Standardization of measurement of cervical elastography, its reproducibility, and analysis of baseline clinical factors affecting elastographic parameters
- Affiliations
-
- 1Department of Obstetrics and Gynecology, Kyung Hee University School of Medicine, Seoul, Korea.
- 2Department of Obstetrics and Gynecology, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 3Department of Obstetrics and Gynecology, Kyungpook National University Hospital, Daegu, Korea.
- 4Department of Obstetrics and Gynecology, Graduate School of Medicine, Dongguk University, Seoul, Korea.
- 5Department of Obstetrics and Gynecology, Konkuk University Medical Center, Konkuk University School of Medicine, Seoul, Korea.
- 6Department of Obstetrics and Gynecology, Institute of Women's Life Medical Science, Yonsei University College of Medicine, Seoul, Korea.
- 7Department of Obstetrics and Gynecology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. ohsymd@skku.edu
- KMID: 2467931
- DOI: http://doi.org/10.5468/ogs.2020.63.1.42
Abstract
OBJECTIVE
To provide a standardized protocol for the measurement of cervical strain elastography, present its reproducibility, and analyze baseline clinical factors affecting the measurement of elastographic parameters.
METHODS
This study was performed by the Korean Research Group of Cervical Elastography. We enrolled pregnant women according to our study protocol. After measuring the cervical length, elastography was performed using the E-Cervixâ„¢ quantification tool to measure the strain of the cervix using intrinsic compression. We evaluated 5 elastographic parameters, namely, the strain of the internal os of the cervix (IOS), strain of the external os of the cervix (EOS), ratio of the strain of IOS and EOS, elasticity contrast index, and hardness ratio. For baseline clinical factors, we examined the maternal body mass index, blood pressure, heart rate, uterine artery Doppler indices, and fetal presentation.
RESULTS
We established a specific protocol for the measurement of cervical elastography using the E cervix program. For all elastographic parameters, the intra-observer intraclass correlation coefficient (ICC) ranged from 0.633 to 0.723 for single measures and from 0.838 to 0.887 for average measures, and the inter-observer ICC ranged from 0.814 to 0.977 for single measures and from 0.901 to 0.988 for average measures. Regression analysis showed that the measurement of the elastographic parameter was not affected by baseline clinical factors.
CONCLUSION
We present a standardized protocol for the measurement of cervical elastography using intrinsic compression. According to this protocol, reproducibility was acceptable and the measurement of elastographic parameters was not affected by the baseline clinical factors studied.
MeSH Terms
Figure
-
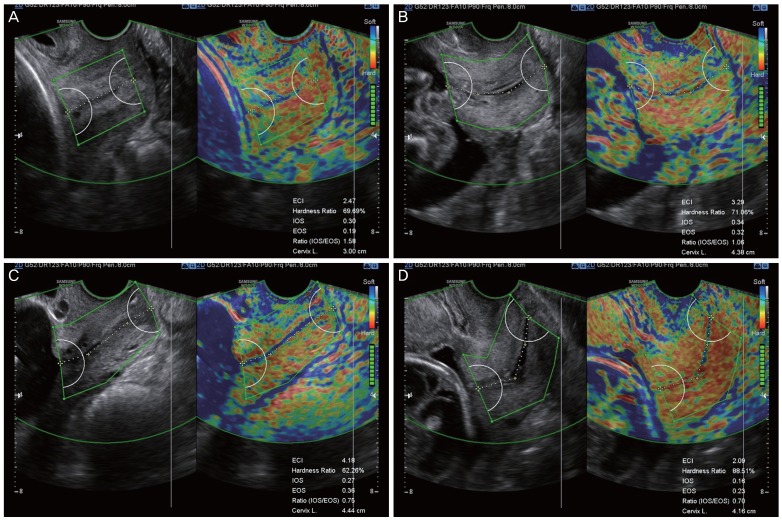
Fig. 1 Standard plane for cervical elastography using the E cervix™. During cervical length measurement, the midline sagittal plane, in which the endocervical canal is clearly visible and the anterior width of the cervix is equal to the posterior width, is obtained. Care must be taken not to apply unnecessary pressure to the anterior cervix and to keep the vaginal probe still during data acquisition. After all motion bars turn green, the screen will freeze automatically. Define the cervix area using either 2-point ROI or 4-point ROI tools. Aim to cover the entire cervix without including other organs, such as the bladder or vaginal wall. (A) Cervical elastogram using 2-point ROI when the endocervical line is straight. (B-D) Cervical elastogram using 4-point ROI when the endocervical line is curved. IOS, strain of internal os of the cervix; EOS, strain of external os of the cervix; Ratio (IOS/EOS), ratio of the strain of the internal and external os; ECI, elasticity contrast index; ROI, region of interest.
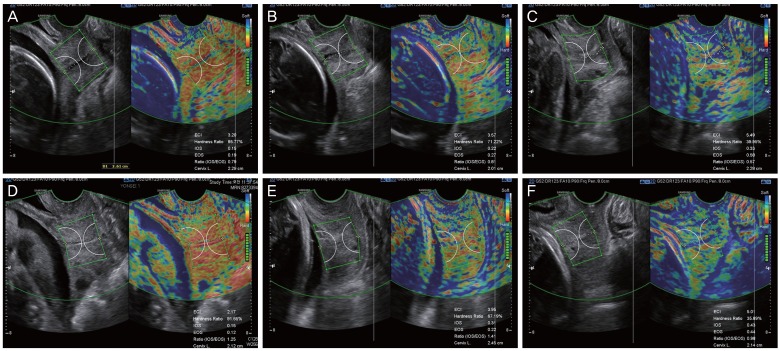
Fig. 2 Cases of cervical elastography performed in short cervix using E cervix™. (A, D) Short cervix showing relatively low strain values, reflecting a hard cervix. In (A), the values of cervical length (CL), elasticity contrast index (ECI), hardness ratio, strain of internal os of cervix (IOS), and strain of external os of cervix (EOS) were 2.29 cm, 3.20, 85.77%, 0.15, and 0.19, respectively, and in (D), these were 2.12 cm, 2.17, 91.65%, 0.15, and 0.12, respectively. (B, E) Short cervix showing relatively intermediate strain values. In (B), the values of CL, ECI, hardness ratio, IOS, and EOS were 2.01 cm, 3.57, 71.22%, 0.22, and 0.27, respectively, and in (E), these were 2.45 cm, 3.95, 67.19%, 0.31, and 0.22, respectively. (C, F) Short cervix showing relatively high strain values, reflecting a soft cervix. In (C), the values of CL, ECI, hardness ratio, IOS, and EOS were 2.28 cm, 5.49, 39.95%, 0.33, and 0.58, respectively, and in (F), these were 2.14 cm, 5.01, 35.89%, 0.43, and 0.44, respectively. Ratio (IOS/EOS), ratio of the strain of the internal and external os.
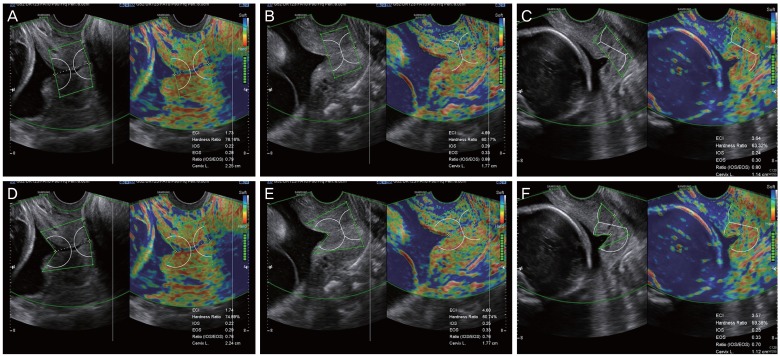
Fig. 3 Performing cervical elastography using the E cervix™ in a short cervix with funneling: 2 methods. Cervical elastography measurements were performed using 2 different methods in the same patients (A vs. D, B vs. E, C vs. F). In the upper panel, measurement of cervical elastography was performed in a way that it only encompassed the functional cervix (A-C). With this method, the lateral margin of the internal os is perpendicular to the endocervical canal, excluding funneling area. In the lower panel, cervical elastography measurements were performed in a way that it encompassed the whole cervix, including the region of funneling by maximal extension of the lateral margin of the internal os (D-F). IOS, strain of internal os of the cervix; EOS, strain of external os of the cervix; Ratio (IOS/EOS), ratio of the strain of the internal and external os; ECI, elasticity contrast index.
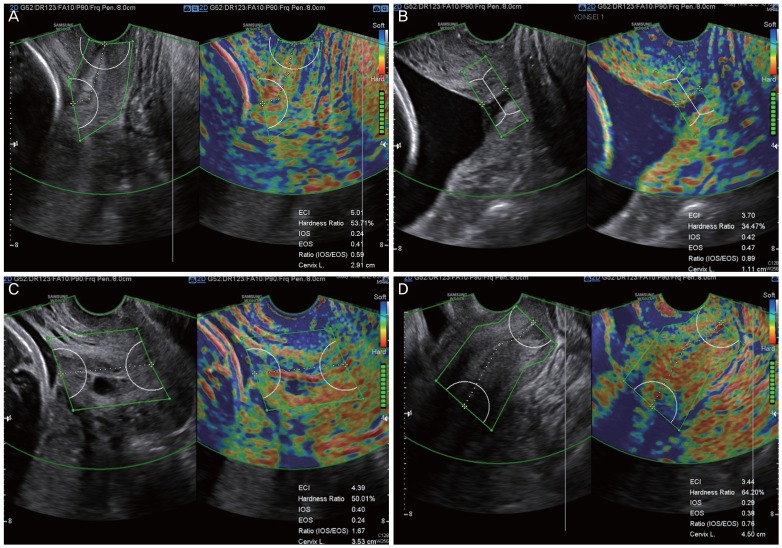
Fig. 4 Inadequate images for cervical elastography. (A) Asymmetric cervix defined as the width of anterior cervix less than half of the posterior cervix. (B) Dilated cervix. Note that the dilated endocervical canal is depicted in blue. (C) Cervix with Nabothian cyst. The Nabothian cyst, depicted in blue due to fluid collection, may increase the ECI. (D) Case in which the internal os of the cervix cannot be clearly visualized, hindering reliable measurement of cervical elastography and cervical length as well. ECI, elasticity contrast index; IOS, strain of internal os of the cervix; EOS, strain of external os of the cervix; Ratio (IOS/EOS), ratio of the strain of the internal and external os.
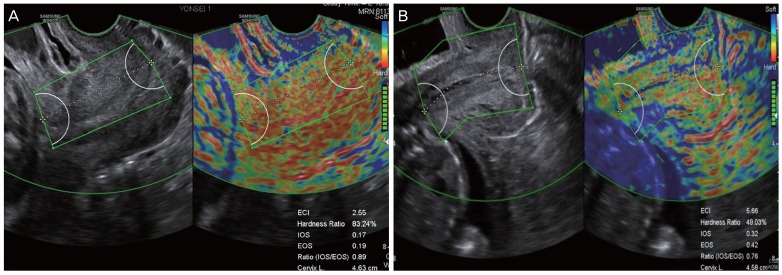
Fig. 5 The common representative images requiring re-measurement. (A) In a curved cervix, a straight line without measuring along the cervical canal would not reflect a correct cervical canal. (B) Measurements that inadvertently contain the bladder or amniotic fluid in the ROI box. This image did not follow the standardized protocol because the bladder was not empty. Ratio (IOS/EOS), ratio of the strain of the internal and external os; ECI, elasticity contrast index; ROI, region of interest.
Reference
-
1. Iams JD, Goldenberg RL, Meis PJ, Mercer BM, Moawad A, Das A, et al. The length of the cervix and the risk of spontaneous premature delivery. National Institute of Child Health and Human Development Maternal Fetal Medicine Unit Network. N Engl J Med. 1996; 334:567–572. PMID: 8569824.2. Taipale P, Hiilesmaa V. Sonographic measurement of uterine cervix at 18–22 weeks' gestation and the risk of preterm delivery. Obstet Gynecol. 1998; 92:902–907. PMID: 9840546.
Article3. Committee on Practice Bulletins—Obstetrics, The American College of Obstetricians and Gynecologists. Practice bulletin no. 130: prediction and prevention of preterm birth. Obstet Gynecol. 2012; 120:964–973. PMID: 22996126.4. Barr RG, Nakashima K, Amy D, Cosgrove D, Farrokh A, Schafer F, et al. WFUMB guidelines and recommendations for clinical use of ultrasound elastography: part 2: breast. Ultrasound Med Biol. 2015; 41:1148–1160. PMID: 25795620.
Article5. Cosgrove D, Barr R, Bojunga J, Cantisani V, Chammas MC, Dighe M, et al. WFUMB guidelines and recommendations on the clinical use of ultrasound elastography: part 4. Thyroid. Ultrasound Med Biol. 2017; 43:4–26. PMID: 27570210.
Article6. Ferraioli G, Filice C, Castera L, Choi BI, Sporea I, Wilson SR, et al. WFUMB guidelines and recommendations for clinical use of ultrasound elastography: part 3: liver. Ultrasound Med Biol. 2015; 41:1161–1179. PMID: 25800942.
Article7. Park HS, Kwon H, Kwak DW, Kim MY, Seol HJ, Hong JS, et al. Addition of cervical elastography may increase preterm delivery prediction performance in pregnant women with short cervix: a prospective study. J Korean Med Sci. 2019; 34:e68. PMID: 30863266.
Article8. Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. 2016; 15:155–163. PMID: 27330520.
Article9. Vayssière C, Morinière C, Camus E, Le Strat Y, Poty L, Fermanian J, et al. Measuring cervical length with ultrasound: evaluation of the procedures and duration of a learning method. Ultrasound Obstet Gynecol. 2002; 20:575–579. PMID: 12493046.
Article10. Iams JD, Grobman WA, Lozitska A, Spong CY, Saade G, Mercer BM, et al. Adherence to criteria for transvaginal ultrasound imaging and measurement of cervical length. Am J Obstet Gynecol. 2013; 209:365.e1–365.e5. PMID: 23958649.11. Baños N, Murillo-Bravo C, Julià C, Migliorelli F, Perez-Moreno A, Ríos J, et al. Mid-trimester sonographic cervical consistency index to predict spontaneous preterm birth in a low-risk population. Ultrasound Obstet Gynecol. 2018; 51:629–636. PMID: 28370687.
Article12. Burger M, Weber-Rössler T, Willmann M. Measurement of the pregnant cervix by transvaginal sonography: an interobserver study and new standards to improve the interobserver variability. Ultrasound Obstet Gynecol. 1997; 9:188–193. PMID: 9165682.
Article13. In : Kim M, Kwak D, Oh S, Sajin K, Yang S, Choi E, Kim M, Park J, Kim K, editors. Intra- and interobserver variance of elastographic parameters measurement of uterine cervix during pregnancy. 26th World Congress on Ultrasound in Obstetrics and Gynecology; 2016 Sep 24–28; Rome, Italy. Hoboken: Wiley;2016. 9. p. 346.14. Feltovich H, Carlson L. New techniques in evaluation of the cervix. Semin Perinatol. 2017; 41:477–484. PMID: 29191290.
Article15. Shiina T, Nightingale KR, Palmeri ML, Hall TJ, Bamber JC, Barr RG, et al. WFUMB guidelines and recommendations for clinical use of ultrasound elastography: part 1: basic principles and terminology. Ultrasound Med Biol. 2015; 41:1126–1147. PMID: 25805059.
Article16. Feltovich H, Hall TJ, Berghella V. Beyond cervical length: emerging technologies for assessing the pregnant cervix. Am J Obstet Gynecol. 2012; 207:345–354. PMID: 22717270.
Article17. Feltovich H, Hall TJ. Quantitative imaging of the cervix: setting the bar. Ultrasound Obstet Gynecol. 2013; 41:121–128. PMID: 23371343.
Article18. Issaoui M, Debost-Legrand A, Skerl K, Chauveau B, Magnin B, Delabaere A, et al. Shear wave elastography safety in fetus: a quantitative health risk assessment. Diagn Interv Imaging. 2018; 99:519–524. PMID: 29934239.
Article19. Swiatkowska-Freund M, Preis K. Elastography of the uterine cervix: implications for success of induction of labor. Ultrasound Obstet Gynecol. 2011; 38:52–56. PMID: 21484905.
Article20. Bae U, Dighe M, Dubinsky T, Minoshima S, Shamdasani V, Kim Y. Ultrasound thyroid elastography using carotid artery pulsation: preliminary study. J Ultrasound Med. 2007; 26:797–805. PMID: 17526611.21. Dighe M, Bae U, Richardson ML, Dubinsky TJ, Minoshima S, Kim Y. Differential diagnosis of thyroid nodules with US elastography using carotid artery pulsation. Radiology. 2008; 248:662–669. PMID: 18539888.
Article22. Dighe M, Kim J, Luo S, Kim Y. Utility of the ultrasound elastographic systolic thyroid stiffness index in reducing fine-needle aspirations. J Ultrasound Med. 2010; 29:565–574. PMID: 20375375.
Article23. Lim DJ, Luo S, Kim MH, Ko SH, Kim Y. Interobserver agreement and intraobserver reproducibility in thyroid ultrasound elastography. AJR Am J Roentgenol. 2012; 198:896–901. PMID: 22451558.
Article24. Dighe M, Luo S, Cuevas C, Kim Y. Efficacy of thyroid ultrasound elastography in differential diagnosis of small thyroid nodules. Eur J Radiol. 2013; 82:e274–e280. PMID: 23410906.
Article25. Hernandez-Andrade E, Garcia M, Ahn H, Korzeniewski SJ, Saker H, Yeo L, et al. Strain at the internal cervical os assessed with quasi-static elastography is associated with the risk of spontaneous preterm delivery at ≤34 weeks of gestation. J Perinat Med. 2015; 43:657–666. PMID: 25781664.
Article26. Swiatkowska-Freund M, Preis K. Cervical elastography during pregnancy: clinical perspectives. Int J Womens Health. 2017; 9:245–254. PMID: 28461768.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Elastographic measurement of the cervix during pregnancy: Current status and future challenges
- Addition of Cervical Elastography May Increase Preterm Delivery Prediction Performance in Pregnant Women with Short Cervix: a Prospective Study
- Semi-quantitative strain elastography may facilitate pre-surgical prediction of mandibular lymph nodes malignancy in dogs
- Ultrasound-based Liver Elastography: Recent Advances
- Sonographic and Strain Elastographic Findings of a Clear Cell Hidradenoma that Looked Like an Epidermoid Tumor: A Case Report
