Modified difficult index adding extremely difficult for fully impacted mandibular third molar extraction
- Affiliations
-
- 1Department of Oral and Maxillofacial Surgery, Gangnam Severance Hospital, Yonsei University College of Dentistry, Seoul, Korea. omshuh@yuhs.ac
- KMID: 2467182
- DOI: http://doi.org/10.5125/jkaoms.2019.45.6.309
Abstract
OBJECTIVES
The aim of this study was to evaluate the validity of the existing classification and difficulty index of impacted mandibular third molars in clinical situations and propose a more practical classification system.
MATERIALS AND METHODS
This study included 204 impacted mandibular third molars in 154 patients; panoramic x-ray images were obtained before tooth extraction. Factors including age, sex, and pattern of impaction were investigated. All impacted third molars were classified and scored for spatial relationship (1-5 points), depth (1-4 points), and ramus relationship (1-3 points). All variables were measured twice by the same observer at a minimum interval of one month. Finally, the difficulty index was defined based on the total points scored as slightly difficult (3-4 points), moderately difficult (5-7 points), very difficult (8-10 points), and extremely difficult (11-12 points).
RESULTS
The strength of agreement of the total points scored and difficulty index were 0.855 and 0.746, respectively. Most cases were classified as moderately difficult (73.0%). Although only 13 out of 204 cases (6.4%) were classified as extremely difficult, patients classified as extremely difficult were the oldest (P < 0.05).
CONCLUSION
For difficulty classification, the authors propose one more difficult category beyond the existing three-step difficulty index: the clinician should consider the patient's age in the difficulty index evaluation.
Keyword
Figure
-
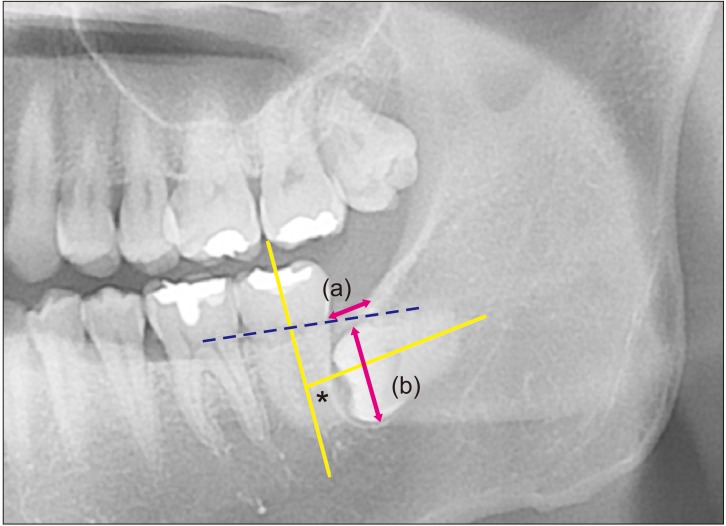
Fig. 1 Measurement and classification of the impacted third molar. Spatial relationship was classified based on the angle measured between the long axis of the impacted third molar and adjacent second molar (yellow line and an asterisk mark). Depth was classified based on the line connecting the cervico-enamel junction (CEJ) of the adjacent second molar (dotted blue line). Ramus relationship/space available was subcategorized based on the ratio between the distance from the ascending ramus to the distal of second molar (a) and the diameter of the impacted third molar (b) (pink arrows).
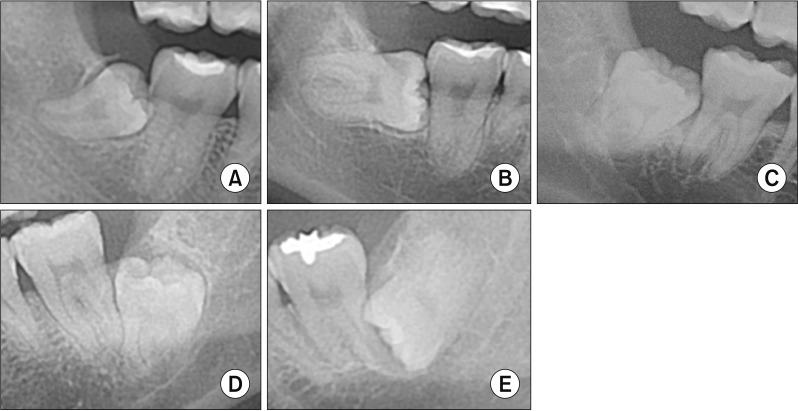
Fig. 2 Spatial relationship. Mesioangulated (A), horizontal (B), vertical (C), distoangulated (D), reverse mesioangulated (E) was defined when the long-axis of the third molar was impacted between 11° to 79°. Horizontal and vertical were defined as cases where the angle between the adjacent second molar was 80° to 100° (almost perpendicular) and −10° to 10° (almost parallel), respectively. When the long axis was −11° to −79°, it was designated distoangulated. Reverse was defined when the crown of impacted third molar was more root-oriented than horizontal.

Fig. 3 Depth. A. Level A, when more than half of the crown of impacted third molar was existing above the cervico-enamel junction (CEJ) of the adjacent second molar. B. Level B, when less than half of the presented crown was above the CEJ. Level C (C) and Level D (D), when the entire crown of the impacted third molar was located below CEJ of the adjacent second molar. Level C was defined as a condition when more than half of the impacted third molar crown was located superior to the mid-level of the adjacent second molar root. Third molar crown levels inferior to the aforementioned reference was categorized as level D.

Fig. 4 Ramus relationship/space available. A. Class I. B. Class II. C. Class III. Eruption space was calculated as the ratio of the distance between the ascending ramus to the distal of second molar (a) and diameter of the impacted third molar (b), which was illustrated in Fig. 1. When eruption space (a/b) was larger than two-thirds, it was classified as class I, between one-third and two-thirds, it was classified as class II, and when smaller than one-third, it was classified as class III.
Cited by 3 articles
-
Development and validation of a difficulty index for mandibular third molars with extraction time
Jeong-Kui Ku, Na-Hee Chang, Yeong-Kon Jeong, Sung Hyun Baik, Sun-Kyu Choi
J Korean Assoc Oral Maxillofac Surg. 2020;46(5):328-334. doi: 10.5125/jkaoms.2020.46.5.328.Third molar extraction in middle-aged and elderly patient
Jae-Young Kim
J Korean Assoc Oral Maxillofac Surg. 2021;47(5):407-408. doi: 10.5125/jkaoms.2021.47.5.407.Effect of a vertical incision on postoperative swelling after an impacted mandibular third molar extraction: two cases with split-mouth designed magnetic resonance imaging analysis
Jeong-Kui Ku, Sung Hyun Baik, Jae-Young Kim, Jong-Ki Huh
J Korean Assoc Oral Maxillofac Surg. 2023;49(2):91-95. doi: 10.5125/jkaoms.2023.49.2.91.
Reference
-
1. Eshghpour M, Nejat AH. Dry socket following surgical removal of impacted third molar in an Iranian population: incidence and risk factors. Niger J Clin Pract. 2013; 16:496–500. PMID: 23974746.
Article2. Ishii S, Abe S, Moro A, Yokomizo N, Kobayashi Y. The horizontal inclination angle is associated with the risk of inferior alveolar nerve injury during the extraction of mandibular third molars. Int J Oral Maxillofac Surg. 2017; 46:1626–1634. PMID: 28760318.
Article3. Lee YK, Park SS, Myoung H. Surgical extraction of mandibular third molar in pterygomandibular space: a case report. J Korean Assoc Oral Maxillofac Surg. 2013; 39:242–245. PMID: 24471052.
Article4. Kupferman SB, Schwartz HC. Malposed teeth in the pterygomandibular space: report of 2 cases. J Oral Maxillofac Surg. 2008; 66:167–169. PMID: 18083435.
Article5. Pell G, Gregory B. Impacted mandibular third molars: classification and modified techniques for removal. Dent Digest. 1933; 39:330–338.6. Winter GB. Principles of exodontia as applied to the impacted mandibular third molar. St. Louis: American Medical Book Company;1926.7. Pederson GW. Oral surgery. Philadelphia: WB Saunders;1988.8. Koerner KR. The removal of impacted third molars. Principles and procedures. Dent Clin North Am. 1994; 38:255–278. PMID: 8206177.9. Yuasa H, Kawai T, Sugiura M. Classification of surgical difficulty in extracting impacted third molars. Br J Oral Maxillofac Surg. 2002; 40:26–31. PMID: 11883966.
Article10. Gbotolorun OM, Arotiba GT, Ladeinde AL. Assessment of factors associated with surgical difficulty in impacted mandibular third molar extraction. J Oral Maxillofac Surg. 2007; 65:1977–1983. PMID: 17884525.
Article11. Sammartino G, Gasparro R, Marenzi G, Trosino O, Mariniello M, Riccitiello F. Extraction of mandibular third molars: proposal of a new scale of difficulty. Br J Oral Maxillofac Surg. 2017; 55:952–957. PMID: 29054564.
Article12. García AG, Sampedro FG, Rey JG, Vila PG, Martin MS. Pell-Gregory classification is unreliable as a predictor of difficulty in extracting impacted lower third molars. Br J Oral Maxillofac Surg. 2000; 38:585–587. PMID: 11092770.13. Quek SL, Tay CK, Tay KH, Toh SL, Lim KC. Pattern of third molar impaction in a Singapore Chinese population: a retrospective radiographic survey. Int J Oral Maxillofac Surg. 2003; 32:548–552. PMID: 14759117.
Article14. Abu-El Naaj I, Braun R, Leiser Y, Peled M. Surgical approach to impacted mandibular third molars--operative classification. J Oral Maxillofac Surg. 2010; 68:628–633. PMID: 20031288.15. Fielding AF, Douglass AF, Whitley RD. Reasons for early removal of impacted third molars. Clin Prev Dent. 1981; 3:19–23.16. Eshghpour M, Nezadi A, Moradi A, Shamsabadi RM, Rezaei NM, Nejat A. Pattern of mandibular third molar impaction: a cross-sectional study in northeast of Iran. Niger J Clin Pract. 2014; 17:673–677. PMID: 25385900.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Which factors are associated with difficult surgical extraction of impacted lower third molars?
- Cone beam computed tomography findings of ectopic mandibular third molar in the mandibular condyle: report of a case
- Development and validation of a difficulty index for mandibular third molars with extraction time
- Positional Relationship of the Mandibular Canal and Impacted Third Molars by Using Dental Cone Beam Computed Tomography
- The influence of mandibular third molar on mandibular angle fracture
