Clinical Characteristics of Chronic Cough in Korea
- An TJ

- Kim JW
- Choi EY
- Jang SH
- Lee HY
- Kang HS
- Koo HK
- Lee JM
- Kim SK
- Shin JW
- Park SY
- Rhee CK
- Moon JY
- Kim YH
- Lee H
- Kim YH
- Kim JH
- Lee SH
- Kim DK
- Yoo KH
- Kim DG
- Jung KS
- Kim HJ
- Yoon HK
- on behalf of the Cough Study Group of the Korean Academy of Tuberculosis and Respiratory Diseases
- Affiliations
-
- 1Division of Pulmonary, Allergy and Critical Care Medicine, Department of Internal Medicine, Yeouido St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea. cmcyhg@gmail.com
- 2Division of Pulmonology and Critical Care Medicine, Department of Internal Medicine, Uijeongbu St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Uijeongbu, Korea.
- 3Division of Pulmonary and Allergy, Department of Internal Medicine, Regional Respiratory Center, Yeungnam University Hospital, Daegu, Korea.
- 4Division of Pulmonary, Allergy, and Critical Care Medicine, Department of Medicine, Hallym University Sacred Heart Hospital, Hallym University College of Medicine, Anyang, Korea.
- 5Division of Pulmonary, Allergy and Critical Care Medicine, Department of Internal Medicine, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea.
- 6Division of Pulmonary, Allergy and Critical Care Medicine, Department of Internal Medicine, Bucheon St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Bucheon, Korea.
- 7Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Ilsan Paik Hospital, Inje University College of Medicine, Goyang, Korea.
- 8Division of Pulmonology, Department of Internal Medicine, St. Vincent's Hospital, College of Medicine, The Catholic University of Korea, Suwon, Korea.
- 9Division of Pulmonary, Allergy, and Critical Care Medicine, Department of Internal Medicine, Chung-Ang University College of Medicine, Seoul, Korea.
- 10Division of Pulmonary and Critical Care Medicine, Chungnam University Medical Center, Daejeon, Korea.
- 11Department of Internal Medicine, Hanyang University Guri Hospital, Hanyang University College of Medicine, Guri, Korea.
- 12Department of Pulmonary and Critical Care Medicine, Kyung Hee University Hospital at Gangdong, Seoul, Korea.
- 13Department of Internal Medicine, Hanyang University College of Medicine, Seoul, Korea.
- 14Division of Pulmonary, Department of Internal Medicine, Korea University Ansan Hospital, Ansan, Korea.
- 15Division of Pulmonary, Critical Care and Sleep Medicine, Department of Internal Medicine, St. Paul's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea.
- 16Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Seoul Metropolitan Government-Seoul National University Boramae Medical Center, Seoul National University College of Medicine, Seoul, Korea.
- 17Division of Pulmonary, Allergy and Critical Care Medicine, Department of Internal Medicine, Konkuk University School of Medicine, Seoul, Korea.
- 18Division of Pulmonary, Allergy and Critical Care Medicine, Hallym University Kangnam Sacred Heart Hospital, Seoul, Korea.
- 19Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Wonkwang University Sanbon Hospital, Wonkwang University School of Medicine, Gunpo, Korea.
- KMID: 2466618
- DOI: http://doi.org/10.4046/trd.2019.0018
Abstract
- BACKGROUND
Chronic cough is defined as a cough lasting more than 8 weeks and socio-economic burden of chronic cough is enormous. The characteristics of chronic cough in Korea are not well understood. The Korean Academy of Tuberculosis and Respiratory Diseases (KATRD) published guidelines on cough management in 2014. The current study evaluated the clinical characteristics of chronic cough in Korea and the efficacy of the KATRD guidelines.
METHODS
This was a multi-center, retrospective observational study conducted in Korea. The participants were over 18 years of age. They had coughs lasting more than 8 weeks. Subjects with current pulmonary diseases, smokers, ex-smokers with more than 10 pack-years or who quit within the past 1 year, pregnant women, and users of cough-inducing medications were excluded. Evaluation and management of cough followed the KATRD cough-management guidelines.
RESULTS
Participants with chronic cough in Korea showed age in the late forties and cough duration of more than 1 year. Upper airway cough syndrome was the most common cause of cough, followed by cough-variant asthma (CVA). Gastro-esophageal reflux diseases and eosinophilic bronchitis were less frequently observed. Following the KATRD cough-management guidelines, 91.2% of the subjects improved after 4 weeks of treatment. Responders were younger, had a longer duration of cough, and an initial impression of CVA. In univariate and multivariate analyses, an initial impression of CVA was the only factor related to better treatment response.
CONCLUSION
The causes of chronic cough in Korea differed from those reported in other countries. The current Korean guidelines proved efficient for treating Korean patients with chronic cough.
Keyword
MeSH Terms
Figure
-
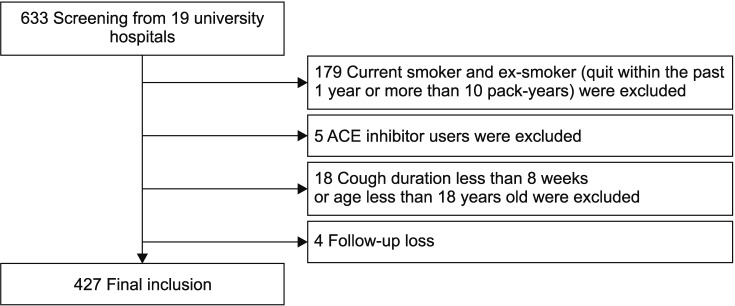
Figure 1 Flow diagram of study. Overall 633 patients were screened. Current smoker and ex-smoker (quit within the past 1 year or more than 10 pack-years) were excluded. Angiotensin-converting enzyme (ACE) inhibitor users were excluded. Participants who were not more than 8 weeks of cough or 18 years old were excluded also. Four patients were lost during follow up. Finally, 427 participants were included in this study.
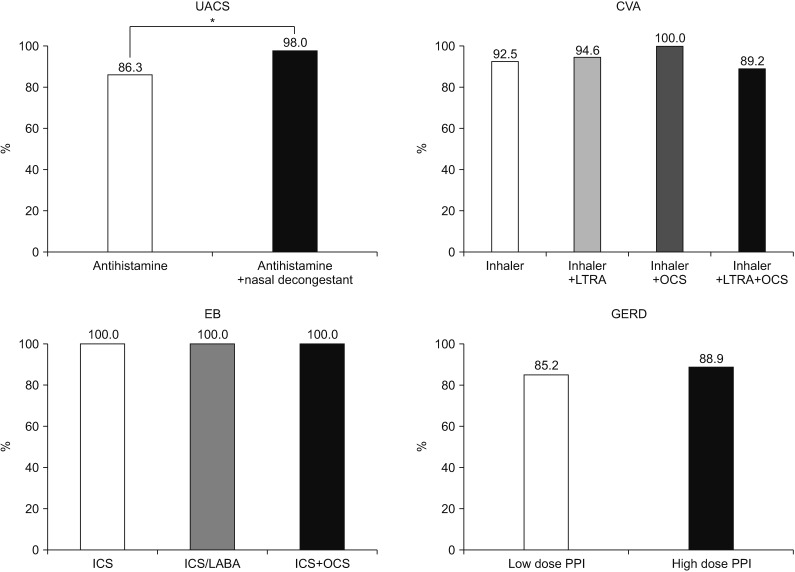
Figure 2 Treatment outcomes according to medication. For the treatment of upper airway cough syndrome (UACS), the combination of an antihistamine with a nasal decongestant had a better response than that by treatment with an antihistamine alone (p=0.03). For the treatment of cough-variant asthma (CVA), there was no significant difference in treatment outcome between an inhaler alone, such as inhaled corticosteroid (ICS) or ICS/long-acting β-agonist (LABA), and the combination of an inhaler with leukotriene receptor antagonist (LTRA) or oral corticosteroid (OCS) or LTRA plus OCS. Cough improved in the overall eosinophilic bronchitis (EB) group. There was no significant difference in gastro-esophageal reflux disease (GERD) treatment according to the proton-pump inhibitor (PPI) dose. *Antihistamine vs. antihistamine plus nasal decongestant (p<0.05).
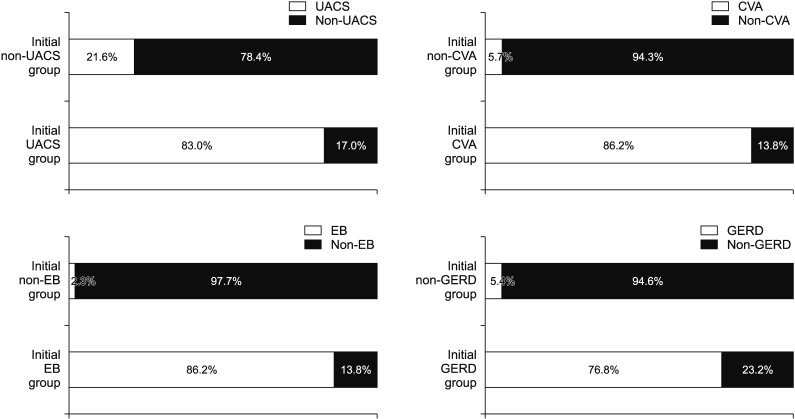
Figure 3 Consistency between the initial impression and final diagnosis of chronic cough. All etiologies showed a high consistency between the initial impression and final diagnosis of chronic cough. Of those with and those without an initial impression of upper airway cough syndrome (UACS), 83% and 21.6%, respectively, were ultimately diagnosed with UACS. The final diagnosis was the same (86.2%) between those with an initial impression of cough-variant asthma (CVA) and those with an initial impression of eosinophilic bronchitis (EB). In contrast, the final diagnosis was not gastro-esophageal reflux disease (GERD) in 23.2% of those with an initial impression of GERD.
Reference
-
1. Birring SS, Prudon B, Carr AJ, Singh SJ, Morgan MD, Pavord ID. Development of a symptom specific health status measure for patients with chronic cough: Leicester Cough Questionnaire (LCQ). Thorax. 2003; 58:339–343. PMID: 12668799.
Article2. Morice AH, McGarvey L, Pavord I. British Thoracic Society Cough Guideline Group. Recommendations for the management of cough in adults. Thorax. 2006; 61(Suppl 1):i1–i24. PMID: 16936230.
Article3. Song WJ, Chang YS, Faruqi S, Kim JY, Kang MG, Kim S, et al. The global epidemiology of chronic cough in adults: a systematic review and meta-analysis. Eur Respir J. 2015; 45:1479–1481. PMID: 25657027.
Article4. Song WJ, Morice AH, Kim MH, Lee SE, Jo EJ, Lee SM, et al. Cough in the elderly population: relationships with multiple comorbidity. PLoS One. 2013; 8:e78081. PMID: 24205100.
Article5. Chung KF, Pavord ID. Prevalence, pathogenesis, and causes of chronic cough. Lancet. 2008; 371:1364–1374. PMID: 18424325.
Article6. Rhee CK, Jung JY, Lee SW, Kim JH, Park SY, Yoo KH, et al. The Korean cough guideline: recommendation and summary statement. Tuberc Respir Dis. 2016; 79:14–21.
Article7. Faruqi S, Murdoch RD, Allum F, Morice AH. On the definition of chronic cough and current treatment pathways: an international qualitative study. Cough. 2014; 10:5. PMID: 25009577.
Article8. Escamilla R, Roche N. Cough hypersensitivity syndrome: towards a new approach to chronic cough. Eur Respir J. 2014; 44:1103–1106. PMID: 25362115.
Article9. Haque RA, Usmani OS, Barnes PJ. Chronic idiopathic cough: a discrete clinical entity? Chest. 2005; 127:1710–1713. PMID: 15888850.10. Irwin RS, Curley FJ, French CL. Chronic cough. The spectrum and frequency of causes, key components of the diagnostic evaluation, and outcome of specific therapy. Am Rev Respir Dis. 1990; 141:640–647. PMID: 2178528.
Article11. Palombini BC, Villanova CA, Araujo E, Gastal OL, Alt DC, Stolz DP, et al. A pathogenic triad in chronic cough: asthma, postnasal drip syndrome, and gastroesophageal reflux disease. Chest. 1999; 116:279–284. PMID: 10453852.12. Simpson G. Investigation and management of persistent dry cough. Thorax. 1999; 54:469–470.
Article13. Pratter MR. Chronic upper airway cough syndrome secondary to rhinosinus diseases (previously referred to as postnasal drip syndrome): ACCP evidence-based clinical practice guidelines. Chest. 2006; 129(1 Suppl):63S–71S. PMID: 16428694.14. Macedo P, Saleh H, Torrego A, Arbery J, MacKay I, Durham SR, et al. Postnasal drip and chronic cough: an open interventional study. Respir Med. 2009; 103:1700–1705. PMID: 19481918.
Article15. Dicpinigaitis PV. Cough. 4: cough in asthma and eosinophilic bronchitis. Thorax. 2004; 59:71–72. PMID: 14694253.16. Badillo R, Francis D. Diagnosis and treatment of gastroesophageal reflux disease. World J Gastrointest Pharmacol Ther. 2014; 5:105–112. PMID: 25133039.
Article17. Spinou A, Birring SS. An update on measurement and monitoring of cough: what are the important study endpoints? J Thorac Dis. 2014; 6(Suppl 7):S728–S734. PMID: 25383207.18. Kang MG, Song WJ, Kim HJ, Won HK, Sohn KH, Kang SY, et al. Point prevalence and epidemiological characteristics of chronic cough in the general adult population: The Korean National Health and Nutrition Examination Survey 2010-2012. Medicine (Baltimore). 2017; 96:e6486. PMID: 28353590.19. Koo HK, Jeong I, Lee SW, Park J, Kim JH, Park SY, et al. Prevalence of chronic cough and possible causes in the general population based on the Korean National Health and Nutrition Examination Survey. Medicine (Baltimore). 2016; 95:e4595. PMID: 27631208.
Article20. Fontana GA, Pistolesi M. Cough. 3: chronic cough and gastrooesophageal reflux. Thorax. 2003; 58:1092–1095. PMID: 14645983.21. Yamasaki A, Hanaki K, Tomita K, Watanabe M, Hasagawa Y, Okazaki R, et al. Cough and asthma diagnosis: physicians' diagnosis and treatment of patients complaining of acute, subacute and chronic cough in rural areas of Japan. Int J Gen Med. 2010; 3:101–107. PMID: 20463827.22. Matsumoto H, Niimi A, Takemura M, Ueda T, Yamaguchi M, Matsuoka H, et al. Prevalence and clinical manifestations of gastro-oesophageal reflux-associated chronic cough in the Japanese population. Cough. 2007; 3:1. PMID: 17210085.
