Korean J Transplant.
2019 Sep;33(3):60-64. 10.4285/jkstn.2019.33.3.60.
Kidney transplantation in human immunodeficiency virus-infected patients: a report of two cases and a review of the literatures
- Affiliations
-
- 1Department of General Surgery, Research Institute of Clinical Medicine of Chonbuk National University-Biomedical Research Institute of Chonbuk National University Hospital, Chonbuk National University Medical School, Jeonju, Korea.
- 2Department of Internal Medicine, Research Institute of Clinical Medicine of Chonbuk National University-Biomedical Research Institute of Chonbuk National University Hospital, Chonbuk National University Medical School, Jeonju, Korea. kidney@jbnu.ac.kr
- KMID: 2468181
- DOI: http://doi.org/10.4285/jkstn.2019.33.3.60
Abstract
- Human immunodeficiency virus (HIV) infection was traditionally considered an absolute contraindication for transplantation because of concerns about HIV disease progression due to immunosuppression. Since potent antiretroviral therapies (ARTs) have become widely available, the prognosis of HIV-infected kidney transplant recipients has dramatically improved. Recent results of prospective multicenter trials on kidney transplantation (KT) in HIV-positive candidates have demonstrated the success and challenges of transplantation in this population. Several studies have reported comparable patient and graft outcomes between HIV-infected and HIV-uninfected recipients after KT in the era of potent combined ARTs. We report two cases of HIV-infected patients who underwent KT at our hospital. In this paper, we present a detailed report of two cases and provide a short review of the existing literature.
MeSH Terms
Figure
-

Fig. 1 Clinical course in case 1. HAART, highly active antiretroviral therapy; Tx, therapy; MMF, mycophenolate mofetil.
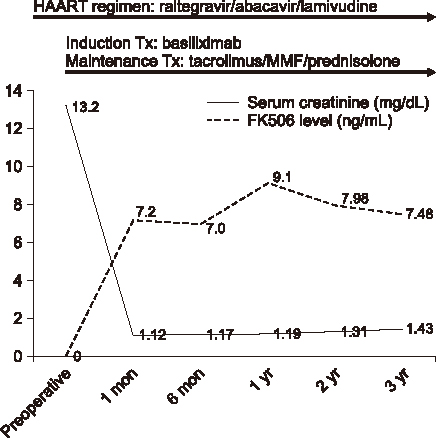
Fig. 2 Clinical course in case 2. HAART, highly active antiretroviral therapy; Tx, therapy; MMF, mycophenolate mofetil.
Reference
-
1. Choi A, Scherzer R, Bacchetti P, Tien PC, Saag MS, Gibert CL, et al. Cystatin C, albuminuria, and 5-year all-cause mortality in HIV-infected persons. Am J Kidney Dis. 2010; 56:872–882.
Article2. Günthard HF, Aberg JA, Eron JJ, Hoy JF, Telenti A, Benson CA, et al. Antiretroviral treatment of adult HIV infection: 2014 recommendations of the International Antiviral Society-USA Panel. JAMA. 2014; 312:410–425.3. Stock PG, Barin B, Murphy B, Hanto D, Diego JM, Light J, et al. Outcomes of kidney transplantation in HIV-infected recipients. N Engl J Med. 2010; 363:2004–2014.
Article4. Roland ME, Barin B, Carlson L, Frassetto LA, Terrault NA, Hirose R, et al. HIV-infected liver and kidney transplant recipients: 1- and 3-year outcomes. Am J Transplant. 2008; 8:355–365.
Article5. Mocroft A, Brettle R, Kirk O, Blaxhult A, Parkin JM, Antunes F, et al. Changes in the cause of death among HIV positive subjects across Europe: results from the EuroSIDA study. AIDS. 2002; 16:1663–1671.
Article6. Locke JE, Mehta S, Reed RD, MacLennan P, Massie A, Nellore A, et al. A national study of outcomes among HIV-infected kidney transplant recipients. J Am Soc Nephrol. 2015; 26:2222–2229.
Article7. Qiu J, Terasaki PI, Waki K, Cai J, Gjertson DW. HIV-positive renal recipients can achieve survival rates similar to those of HIV-negative patients. Transplantation. 2006; 81:1658–1661.
Article8. Roefs A, van der Ende M, IJzermans J, Weimar W, van Gelder T. Long-term survival after kidney transplantation in an HIV-positive patient. Clin Transplant. 2009; 23:278–281.
Article9. Roland ME, Barin B, Huprikar S, Murphy B, Hanto DW, Blumberg E, et al. Survival in HIV-positive transplant recipients compared with transplant candidates and with HIV-negative controls. AIDS. 2016; 30:435–444.
Article10. Solid organ transplantation in the HIV-infected patient. Am J Transplant. 2004; 4 Suppl 10:83–88.11. Miró JM, Torre-Cisnero J, Moreno A, Tuset M, Quereda C, Laguno M, et al. GESIDA/GESITRA-SEIMC, PNS and ONT consensus document on solid organ transplant (SOT) in HIV-infected patients in Spain (March, 2005). Enferm Infecc Microbiol Clin. 2005; 23:353–362.
Article12. Bhagani S, Sweny P, Brook G. British HIV Association. Guidelines for kidney transplantation in patients with HIV disease. HIV Med. 2006; 7:133–139.
Article13. Trullas JC, Cofan F, Tuset M, Ricart MJ, Brunet M, Cervera C, et al. Renal transplantation in HIV-infected patients: 2010 update. Kidney Int. 2011; 79:825–842.
Article14. Norman SP, Kommareddi M, Kaul DR. Update on kidney transplantation in HIV-infected recipients. AIDS Rev. 2012; 14:195–207.15. Panel de Expertos de Gesida. Plan Nacional sobre el Sida. AIDS Study Group/Spanish AIDS Plan consensus document on antiretroviral therapy in adults with human immunodeficiency virus infection (updated January 2010). Enferm Infecc Microbiol Clin. 2010; 28:362.e1–362.e91.16. Thompson MA, Aberg JA, Cahn P, Montaner JS, Rizzardini G, Telenti A, et al. Antiretroviral treatment of adult HIV infection: 2010 recommendations of the International AIDS Society-USA panel. JAMA. 2010; 304:321–333.17. Pulzer A, Seybold U, Schönermarck U, Stangl M, Habicht A, Bogner JR, et al. Calcineurin inhibitor dose-finding before kidney transplantation in HIV patients. Transpl Int. 2013; 26:254–258.
Article18. Karpas A, Lowdell M, Jacobson SK, Hill F. Inhibition of human immunodeficiency virus and growth of infected T cells by the immunosuppressive drugs cyclosporin A and FK 506. Proc Natl Acad Sci U S A. 1992; 89:8351–8355.
Article19. Franke EK, Luban J. Inhibition of HIV-1 replication by cyclosporine A or related compounds correlates with the ability to disrupt the Gag-cyclophilin A interaction. Virology. 1996; 222:279–282.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Ankylosing Spondylitis in a Patient with Human Immunodeficiency Virus
- Esophago-Pleural Fistula with Multiple Esophageal Ulcers in Human Immunodeficiency Virus Infected Patient: A Case Report
- A Case of Acute Erythroleukemia in a Human Immunodeficiency Virus-Infected Patient
- Malignancies in HIV-infected patients
- HIV-Infected Patients with Osteoporotic Fractures: A Case Report and Review of the Literature
