Geometric morphometric analysis of malocclusion on lateral cephalograms in Malaysian population
- Affiliations
-
- 1Department of Anatomy, Faculty of Medicine & Biomedical Sciences, MAHSA University, Selangor, Malaysia.
- 2Department of Basic Sciences and Oral Biology, Faculty of Dentistry, Universiti Sains Islam Malaysia, Kuala Lumpur, Malaysia. draspa76@usim.edu.my
- 3Department of Paediatric Dentistry and Orthodontics, Faculty of Dentistry, Universiti Sains Islam Malaysia, Kuala Lumpur, Malaysia.
- 4Centre of Paediatric Dentistry and Orthodontics Studies, Faculty of Dentistry, Universiti Terkonologi MARA, Shah Alam, Malaysia.
- KMID: 2466692
- DOI: http://doi.org/10.5115/acb.19.118
Abstract
- Geometric morphometrics is a new approach for shape identification in diagnosis of malocclusion. Lateral cephalogram is an X-ray that taken for diagnosing malocclusion in dental setting. The aim of this study was to determine the differences of craniofacial shape in malocclusion by application of two-dimensional geometric morphometrics and to compile the database of malocclusion in adult Malaysian population. Lateral cephalogram radiographs of 381 adults Malaysia (age 18-45) were retrieved retrospectively and assigned to three groups according to their occlusion: class I, class II, and class III. The geometric morphometric shape study incorporated nine landmarks and was analyzed in details using tpsUtil p software. Geometric morphometric analysis such was done using MorphoJ software. The results of the principal component's analysis (PCA) yielded 14 main components responsible for 100% of the variation exhibited by the malocclusion with three highly significant PCA. The highest Mahalanobis distances were exhibited by the malocclusion class II and III population. The Procrustes ANOVA showed that the shape effect was highly significant (P<0.01). The discriminant function analysis showed the high percentage of 80% discriminate among the malocclusions after cross-validation. There are significant differences for ANB angle (A point-Nasion-B point) in all malocclusion groups. Class II has the widest ANB angle while class III has the most acute ANB angle. Skeletal shape was clearly associated with dental malocclusion and showed considerable variation. Geometric morphometrics is an alternative research tool and can be used for diagnosing individual classification of malocclusion.
MeSH Terms
Figure
-
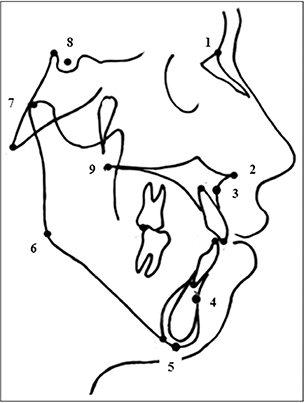
Fig. 1 Map of nine anatomical landmarks: 1, nasion (Na); 2, anterior nasal spine (ANS); 3, A-point (A); 4, B-point (B); 5, menton (Me); 6, gonion; 7, porion (Po); 8, Sella (S); 9, posterior nasal spine.
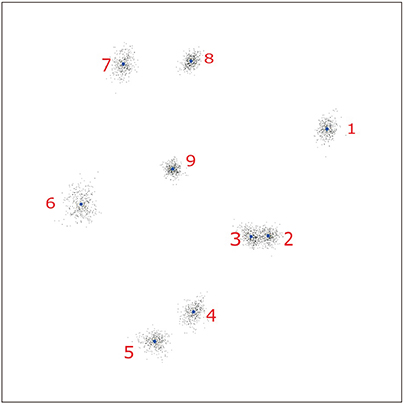
Fig. 2 Generalized procrustes analysis consisting of scatterplot of the superimposed landmark configurations.
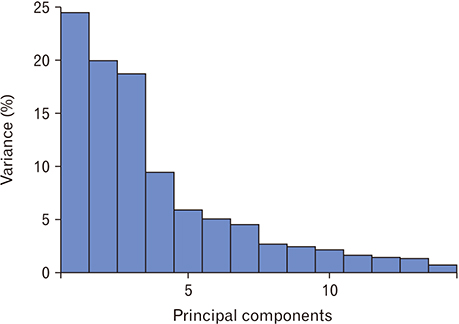
Fig. 3 Screen plot showing the amount of variance for all classes of malocclusion.
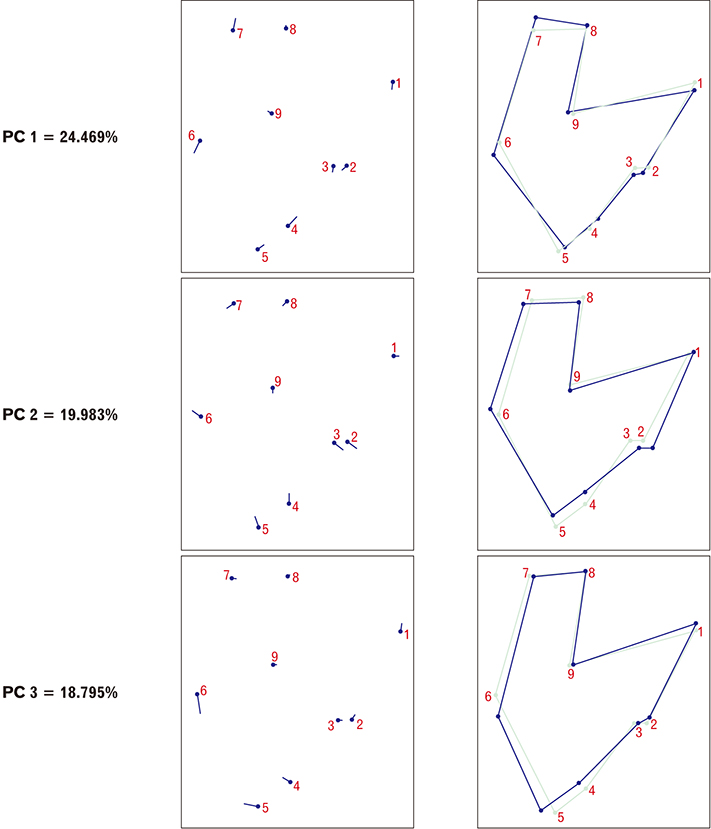
Fig. 4 Lollipop graph with shape changes of first-three principal component (PC).
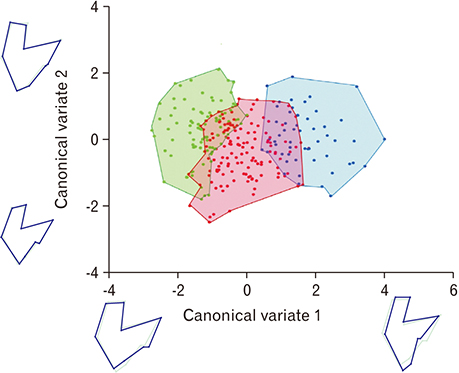
Fig. 5 Scatter plot of the first two between-group principal components of shape. Class I patients are shown by red filled region, class II patients by green filled region, class III patients by blue region. Shape differences associated with canovial variate axes are visualized by wire-frame graphs illustrating the shape changes corresponding to scores of −4 and 6 for CV1 and −4 and 6 for CV2.
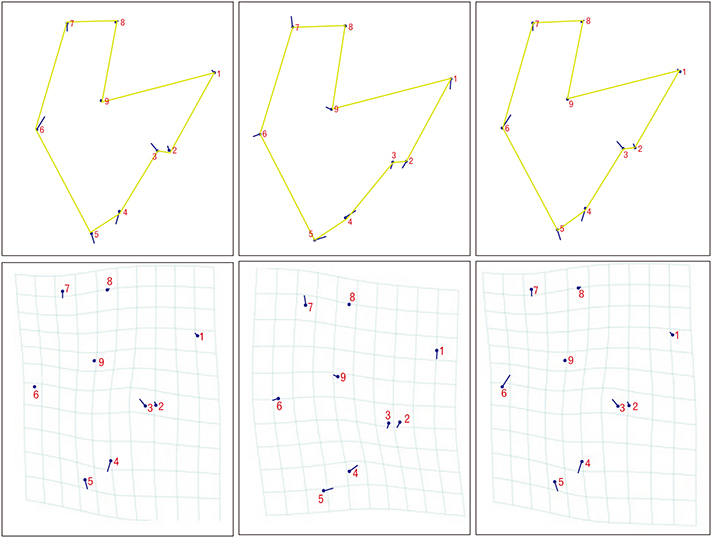
Fig. 6 Wire-frame and transformation grid graphs illustrating the mean shape of three different class of malocclusion.
Reference
-
1. Ramfjord SP, Ash MM. Occlusion. 3rd ed. Philadelphia: WB Saunders Co.;1982.2. Gruenbaum T. Famous figures in dentistry mouth. JASDA. 2010; 30:18.3. Parmesh H, Mathur VP. National Oral Health Care Program. Indian Pediatr. 2002; 39:1001–1005.4. Katz MI. Angle’s classification revisited. Am J Orthod Dentofacial Orthop. 2007; 132:716–717.5. McIntyre GT, Mossey PA. Size and shape measurement in contemporary cephalometrics. Eur J Orthod. 2003; 25:231–242.6. Moyers RE, Bookstein FL. The inappropriateness of conventional cephalometrics. Am J Orthod. 1979; 75:599–617.7. Bookstein FL. Reconsidering “The inappropriateness of conventional cephalometrics”. Am J Orthod Dentofacial Orthop. 2016; 149:784–797.8. Halazonetis DJ. Morphometrics for cephalometric diagnosis. Am J Orthod Dentofacial Orthop. 2004; 125:571–581.9. Rein TR, Harvati K. Geometric morphometrics and virtual anthropology: advances in human evolutionary studies. Anthropol Anz. 2014; 71:41–55.10. Cooke SB, Terhune CE. Form, function, and geometric morphometrics. Anat Rec (Hoboken). 2015; 298:5–28.11. Díaz Muñoz A, Soto GM. Skeletodental diagnosis using a geometric morphometric approach. Int J Odontostomat. 2014; 8:5–11.12. Freudenthaler J, Čelar A, Ritt C, Mitteröcker P. Geometric morphometrics of different malocclusions in lateral skull radiographs. J Orofac Orthop. 2017; 78:11–20.13. James Rohlf F, Marcus LF. A revolution morphometrics. Trends Ecol Evol. 1993; 8:129–132.14. Krey KF, Dannhauer KH. Morphometric analysis of facial profile in adults. J Orofac Orthop. 2008; 69:424–436.15. Mageet AO. Classification of skeletal and dental malocclusion: revisited. Stomatol Edu J. 2016; 3:38–44.16. Wellens HL, Kuijpers-Jagtman AM, Halazonetis DJ. Geometric morphometric analysis of craniofacial variation, ontogeny and modularity in a cross-sectional sample of modern humans. J Anat. 2013; 222:397–409.17. Dryden IL, Mardia KV. Statistical shape analysis. Chichester: Wiley;1998. p. 2716–2717.18. Klingenberg CP. Size, shape, and form: concepts of allometry in geometric morphometrics. Dev Genes Evol. 2016; 226:113–137.19. Enlow DH, Kuroda T, Lewis AB. The morphological and morphogenetic basis for craniofacial form and pattern. Angle Orthod. 1971; 41:161–188.20. Franchi L, Baccetti T, McNamara JA Jr. Thin-plate spline analysis of mandibular growth. Angle Orthod. 2001; 71:83–89.21. Moreno Uribe LM, Howe SC, Kummet C, Vela KC, Dawson DV, Southard TE. Phenotypic diversity in white adults with moderate to severe Class II malocclusion. Am J Orthod Dentofacial Orthop. 2014; 145:305–316.22. Moreno Uribe LM, Vela KC, Kummet C, Dawson DV, Southard TE. Phenotypic diversity in white adults with moderate to severe Class III malocclusion. Am J Orthod Dentofacial Orthop. 2013; 144:32–42.23. Proffit WR. Diagnosis and treatment planning for alveolar surgery, with special reference to soft tissue considerations. Trans Eur Orthod Soc. 1973; 604–608.24. Iwasaki H, Ishikawa H, Chowdhury L, Nakamura S, Iida J. Properties of the ANB angle and the Wits appraisal in the skeletal estimation of Angle’s Class III patients. Eur J Orthod. 2002; 24:477–483.25. Ghani S, Jabbar A. Correlation of ANB angle and wits appraisal in different malocclusion groups. J Pak Dent Assoc. 2013; 22:130–133.26. Zegan G, Dascălu C, Mavru RB, Anistoroaei D. Cephalometric features of class III malocclusion. Rev Med Chir Soc Med Nat Iasi. 2015; 119:1153–1160.27. Okşayan R, Aktan AM, Sökücü O, Haştar E, Ciftci ME. Does the panoramic radiography have the power to identify the gonial angle in orthodontics? ScientificWorldJournal. 2012; 2012:219708.28. Mitteroecker P, Gunz P. Advances in geometric morphometrics. Evol Biol. 2009; 36:235–247.29. Bookstein FL. Landmark methods for forms without landmarks: morphometrics of group differences in outline shape. Med Image Anal. 1997; 1:225–243.30. Ousley SD. Forensic classification and biodistance in the 21st century: the rise of learning machines. In : Pilloud MA, Hefner JT, editors. Biological Distance Analysis: Forensic and Bioarchaeological Perstpectives. San Diego, CA: Academic Press;2016. p. 197–212.31. Ibrahim A, Alias A, Nor FM, Swarhib M, Abu Bakar SN, Das S. Study of sexual dimorphism of Malaysian crania: an important step in identification of the skeletal remains. Anat Cell Biol. 2017; 50:86–92.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Geometric morphometric analysis of malocclusion on lateral cephalograms in Malaysian population
- Comparison of analysis of the lateral cephalogram and analysis of lateral facial photograph
- The comparative study of three-dimensional cephalograms to actual models and conventional lateral cephalograma in linear and angular measurements
- Dilemma of gonial angle measurement: Panoramic radiograph or lateral cephalogram
- Correction of positional change of frontal cephalometric landmarks caused by vertical head rotation
