic otitis media underwent mastoid obliteration using beta-TPP after a intact canal wall mastoidectomy or simple mastoidectomy. The clinical data were prospectively evaluated including: the diagnosis, temporal bone computed tomography (TBCT), otoscopic findings, pure tone audiogram, and complications. In the animal experiment, beta-TPP was applied into the right bulla in five rats, and the opposite bulla was used as the control in the non-obliterated state. The skulls of five other rats were drilled out and the holes were obliterated with beta-TPP. TBCT were obtained at 3, 6, and 9 months after the obliteration and histologic analysis was done at 3 and 9 months after surgery.
RESULTS
In the human study, fourteen TBCTs were obtained at 12 months after the surgery. All demonstrated no bone resorption in the obliterated mastoids. Among the 15 cases displaying retracted tympanic membranes preoperatively, 11 showed no retraction, 2 showed retraction postoperatively, 1 was lost to follow-up and 1 was a case of postoperative wound infection. Among 20 cases, one case developed a postoperative infection that necessitated a second operation. Sixteen underwent ossiculoplasty; hearing improvements were obtained in 15 cases and 1 case showed decreased hearing. In the animal study, new bone formation without significant bone resorption in the radiologic and histologic findings were noted in both the skull and bulla groups.
CONCLUSION
Although beta-TPP is a foreign material having the possibility of infection, mastoid obliteration with it can be a treatment option in middle ear surgeries to prevent retraction pockets or the recurrence of diseases.
MeSH Terms
Figure
-

Fig. 1 Surgical techniques of mastoid obliteration using PolyBone®. (A) Inflammatory tissues in the mastoid cavity were completely removed. (B) The mastoid cavity was obliterated with PolyBone®. (C) PolyBone® in the mastoid cavity was covered with a harvested autologous bone pate.
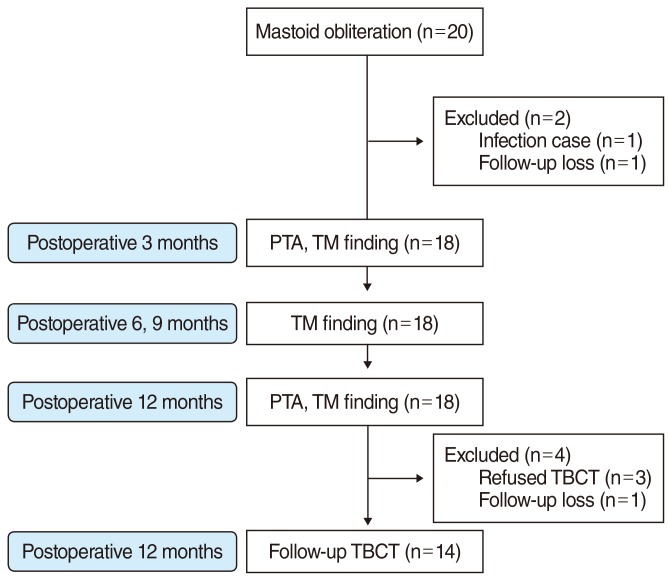
Fig. 2 The human study flow diagram. PTA, pure tone audiometry; TM, tympanic membrane.
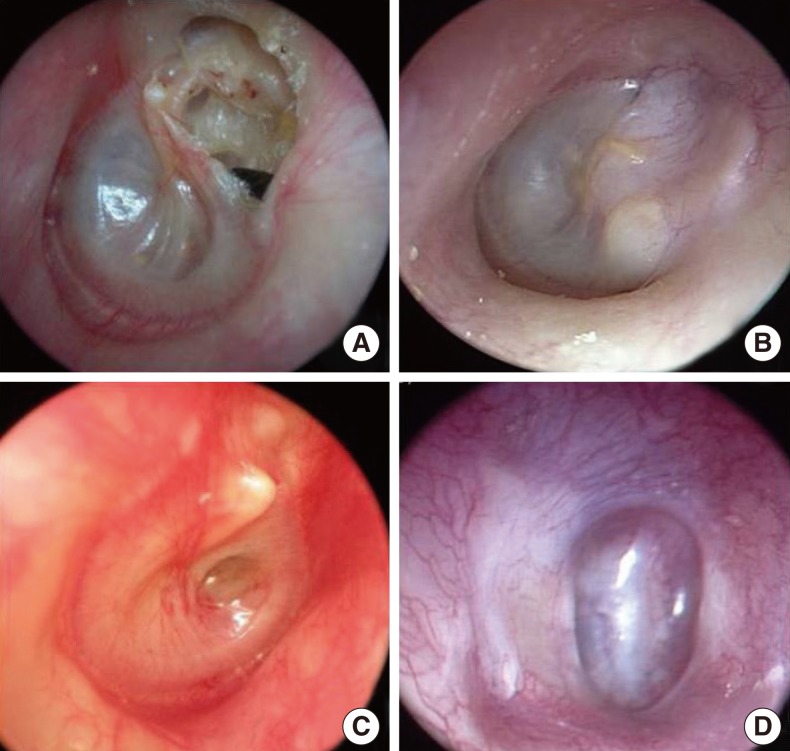
Fig. 3 Preoperative and postoperative tympanic membrane (TM) otoscopic findings. (A) Attic destruction was noted in preoperative TM findings (case 1). (B) No retraction in postoperative TM findings (case 1). (C) A retraction pocket was noted in preoperative TM findings (case 4). (D) The retraction pocket had recurred in postoperative TM findings (case 4).
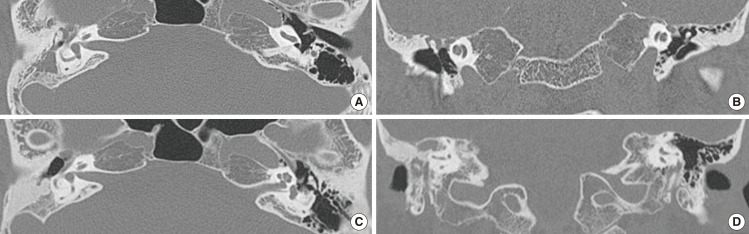
Fig. 4 Temporal bone computed tomography (CT) before and 12 months after the operation in case 6. The preoperative CT (A, axial; B, coronal) showed mastoid hazziness in the right side. Images obtained at 12 months after surgery (C, axial; D, coronal) demonstrated high density which suggested that the PolyBone® graft remained in the right obliterated mastoid area.

Fig. 5 Complications in case 10. In the intraoperative finding, a wet middle ear mucosa was noted. (A) We blocked the aditus ad antrum with an autologous bone pate, gelfoam and glue. (B) The mastoid cavity was obliterated with PolyBone® and covered with a bone pate. (C, D) However, operation site swelling and otorrhea were found on postoperative day 5. We performed a canal wall down mastoidectomy on postoperative day 10.
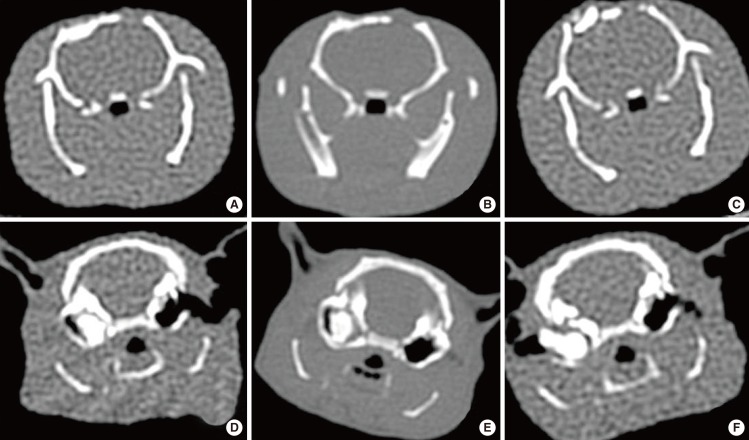
Fig. 6 Computed tomography (CT) images of the skull and bulla at 3, 6, and 9 months after obliteration in the animal study. A-C are coronal views obtained from of the same rat in the skull group, and D-F are from the same rat in the bulla group. After drillings were done in both sides, PolyBone® grafts were performed in only the right side. CT images demonstrated high density in only right side, suggesting no bone resorption in the right skull and bulla at 3, 6, and 9 months after obliteration. However, there was no change in the left side skull and bulla (control side). (A, D) Three months after obliteration, (B, E) 6 months after obliteration, (C, F) 9 months after obliteration.
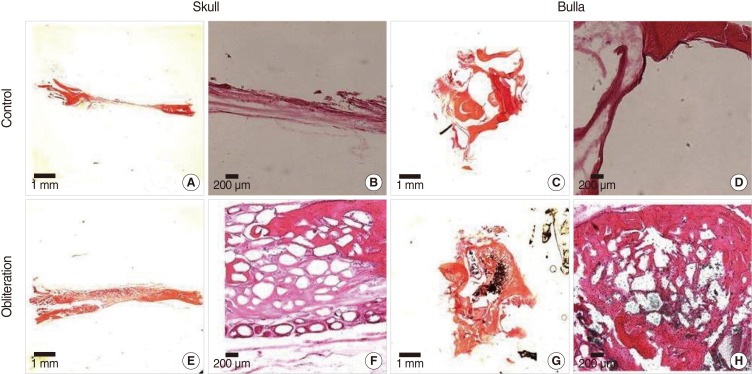
Fig. 7 Histopathologic findings in the skull and bulla at 9 months after obliteration in the animal study. In the control group (A-D), there was no new bone formation. In contrast, active new bone formation was seen without inflammatory infiltration around the implantation field in the PolyBone® graft group (E-H), (H&E, A, C, E, and G, ×12.5; B, D, F, and H, ×40).
Reference
-
1. Palva T, Virtanen H. Ear surgery and mastoid air cell system. Arch Otolaryngol. 1981; 2. 107(2):71–73. PMID: 7469894.
Article2. Lee WS, Choi JY, Song MH, Son EJ, Jung SH, Kim SH. Mastoid and epitympanic obliteration in canal wall up mastoidectomy for prevention of retraction pocket. Otol Neurotol. 2005; 11. 26(6):1107–1111. PMID: 16272924.
Article3. Palmgren O. Long-term results of open cavity and tympanomastoid surgery of the chronic ear. Acta Otolaryngol. 1979; 88(5-6):343–349. PMID: 532609.
Article4. Merifield DO. Obliteration of the mastoid segment: a clinical review and pilot study of various transplant materials. Ann Otol Rhinol Laryngol. 1963; 3. 72:157–190. PMID: 13934989.5. Solomons NB, Robinson JM. Obliteration of mastoid cavities using bone pate. J Laryngol Otol. 1988; 9. 102(9):783–784. PMID: 3171368.6. Lenis A. Hydroxylapatite canal wall reconstruction in patients with otologic dilemmas. Am J Otol. 1990; 11. 11(6):411–414. PMID: 2178321.7. Committee on Hearing and Equilibrium guidelines for the evaluation of results of treatment of conductive hearing loss. American Academy of Otolaryngology-Head and Neck Surgery Foundation, Inc. Otolaryngol Head Neck Surg. 1995; 9. 113(3):186–187. PMID: 7675477.8. Palva T. Operative technique in mastoid obliteration. Acta Otolaryngol. 1973; 4. 75(4):289–290. PMID: 4702622.
Article9. Gantz BJ, Wilkinson EP, Hansen MR. Canal wall reconstruction tympanomastoidectomy with mastoid obliteration. Laryngoscope. 2005; 10. 115(10):1734–1740. PMID: 16222186.
Article10. Shea MC Jr, Gardner G Jr, Simpson ME. Mastoid obliteration using homogenous bone chips and autogenous bone paste. Trans Am Acad Ophthalmol Otolaryngol. 1972; Jan-Feb. 76(1):160–172. PMID: 4337026.11. Black B. Mastoidectomy elimination: obliterate, reconstruct, or ablate? Am J Otol. 1998; 9. 19(5):551–557. PMID: 9752959.12. Dornhoffer JL. Surgical modification of the difficult mastoid cavity. Otolaryngol Head Neck Surg. 1999; 3. 120(3):361–367. PMID: 10064639.
Article13. Meurman Y, Ojala L. Primary reduction of a large operation cavity in radical mastoidectomy with a muscle-periosteal flap. Acta Otolaryngol. 1949; 6. 37(3):245–252. PMID: 15396404.
Article14. Palva T, Palva A, Karja J. Musculoperiosteal flap in cavity obliteration: histopathological study seven years postoperatively. Arch Otolaryngol. 1972; 2. 95(2):172–177. PMID: 5060065.
Article15. Thomas Rambo JH. Further experience with musculoplasty. AMA Arch Otolaryngol. 1960; 71(3):428–436.16. Cho SW, Cho YB, Cho HH. Mastoid obliteration with silicone blocks after canal wall down mastoidectomy. Clin Exp Otorhinolaryngol. 2012; 3. 5(1):23–27. PMID: 22468198.
Article17. Minoda R, Hayashida M, Masuda M, Yumoto E. Preliminary experience with beta-tricalcium phosphate for use in mastoid cavity obliteration after mastoidectomy. Otol Neurotol. 2007; 12. 28(8):1018–1021. PMID: 17898672.18. Goldenberg RA. Hydroxylapatite ossicular replacement prostheses: preliminary results. Laryngoscope. 1990; 7. 100(7):693–700. PMID: 2163478.19. Grote JJ. Reconstruction of the ossicular chain with hydroxyapatite implants. Ann Otol Rhinol Laryngol Suppl. 1986; Mar-Apr. 123:10–12. PMID: 3083755.
Article20. Estrem SA, Highfill G. Hydroxyapatite canal wall reconstruction/mastoid obliteration. Otolaryngol Head Neck Surg. 1999; 3. 120(3):345–349. PMID: 10064636.
Article21. Ambard AJ, Mueninghoff L. Calcium phosphate cement: review of mechanical and biological properties. J Prosthodont. 2006; Sep-Oct. 15(5):321–328. PMID: 16958734.
Article22. Lee HS, Cho YS, Chung WH, Lee SR, Chung J, Hong SH. Obliteration of the temporal dorsal bullae of guinea pigs using hydroxyapatite granules (Bongros®): a radiological and histological study. Korean J Otorhinolaryngol-Head Neck Surg. 2009; 1. 52(1):14–18.
Article23. Takahashi S, Nakano Y. A morphological study on obliteration of the temporal dorsal bullae using hydroxyapatite granules. Am J Otol. 1996; 3. 17(2):197–199. PMID: 8723945.24. Kveton JF, Friedman CD, Costantino PD. Indications for hydroxyapatite cement reconstruction in lateral skull base surgery. Am J Otol. 1995; 7. 16(4):465–469. PMID: 8588646.25. Mahendran S, Yung MW. Mastoid obliteration with hydroxyapatite cement: the Ipswich experience. Otol Neurotol. 2004; 1. 25(1):19–21. PMID: 14724486.
Article26. Lee WS, Kim SH, Lee WS, Kim SH, Moon IS, Byeon HK. Canal wall reconstruction and mastoid obliteration in canal wall down tympanomastoidectomized patients. Acta Otolaryngol. 2009; 9. 129(9):955–961. PMID: 19153845.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Effect on Acoustic Characteristics of Surgical Modification of the External Ear
- Magnetic Resonance Imaging of the Mastoid Cavity and the Middle Ear: Prevalence and Clinical Significance of Incidental Abnormal Findings in a Non-ENT Adult and Pediatric Population
- The Effect of Mastoid Obliteration Technique Using Superiorly Based Musculoperiosteal Flap and Autologous Conchal Cartilage
- Postoperative Mastoid Aeration Following Canal Wall Up Mastoidectomy according to Preoperative Middle Ear Disease: Analysis of Temporal Bone Computed Tomography Scans
- Outcomes of Modified Canal Wall Down Mastoidectomy and Mastoid Obliteration Using Autologous Materials
