Topographical anatomy of the greater omentum and transverse mesocolon: a study using human fetuses
- Affiliations
-
- 1Division of Common Curriculum, Hokkaido Chitose College of Rehabilitation, Chitose, Japan.
- 2Department of Anatomy, Jeonbuk National University Medical School, Jeonju, Korea. 407kk@hanmail.net
- 3Department of Maxillofacial Anatomy, Graduate School of Tokyo Medical and Dental University, Tokyo, Japan.
- 4Division of Internal Medicine, Jikou-kai Clinic of Home Visits, Sapporo, Japan.
- 5Department of Anatomy and Embryology, Faculty of Medicine, Complutense University, Madrid, Spain.
- KMID: 2466698
- DOI: http://doi.org/10.5115/acb.19.112
Abstract
- The greater omentum covers the transverse colon from the anterior side in adults, but people might believe the morphology stable once established during fetal life. Sections from 49 midterm and 17 late-stage human fetuses, of gestational ages (GA) 8-15 and 30-38 weeks, respectively, showed complete fusion between the greater omentum and transverse mesocolon after physiological herniation at GA 8-9 weeks; the transverse colon attaching to the anterior aspect of the gastric antrum and pylorus at GA 10-15 weeks; the colon pushing the pylorus or superior portion of the duodenum upward (at GA 10-15 weeks and 30-38 weeks); and the greater omentum without covering the greater portion of the jejunum and ileum but shifted leftward (at GA 30-38 weeks). These subsequent topographical variations of the transverse colon with the stomach and duodenum included the colon tightly fusing with the stomach by a fibrous tissue and; the greater omentum and/or the mesocolon wedged between the stomach and transverse colon. Therefore, in combination, the colon was partly separated from the greater omentum. Moreover, at GA 30-38 weeks, the duodenum consistently showed a horizontal loop in contrast to the usual C-loop in the frontal plane. Consequently, after a complete fusion occurred once between the greater omentum and transverse mesocolon, the topographical change of the upper abdominal viscera seemed to modify, change or even break the initial fusion of the peritoneum. A logical lamination of the peritoneum seemed not to simply connect with the surgical application.
Keyword
MeSH Terms
Figure
-

Fig. 1 Schematic representation of the greater omentum, duodenum and transverse colon in adults. Panel A is an anterior view showing an apron-like extension of the greater omentum. The transverse colon appears as a transparent image under the omentum. Panel B displays topographical anatomy after removal of the liver, stomach, jejunum and ileum, as well as entire parts of the colon. An attachment of the transverse mesocolon (red color) crosses the pancreas (P) longitudinally. The left and right kidneys (LK, RK) are located behind the transparent peritoneum. An insert on the left-hand side shows a logical lamination of the peritoneum. Specifically, the greater omentum, consisting of four layers, is attached to two layers of the transverse mesocolon. D3, horizontal or third portion of the duodenum; D4, ascending or fourth portion of the duodenum; SMA, superior mesentery artery.

Fig. 2 Sagittal sections of midterm fetuses. Panel A shows a specimen of crown-rump length (CRL) 32 mm (gestational age [GA] 8 weeks); panels B and D show a specimen of CRL 36 mm (GA 9 weeks); and panels C and E show a specimen of CRL 61 mm (GA 10 weeks). Panel B and C were prepared at the same magnification, and panels D and E are higher magnification views of the squares in panels B and C, respectively. (A) The greater omentum (GO) is separated from the transverse mesocolon. (B, C) The GO extends inferiorly from the stomach and is fused to the transverse mesocolon. However, the fusion plane cannot be identified (stars in panels D and E). (B) The mesocolon (arrows) is separated from the retroperitoneal structures below the pancreas (P). Scale bars=1 mm. AD, adrenal; J, jejunum; LO, lesser omentum; LY, lymph node; P, pancreas; PC, peritoneal cavity; SMV, superior mesentery vein; ST, stomach; TC, transverse colon.

Fig. 3 Horizontal sections of a specimen of crown-rump length 48 mm. Panels A and C show the uppermost and lowermost sites in the figure, respectively. Intervals are 0.4 mm between panels A and B and 1.8 mm between panels B and C. Panels D and E are higher magnification views of squares in panel A, and panel F is a higher magnification of the square in panel C. The transverse colon (TC) is attached to the anterior surface of the pylorus as well as the superior or first portion of the duodenum (D1; A, B). The TC pushes up the greater omentum (GO; A, D), and the jejunum (J) pushes up the transverse mesocolon (A, E). The omentum is fused with the mesocolon (stars in panel E), and double laminae of the omentum extend anteriorly into the liver and enclose the umbilical vein (C, F). Panels A–C (D–E) were prepared at the same magnifications. Scale bars=1 mm. AC, ascending colon; AD, adrenal; AO, aorta; AP, appendix; CL, caudate lobe of the liver; D2, descending or second portion of the duodenum; DC, descending colon; GB, gallbladder; IVC, inferior vena cava; LK, left kidney; P, pancreas; PC, peritoneal cavity; SMA, superior mesentery artery; ST, stomach; UV, umbilical vein.

Fig. 4 Horizontal sections of a specimen of crown-rump length 90 mm. Panels A and D show the uppermost and lowermost sites in the figure, respectively. Intervals between panels A and B, B and C, and C and D are 1.3 mm, 0.7 mm and 1.0 mm, respectively. Panels E–H are higher magnification views of squares in panels A–D, respectively. The transverse colon (TC) is attached to the anterior surface of the stomach (ST) as well as the superior or first portion of the duodenum (A, E). The jejunum (J) pushes up the transverse mesocolon (A). The greater omentum (GO) extends widely along the liver (B, C). The TC is tightly attached to the pylorus, the descending portion of the duodenum (D2), the pancreas (P) and the right kidney (RK) without specific borders (triangles in panels E–H). The transverse mesocolon is indicated by arrows (A–D). The arrowheads in panels A–C indicate a hole in the mesocolon. Panels A–D (E–H) were prepared at the same magnifications. Scale bars=1 mm. AD, adrenal; AO, aorta; D1, superior or first portion of the duodenum; D4, ascending or fourth portion or the duodenum; DC, descending colon; GB, gallbladder; LK, left kidney; P, pancreas; papilla, major duodenal papilla; PC, peritoneal cavity; SMA, superior mesentery artery; TC, transverse colon.

Fig. 5 Horizontal sections of a specimen of crown-rump length 97 mm. Panels A and C show the uppermost and lowermost sites in the figure, respectively. Intervals between panels A and B and B and C are 0.8 mm and 1.6 mm, respectively. The insert between panels B and C displays a higher magnification view of the irregular square in panel B. The transverse colon (TC) is attached to the anterior surface of the stomach (ST) as well as the superior or first portion of the duodenum (D1; A, B). The jejunum (J) pushes up the transverse mesocolon (panel B and inset). The greater omentum (GO) is fused with the mesocolon (stars in the inset and panel C) and the colon is tightly attached to the stomach without any specific borders (triangles in the insert). A major part of the GO is present along the left lobe of the liver (A–C). Panels A–C were prepared at the same magnification. Scale bars=1 mm. AD, adrenal; AO, aorta; D2, descending or second portion or the duodenum; D4, ascending or fourth portion of the duodenum; DC, descending colon; GB, gallbladder; LK, left kidney; P, pancreas; papilla, major duodenal papilla; PC, peritoneal cavity; RK, right kidney; SMA, superior mesentery artery; TC, transverse colon.

Fig. 6 Inter-individual differences in the macroscopic morphologies of the greater omentum. Panels A (of a fetus of crown-rump length [CRL] 258 mm) and B (of a fetus of CRL 264 mm) display the greater omentum (GO) extending leftward and inferiorly. The morphology of the wavy jejunum and ileum was similar in these fetuses. Panel C (of a fetus of CRL 272 mm) shows rightward shifting of the omentum, with the asterisk in panel C indicating an injury during dissection. RK, right kidney; ST, stomach; TC, transverse colon; UV, umbilical vein.

Fig. 7 Macroscopic and histologic observations of a specimen of crown-rump length 274 mm. Panel A shows the greater omentum (GO) extending inferiorly from the stomach and covering almost the entire jejunum and ileum. The transverse colon (TC) is located under the transparent omentum, and the right part of the TC appears wavy (star) near the pylorus. Panel B shows the transverse mesocolon reflected upward after removal of most parts of the ileum and jejunum ( J). Panel C shows a cut line of the transverse mesocolon (arrows). The mesocolon is attached to the inferior aspect of the pylorus. Panel D shows the topographic anatomy of the upper abdomen, including the TC adjacent to the stomach (ST); this sectional plane is indicated by a blue line in panel C. Panel E shows the right anterior part of panel D, and panels F and G are higher magnification views of squares in panel E. The GO appears to cover the transverse mesocolon from the anterior side, with both separated by a narrow space (circles in panels F and G). Similarly, the mesocolon is separated from the peritoneum covering the second portion of the duodenum (D2; G). Scale bars=5 mm (D), 1 mm (E–G). AC, ascending colon; AD, adrenal; AP, appendix; DC, descending colon; LK, left kidney; P, pancreas; papilla, major duodenal papilla; RK, right kidney; SMA, superior mesentery artery; UV, umbilical vein.
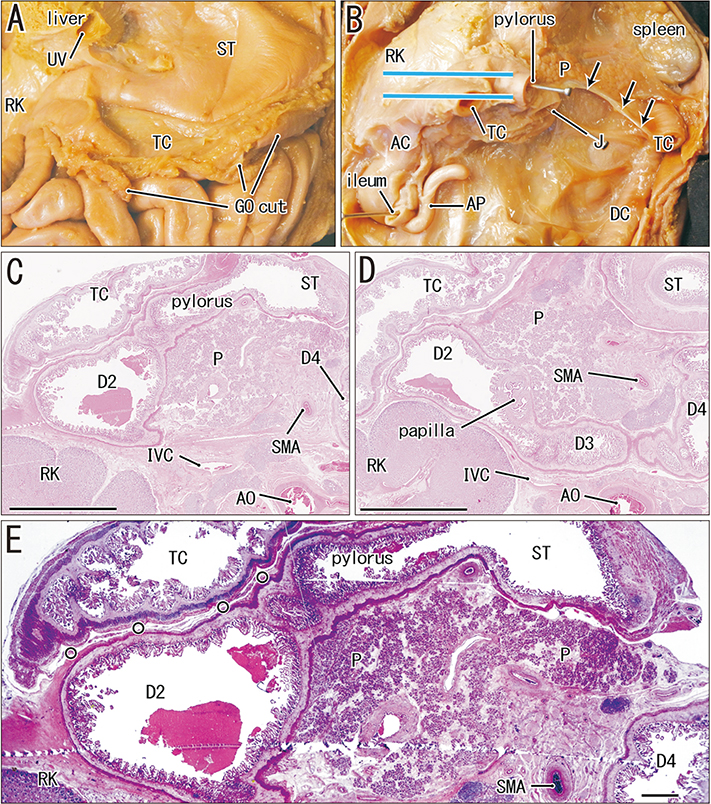
Fig. 8 Macroscopic and histologic observations of a specimen of crown-rump length 262 mm. Panel A is an anterior view after removal of major parts of the liver and greater omentum (GO), showing an attachment between the transverse colon (TC) and the stomach (ST). Panel B displays a cut surface of the transverse mesocolon (arrows) along the pancreas (P) after removal of major parts of the ST, TC, jejunum ( J) and ileum. Panels C and D are views along the horizontal planes indicated by the two blue lines in panel B. Panel C shows attachment of the TC to the anterior aspects of the pylorus and duodenum, and panel D shows attachment of the TC to the duodenum and right kidney (RK). Panel E is a higher magnification view of the central part of panel C. The TC is separated from the duodenum by a narrow peritoneal space (small circles). The duodenum, from the descending (D2) to the ascending (D4) portion, is seen in a single horizontal section (D). Scale bars=1 mm. AC, ascending colon; AO, aorta; AP, appendix; D3, horizontal or third portion of the duodenum; DC, descending colon; IVC, inferior vena cava; SMA, superior mesentery artery; UV, umbilical vein.

Fig. 9 Macroscopic and histologic observations of a specimen of crown-rump length 282 mm. Panels A displays the upper abdomen after removal of almost the entire liver and cutting of the greater omentum (GO). Panel B exhibits the transverse colon (TC) reflected upward after removal of most parts of the ileum and jejunum (J). Panel C shows partial removal of the TC. Panel D shows the topographical anatomy of the upper abdomen, including the TC, between the descending portion of the duodenum (D2) and the stomach (ST); this sectional plane is indicated by a blue line in panel C. Panel E shows the anterior part of panel E, panel F shows a higher magnification view of the square in panel E, and panel G shows a plane 1 mm above panel E. A comparison of panels E and G shows that the TC appears to push upward the superior portion of the duodenum (D1). Panel H is a higher magnification view of the square in panel G. Panels F and H both contain branches of the colic and gastric arteries (MCA, RGEA). The circles in panels F and H indicate a border between the GO and the mesocolon. The duodenum, from the descending to the ascending portion, is seen in a single horizontal section (D). Scale bars=5 mm (D), 1 mm (E–H). AC, ascending colon; AD, adrenal; AP, appendix; D3, horizontal or third portion of the duodenum; DC, descending colon; GDA, gastroduodenal artery; IVC, inferior vena cava; LK, left kidney; MCA, middle colonic artery; P, pancreas; papilla, major duodenal papilla; RGEA, right gastroepiploic artery; RK, right kidney; SMA, superior mesentery artery; UV, umbilical vein.
Reference
-
1. Carlson BM. Human embryology and developmental biology. 2nd ed. Philadelphia, PA: Mosby Elsevier;2009. p. 353–392.2. Schoenwolf GC, Bleyl SB, Brauer PR, Francis-West PH. Larsen's human embryology. 4th ed. Philadelphia, PA: Churchill Livingstone Elsevier;2009. p. 435–477.3. Sugarbaker PH. Peritonectomy procedures. Ann Surg. 1995; 221:29–42.4. Kurokawa Y, Doki Y, Mizusawa J, Terashima M, Katai H, Yoshikawa T, Kimura Y, Takiguchi S, Nishida Y, Fukushima N, Iwasaki Y, Kaji M, Hirao M, Katayama H, Sasako M. Bursectomy versus omentectomy alone for resectable gastric cancer (JCOG1001): a phase 3, open-label, randomised controlled trial. Lancet Gastroenterol Hepatol. 2018; 3:460–468.5. Cho BH, Kimura W, Song CH, Fujimiya M, Murakami G. An investigation of the embryologic development of the fascia used as the basis for pancreaticoduodenal mobilization. J Hepatobiliary Pancreat Surg. 2009; 16:824–831.6. Kim WK, Kim H, Ahn DH, Kim MH, Park HW. Timetable for intestinal rotation in staged human embryos and fetuses. Birth Defects Res A Clin Mol Teratol. 2003; 67:941–945.7. Metzger R, Metzger U, Fiegel HC, Kluth D. Embryology of the midgut. Semin Pediatr Surg. 2011; 20:145–151.8. Soffers JH, Hikspoors JP, Mekonen HK, Koehler SE, Lamers WH. The growth pattern of the human intestine and its mesentery. BMC Dev Biol. 2015; 15:31.9. Ueda Y, Yamada S, Uwabe C, Kose K, Takakuwa T. Intestinal rotation and physiological umbilical herniation during the embryonic period. Anat Rec (Hoboken). 2016; 299:197–206.10. Cho BH, Kim JH, Jin ZW, Wilting J, Rodríguez-Vázquez JF, Murakami G. Topographical anatomy of the intestines during in utero physiological herniation. Clin Anat. 2018; 31:583–592.11. Rigoard P, Haustein SV, Doucet C, Scepi M, Richer JP, Faure JP. Development of the right colon and the peritoneal surface during the human fetal period: human ontogeny of the right colon. Surg Radiol Anat. 2009; 31:585–589.12. Kim JH, Han EH, Jin ZW, Lee HK, Fujimiya M, Murakami G, Cho BH. Fetal topographical anatomy of the upper abdominal lymphatics: its specific features in comparison with other abdominopelvic regions. Anat Rec (Hoboken). 2012; 295:91–104.13. Kaigai N, Nako A, Yamada S, Uwabe C, Kose K, Takakuwa T. Morphogenesis and three-dimensional movement of the stomach during the human embryonic period. Anat Rec (Hoboken). 2014; 297:791–797.14. Jeong YJ, Cho BH, Kinugasa Y, Song CH, Hirai I, Kimura W, Fujimiya M, Murakami G. Fetal topohistology of the mesocolon transversum with special reference to fusion with other mesenteries and fasciae. Clin Anat. 2009; 22:716–729.15. Culligan K, Remzi FH, Soop M, Coffey JC. Review of nomenclature in colonic surgery: proposal of a standardised nomenclature based on mesocolic anatomy. Surgeon. 2013; 11:1–5.16. Culligan K, Walsh S, Dunne C, Walsh M, Ryan S, Quondamatteo F, Dockery P, Coffey JC. The mesocolon: a histological and electron microscopic characterization of the mesenteric attachment of the colon prior to and after surgical mobilization. Ann Surg. 2014; 260:1048–1056.17. Sato Y, Matsuki S, Yamamoto T, Goto H. Adhesion of the greater omentum seen in adult cadavers. Nihon Univ J Med. 1960; 19:3384–3391.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Pseudocyst Originated from Ectopic Pancreas of Transverse Mesocolon Associated with Colonic Duplication
- Anomalous peritoneal band connecting greater omentum to the ascending colon: a possible cause for dilation of ascending colon
- Absence of transverse colon, persistent descending mesocolon, displaced small and large bowels: a rare congenital anomaly with a high risk of volvulus formation
- Primary Multiple Mesenteric Liposarcoma of the Transverse Mesocolon
- A Case of Huge Cystic Lymphangioma of the Greater Omentum
