Time Course of Functional Recovery in Takotsubo (Stress) Cardiomyopathy: A Serial Speckle Tracking Echocardiography and Electrocardiography Study
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Samsung Changwon Hospital, Sungkyunkwan University School of Medicine, Changwon, Korea. conatuse@gmail.com
- KMID: 2468381
- DOI: http://doi.org/10.4250/jcvi.2019.0083
Abstract
- BACKGROUND
Although rapid recovery of cardiac contraction is a hallmark of Takotsubo cardiomyopathy (TTC), the time course of recovery is still ill-defined. We aimed to investigate the time course of left ventricular (LV) functional recovery using 2D speckle tracking echocardiography and electrocardiography (ECG).
METHODS
Thirty-two consecutive patients (65 ± 16 years, 26 women) with TTC were prospectively recruited. ECG and echocardiography were performed at baseline (No. 1), before discharge (No. 2), and at 1 week (No. 3) and 5 weeks (No. 4) after discharge. Echocardiographic images and ECGs were analyzed to measure ejection fraction (LVEF), global and regional longitudinal strain (GLS, RLS), and T wave inversion (TWI) scores.
RESULTS
At baseline, LVEF, GLS, and TWI score were 39 ± 8.8%, -11 ± 4.3%, and 1.8 ± 3.0, respectively. Both LVEF and GLS continued to improve from baseline at the No. 2, No. 3, and No. 4 timepoints (49 ± 9.3%, 56 ± 7.5%, 58 ± 6.8%, respectively, for LVEF and -15 ± 4.2%, -17 ± 3.9%, -19 ± 3.4%, respectively, for GLS). TWI score was decreased at the No. 3 ECG relative to baseline and then increased (No. 2: -2.5 ± 3.0, No. 3: -2.9 ± 5.2, No. 4: -0.3 ± 4.4). In the apical subgroup, the reverse base-to-apex gradient of RLS had disappeared by the No. 3 echocardiography.
CONCLUSIONS
Contractile function as assessed by LVEF and GLS recovered continuously in patients with TTC throughout the acute and subacute phases, with rapid recovery in the acute phase. Negative T wave progressed during the acute phase and recovered more slowly during the subacute phase.
MeSH Terms
Figure
-
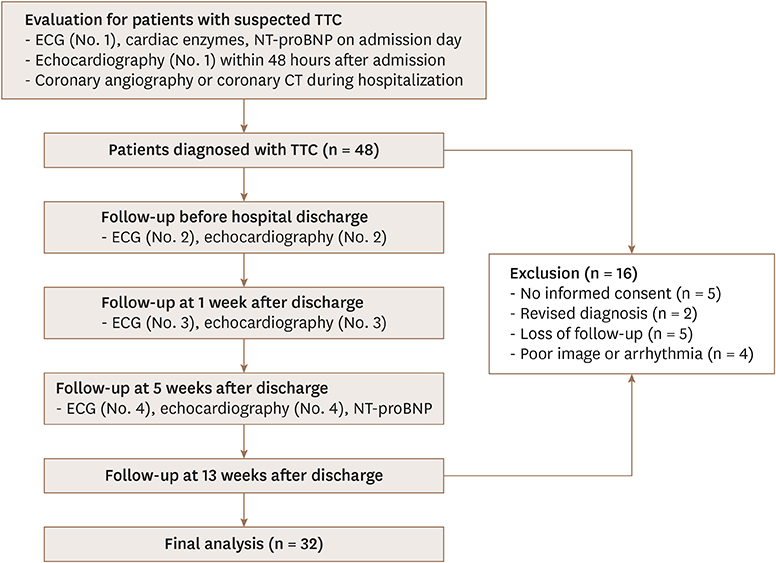
Figure 1 Study flow-chart. CT: computed tomography, ECG: electrocardiography, NT-proBNP: N-terminal prohormone brain natriuretic peptide, TTC: Takotsubo cardiomyopathy.

Figure 2 Representative bull's eye mapping images of serial longitudinal peak systolic strain and electrocardiography (ECG) in patients with apical type (upper panel) or non-apical type (lower panel) Takotsubo cardiomyopathy. The No. 1 ECG was recorded on admission and the No. 1 bull's-eye map were recorded on day 2 in the upper panel, while the No. 1 ECG and bull's-eye map were recorded on the same day in the lower panel. All No. 2 - 4 bull' eye maps and ECGs were recorded on the same day. Only precordial lead results are shown in the ECG images.

Figure 3 Serial ejection fraction (A), global longitudinal peak systolic strain (B), and T wave inversion score (C) in all study patients (n = 32). T wave inversion score in apical (D) (n = 20) and non-apical type (E) (n = 12).
Reference
-
1. Templin C, Ghadri JR, Diekmann J, et al. Clinical features and outcomes of Takotsubo (stress) cardiomyopathy. N Engl J Med. 2015; 373:929–938.2. Medeiros K, O'Connor MJ, Baicu CF, et al. Systolic and diastolic mechanics in stress cardiomyopathy. Circulation. 2014; 129:1659–1667.
Article3. Gianni M, Dentali F, Grandi AM, Sumner G, Hiralal R, Lonn E. Apical ballooning syndrome or takotsubo cardiomyopathy: a systematic review. Eur Heart J. 2006; 27:1523–1529.
Article4. Scally C, Rudd A, Mezincescu A, et al. Persistent long-term structural, functional, and metabolic changes after stress-induced (Takotsubo) cardiomyopathy. Circulation. 2018; 137:1039–1048.
Article5. Nowak R, Fijalkowska M, Gilis-Malinowska N, et al. Left ventricular function after takotsubo is not fully recovered in long-term follow-up: A speckle tracking echocardiography study. Cardiol J. 2017; 24:57–64.
Article6. Kobayashi Y, Okura H, Kobayashi Y, Fukuda S, Hirohata A, Yoshida K. Left ventricular myocardial function assessed by three-dimensional speckle tracking echocardiography in Takotsubo cardiomyopathy. Echocardiography. 2017; 34:523–529.
Article7. Heggemann F, Weiss C, Hamm K, et al. Global and regional myocardial function quantification by two-dimensional strain in Takotsubo cardiomyopathy. Eur J Echocardiogr. 2009; 10:760–764.
Article8. Mansencal N, Abbou N, Pillière R, El Mahmoud R, Farcot JC, Dubourg O. Usefulness of two-dimensional speckle tracking echocardiography for assessment of Tako-Tsubo cardiomyopathy. Am J Cardiol. 2009; 103:1020–1024.
Article9. Geyer H, Caracciolo G, Abe H, et al. Assessment of myocardial mechanics using speckle tracking echocardiography: fundamentals and clinical applications. J Am Soc Echocardiogr. 2010; 23:351–369. quiz 453-5.
Article10. Kosuge M, Ebina T, Hibi K, et al. Differences in negative T waves between takotsubo cardiomyopathy and reperfused anterior acute myocardial infarction. Circ J. 2012; 76:462–468.
Article11. Mugnai G, Vassanelli F, Pasqualin G, et al. Dynamic changes of repolarization abnormalities in takotsubo cardiomyopathy. Acta Cardiol. 2015; 70:225–232.
Article12. Ishigaki D, Okuyama H, Yuki K, et al. Serial evaluation of left ventricular contraction and relaxation in Takotsubo cardiomyopathy by 2D speckle tracking echocardiography. J Med Ultrason (2001). 2012; 39:265–269.
Article13. Hung MJ, Kao YC, Chen WS, et al. Layer-specific quantification of myocardial deformation in sepsis-induced Takotsubo cardiomyopathy: Three case reports of a serial 2-dimensional speckle-tracking echocardiographic study. Medicine (Baltimore). 2016; 95:e5250.14. Madhavan M, Prasad A. Proposed Mayo Clinic criteria for the diagnosis of Tako-Tsubo cardiomyopathy and long-term prognosis. Herz. 2010; 35:240–243.
Article15. Belghitia H, Brette S, Lafitte S, et al. Automated function imaging: a new operator-independent strain method for assessing left ventricular function. Arch Cardiovasc Dis. 2008; 101:163–169.16. Yamaji H, Iwasaki K, Kusachi S, et al. Prediction of acute left main coronary artery obstruction by 12-lead electrocardiography. ST segment elevation in lead aVR with less ST segment elevation in lead V(1). J Am Coll Cardiol. 2001; 38:1348–1354.
Article17. Kurisu S, Sato H, Kawagoe T, et al. Tako-tsubo-like left ventricular dysfunction with ST-segment elevation: a novel cardiac syndrome mimicking acute myocardial infarction. Am Heart J. 2002; 143:448–455.
Article18. Neil CJ, Nguyen TH, Singh K, et al. Relation of delayed recovery of myocardial function after takotsubo cardiomyopathy to subsequent quality of life. Am J Cardiol. 2015; 115:1085–1089.
Article19. Sharkey SW, Lesser JR, Zenovich AG, et al. Acute and reversible cardiomyopathy provoked by stress in women from the United States. Circulation. 2005; 111:472–479.
Article20. Choi JO, Shin MS, Kim MJ, et al. Normal echocardiographic measurements in a Korean population study: Part I. Cardiac chamber and great artery evaluation. J Cardiovasc Ultrasound. 2015; 23:158–172.
Article21. Park JH, Lee JH, Lee SY, et al. Normal 2-dimensional strain values of the left ventricle: A substudy of the normal echocardiographic measurements in Korean population study. J Cardiovasc Ultrasound. 2016; 24:285–293.
Article22. Takigiku K, Takeuchi M, Izumi C, et al. Normal range of left ventricular 2-dimensional strain: Japanese Ultrasound Speckle Tracking of the Left Ventricle (JUSTICE) study. Circ J. 2012; 76:2623–2632.23. Kurisu S, Inoue I, Kawagoe T, et al. Time course of electrocardiographic changes in patients with tako-tsubo syndrome: comparison with acute myocardial infarction with minimal enzymatic release. Circ J. 2004; 68:77–81.24. Perazzolo Marra M, Zorzi A, Corbetti F, et al. Apicobasal gradient of left ventricular myocardial edema underlies transient T-wave inversion and QT interval prolongation (Wellens' ECG pattern) in Tako-Tsubo cardiomyopathy. Heart Rhythm. 2013; 10:70–77.
Article25. Moreira HT, Nwabuo CC, Armstrong AC, et al. Reference ranges and regional patterns of left ventricular strain and strain rate using two-dimensional speckle-tracking echocardiography in a healthy middle-aged black and white population: The CARDIA Study. J Am Soc Echocardiogr. 2017; 30:647–658.e2.
Article26. Heggemann F, Hamm K, Kaelsch T, et al. Global and regional myocardial function quantification in Takotsubo cardiomyopathy in comparison to acute anterior myocardial infarction using two-dimensional (2D) strain echocardiography. Echocardiography. 2011; 28:715–719.
Article27. Elesber AA, Prasad A, Lennon RJ, Wright RS, Lerman A, Rihal CS. Four-year recurrence rate and prognosis of the apical ballooning syndrome. J Am Coll Cardiol. 2007; 50:448–452.
Article28. Matabuena Gomez-Limon J, Isaza Arana S, Robledo-Carmona J, et al. Clinical and echocardiographic course in tako-tsubo cardiomyopathy: Long-term follow-up from a multicenter study. Int J Cardiol. 2017; 228:97–102.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Time Course of Functional Recovery and ECG Change in Takotsubo Cardiomyopathy
- Stress-Induced Cardiomyopathy: The Role of Echocardiography
- Biventricular Takotsubo Cardiomyopathy Associated with Epilepsy
- Takotsubo Cardiomyopathy Associated with Guillain-Barre Syndrome
- A case of pheochromocytoma presenting as inverted Takotsubo cardiomyopathy
