Newly Diagnosed Klippel-Trenaunay Syndrome Presenting with Rectal Polyposis in a Male Pediatric Patient: A Case Report
- Affiliations
-
- 1Department of Pediatrics, Pusan National University Children's Hospital, Pusan National University School of Medicine, Yangsan, Korea. moonmissing@gmail.com
- KMID: 2467901
- DOI: http://doi.org/10.5223/pghn.2020.23.1.115
Abstract
- Klippel-Trenaunay syndrome (KTS) is a rare disorder characterized by a triad of abnormal bone and soft tissue growth, the presence of a port-wine stain, and venous malformations. Gastrointestinal (GI) manifestations of KTS are relatively common and generally do not cause significant problems. However, persistence can lead to chronic GI blood loss or even massive bleeding in rare cases. The majority of the severe GI manifestations associated with KTS present as vascular malformations around the GI tract and exposed vessels can lead to serious bleeding into the GI tract. Herein, we report a case of a 16-year-old boy with severe iron deficiency anemia who was previously misdiagnosed as hemorrhoid due to small amount of chronic bleeding. The actual cause of chronic GI bleeding was from an uncommon GI manifestation of KTS as rectal polyposis.
MeSH Terms
Figure
-
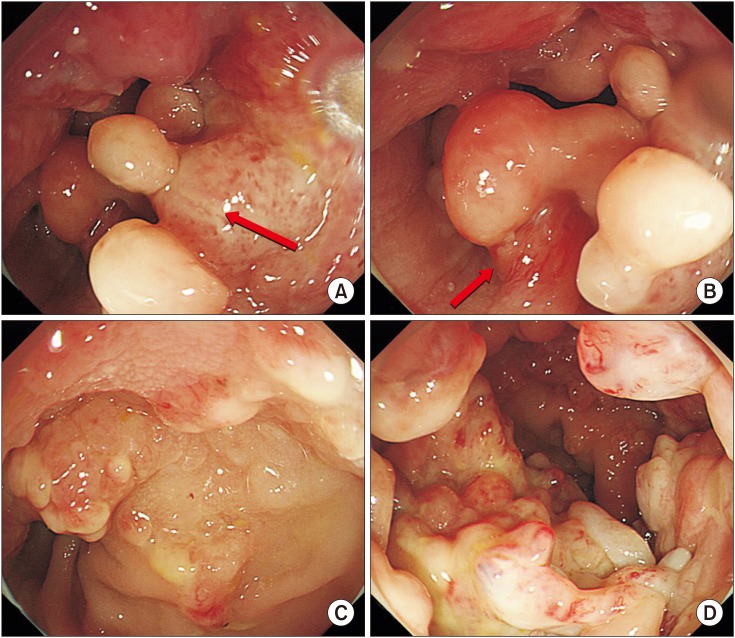
Fig. 1 Colonoscopy showing multiple numerous sessile and pedunculated (arrow) polyps (A, B) covered with diffuse fibrinous exudative materials in the rectum. Nearly the entire encircled luminal mucosa was affected. (C, D) Tortuous and dilated surface blood vessels are noted on the tip of the polyps.

Fig. 2 Diffuse, irregular, marginated, light-red capillary malformations on the trunk (A) and lateral aspect of the lower extremities (B), which are characteristic findings in Klippel-Trenaunay syndrome called port-wine stains. Hypertrophy of the right upper extremity (A) and macrodactyly of the right second toe (C) was also observed.
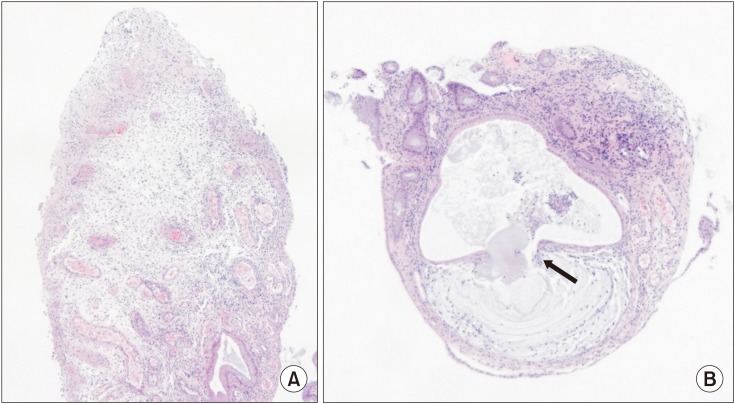
Fig. 3 (A) Histology of the rectal polyp showing diffuse lymphocytic infiltration, crypt dilatation, mucinous infiltration of the crypt, and surface ulcerations. (B) Mucus retained inside the expended crypt ruptured into the lamina propria (arrow) (H&E, ×40).
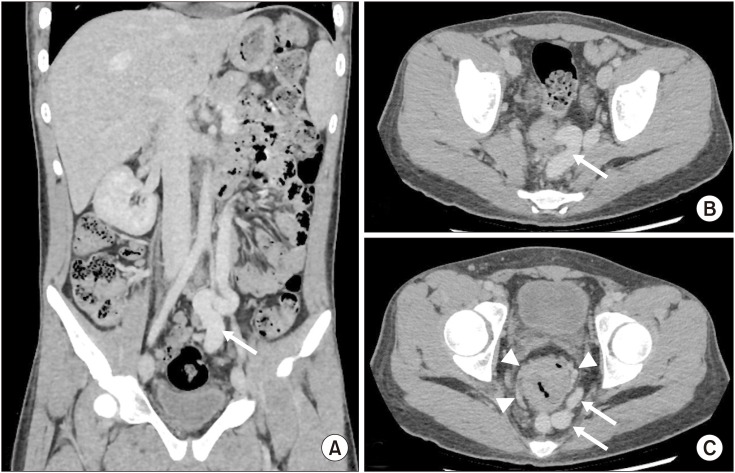
Fig. 4 (A) Coronal and (B, C) axial sections of contrast enhanced abdominal computed tomography showing a huge dilated vein (arrow), the upper portion of which drains into the splenic vein while the lower portion drains into the left internal ileac vein through the superior and middle rectal veins (A-C). (C) Congested small vessels are seen developing around the rectum (arrowhead). (B, C) Circumferential thickening of the rectum is observed along with irregularity and narrowing of the lumen.
Reference
-
1. Wilson CL, Song LM, Chua H, Ferrara M, Devine RM, Dozois RR, et al. Bleeding from cavernous angiomatosis of the rectum in Klippel-Trenaunay syndrome: report of three cases and literature review. Am J Gastroenterol. 2001; 96:2783–2788. PMID: 11569713.
Article2. Kim JH, Kim CW, Son DK, Chung BW, Yang SE, Kim JI, et al. A case of Klippel-Trenaunay-Weber syndrome presenting with esophageal and gastric varices bleeding. Korean J Gastroenterol. 2004; 43:137–141. PMID: 14978373.3. Huiras EE, Barnes CJ, Eichenfield LF, Pelech AN, Drolet BA. Pulmonary thromboembolism associated with Klippel-Trenaunay syndrome. Pediatrics. 2005; 116:e596–600. PMID: 16166386.
Article4. Gwinn JL, Lee FA. Congestive heart failure secondary to peripheral arteriovenous malformation. Klippel-Trenaunay syndrome. Am J Dis Child. 1977; 131:89–90. PMID: 189595.5. Wang ZK, Wang FY, Zhu RM, Liu J. Klippel-Trenaunay syndrome with gastrointestinal bleeding, splenic hemangiomas and left inferior vena cava. World J Gastroenterol. 2010; 16:1548–1552. PMID: 20333801.
Article6. Samo S, Sherid M, Husein H, Sulaiman S, Yungbluth M, Vainder JA. Klippel-Trenaunay syndrome causing life-threatening GI bleeding: a case report and review of the literature. Case Rep Gastrointest Med. 2013; 2013:813653. PMID: 23862081.
Article7. Choi YJ, Jee SR, Park KS, Ryu CH, Seo HR, Ha SI, et al. Involvement of splenic hemangioma and rectal varices in a patient with klippel: trenaunay syndrome. Korean J Gastroenterol. 2011; 58:157–161. PMID: 21960105.8. Brunner M, Agaimy A, Atreya R, Grützmann R, Matzel KE. Cap polyposis in children: case report and literature review. Int J Colorectal Dis. 2019; 34:363–368. PMID: 30426196.
Article
