Scapular Dyskinesis Assessment with Low Dose Three-Dimensional Wing Computer Tomography after Anatomical Union of Clavicle Fracture
- Affiliations
-
- 1Department of Orthopedic Surgery, Inje University Seoul Paik Hospital, Seoul, Korea. jsh@paik.ac.kr
- 2Department of Orthopedic Surgery, Chuncheon Sacred Heart Hospital, Hallym University College of Medicine, Chuncheon, Korea.
- 3Department of Radiology, Inje University Sanggye Paik Hospital, Seoul, Korea.
- KMID: 2466804
- DOI: http://doi.org/10.5763/kjsm.2019.37.4.149
Abstract
- PURPOSE
Malunions after clavicle fractures are generally considered to cause scapular dyskinesis. This study aims to verify the incidence of scapular dyskinesis following anatomically reduced clavicle fracture and to verify the usefulness of low-dose three-dimensional (3D) scapular wing computed tomography (3D-scapula wing-CT) analysis.
METHODS
Twenty-four patients with mid-clavicle fracture and four patients with distal clavicle fracture were recruited. After anatomical reduction and bony union, scapular dyskinesis was assessed by history taking and physical examination by two orthopedic doctors. The mean follow-up period for the assessment was 14.3±10.1 months. Low-dose 3D-scapular wing-CT analysis in prone position was performed with calculated effective dose 2.35 mSv, which means approximately 25% dose of conventional setting. Four observers evaluated five angles (upward rotation, internal rotation, anterior tilting, superior translation, protraction) from 3D-reconstructed images on both shoulders of a patient. Authors analyzed the results between injured to normal shoulder.
RESULTS
Scapular dyskinesis or significant shortening of injured clavicle (mean clavicle length difference, − 1.77±6.36 mm) were not observed among the included 28 subjects. The difference values of the five angles between the fractured side and normal side showed no statistical significance (upward rotation: 1.51, p=0.13; superior translation: 0.89, p=0.327; anterior tilting: 1.7, p=0.096; protraction: 0.83, p=0.374; internal rotation: 0.98, p=0.406). As the interclass correlation coefficients of four observers was 0.988 (p=0.00), images from low-dose 3D-wing-CT are clear enough to assess scapular dyskinesis (interclass correlation coefficient, 0.996; p=0.00).
CONCLUSION
It is important to make anatomical reduction and length restoration of clavicle fracture for preventing scapular dyskinesis. Low-dose 3D-scapular wing-CT is an effective tool for assessing scapular dyskinesis, which provides images of sufficient quality with little increase in morbidity from radiation hazard.
Keyword
MeSH Terms
Figure
-
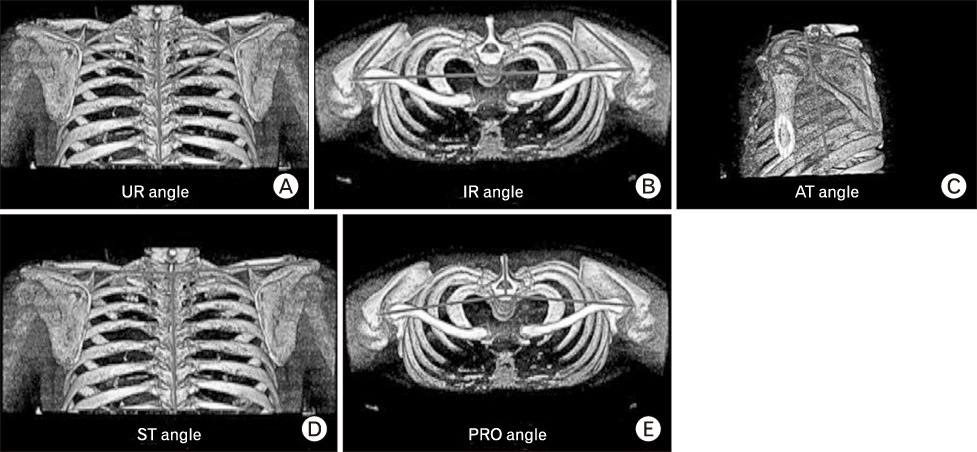
Fig. 1 Low dose three-dimensional wing computed tomography images in prone position. (A) Upward rotation (UR) angle: the angle between the extension of the line from the acromioclavicular (AC) joint to root of scapular spine (RSS) and the vertebral axis (C7–T7) on a posterior-coronal view. (B) Internal rotation (IR) angle: the angle between the line joining the 2 AC joints and the line from the corresponding AC joint to RSS on a superior-axial view. (C) Anterior tilting (AT) angle: the angle between the line from the inferomedial angle of scapula parallel to the medial border of scapula and the line joining the anterior tips of C7 and T7 vertebrae on a lateral-sagittal view. (D) Superior translation (ST) angle: the angle between the line from the AC joint to midpoint of the spinous process of the C7 vertebra and the vertebral axis (C7–T7) on a posterior-coronal view. (E) Protraction (PRO) angle: the angle between the line parallel to the vertebral axis (C7–T7) and the line from the corresponding AC joint to the center of the C7 vertebral body on a superior-axial view.
Reference
-
1. Donnelly TD, Macfarlane RJ, Nagy MT, Ralte P, Waseem M. Fractures of the clavicle: an overview. Open Orthop J. 2013; 7:329–333.2. Huttunen TT, Launonen AP, Berg HE, Lepola V, Fellander-Tsai L, Mattila VM. Trends in the incidence of clavicle fractures and surgical repair in Sweden: 2001–2012. J Bone Joint Surg Am. 2016; 98:1837–1842.3. Nordqvist A, Petersson C. The incidence of fractures of the clavicle. Clin Orthop Relat Res. 1994; (300):127–132.4. Van Tassel D, Owens BD, Pointer L, Moriatis Wolf J. Incidence of clavicle fractures in sports: analysis of the NEISS Database. Int J Sports Med. 2014; 35:83–86.5. McKee MD, Wild LM, Schemitsch EH. Midshaft malunions of the clavicle. J Bone Joint Surg Am. 2003; 85:790–797.6. Nordqvist A, Petersson CJ, Redlund-Johnell I. Mid-clavicle fractures in adults: end result study after conservative treatment. J Orthop Trauma. 1998; 12:572–576.7. Zlowodzki M, Zelle BA, Cole PA, Jeray K, McKee MD. Evidence-Based Orthopaedic Trauma Working Group. Treatment of acute midshaft clavicle fractures: systematic review of 2144 fractures: on behalf of the Evidence-Based Orthopaedic Trauma Working Group. J Orthop Trauma. 2005; 19:504–507.8. Kibler WB, Sciascia A. Current concepts: scapular dyskinesis. Br J Sports Med. 2010; 44:300–305.9. Kibler WB, Sciascia A, Wilkes T. Scapular dyskinesis and its relation to shoulder injury. J Am Acad Orthop Surg. 2012; 20:364–372.10. Keenan KE, Skedros JG. A patient with clavicle fracture and recurrent scapular winging with spontaneous resolutions. Case Rep Orthop. 2012; 2012:603726.11. Rasyid HN, Nakajima T, Hamada K, Fukuda H. Winging of the scapula caused by disruption of “sternoclaviculoscapular linkage”: report of 2 cases. J Shoulder Elbow Surg. 2000; 9:144–147.12. Shields E, Behrend C, Beiswenger T, et al. Scapular dyskinesis following displaced fractures of the middle clavicle. J Shoulder Elbow Surg. 2015; 24:e331–e336.13. Park JY, Hwang JT, Oh KS, Kim SJ, Kim NR, Cha MJ. Revisit to scapular dyskinesis: three-dimensional wing computed tomography in prone position. J Shoulder Elbow Surg. 2014; 23:821–828.14. Smekal V, Deml C, Irenberger A, et al. Length determination in midshaft clavicle fractures: validation of measurement. J Orthop Trauma. 2008; 22:458–462.15. Park JY, Hwang JT, Kim KM, Makkar D, Moon SG, Han KJ. How to assess scapular dyskinesis precisely: 3-dimensional wing computer tomography. A new diagnostic modality. J Shoulder Elbow Surg. 2013; 22:1084–1091.16. Karduna AR, McClure PW, Michener LA. Scapular kinematics: effects of altering the Euler angle sequence of rotations. J Biomech. 2000; 33:1063–1068.17. Lenza M, Buchbinder R, Johnston RV, Ferrari BA, Faloppa F. Surgical versus conservative interventions for treating fractures of the middle third of the clavicle. Cochrane Database Syst Rev. 2019; 1:CD009363.18. Ristevski B, Hall JA, Pearce D, Potter J, Farrugia M, McKee MD. The radiographic quantification of scapular malalignment after malunion of displaced clavicular shaft fractures. J Shoulder Elbow Surg. 2013; 22:240–246.19. The 2007 Recommendations of the International Commission on Radiological Protection. ICRP publication 103. Ann ICRP. 2007; 37:1–332.20. American Association of Physicists in Medicine. Policies & procedures: AAPM position statement on radiation risks from medical imaging procedures [Internet]. Alexandria (VA): American Association of Physicists in Medicine;c2018. cited 2018 Oct 4. Available from: https://www.aapm.org/org/policies/details.asp?type=PP&id=439.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Scapular Dyskinesis
- Reliability of the scapular dyskinesis test yes-no classification in asymptomatic individuals between students and expert physical therapists
- Mini-open Treatment Using Plate of Clavicle Mid-shaft Fractures
- Treatment of the Ipsilateral Fractures of the Scapular Neck and Clavicle
- Intramedullary Fixation in the Fracture of the Shaft of the Clavicle by Threaded Kirschner Wire
