J Pathol Transl Med.
2019 Nov;53(6):399-402. 10.4132/jptm.2019.08.05.
Concurrent Anti-glomerular Basement Membrane Nephritis and IgA Nephropathy
- Affiliations
-
- 1Department of Pathology, Chungnam National University School of Medicine, Daejeon, Republic of Korea. mkyeo83@gmail.com
- 2Department of Nephrology, Chungnam National University School of Medicine, Daejeon, Republic of Korea.
- KMID: 2465440
- DOI: http://doi.org/10.4132/jptm.2019.08.05
Abstract
- Anti-glomerular basement membrane (GBM) nephritis is characterized by circulating anti-GBM antibodies and crescentic glomerulonephritis (GN) with deposition of IgG along the GBM. In a limited number of cases, glomerular immune complexes have been identified in anti-GBM nephritis. A 38-year-old female presented azotemia, hematuria, and proteinuria without any pulmonary symptoms. A renal biopsy showed crescentic GN with linear IgG deposition along the GBM and mesangial IgA deposition. The patient was diagnosed as concurrent anti-GBM nephritis and IgA nephropathy. Therapies with pulse methylprednisolone and cyclophosphamide administration were effective. Concurrent cases of both anti-GBM nephritis and IgA nephropathy are rare among cases of anti-GBM diseases with deposition of immune complexes. This rare case of concurrent anti-GBM nephritis and IgA nephropathy with literature review is noteworthy.
MeSH Terms
-
Adult
Anti-Glomerular Basement Membrane Disease
Antibodies
Antigen-Antibody Complex
Azotemia
Basement Membrane*
Biopsy
Cyclophosphamide
Female
Glomerulonephritis
Glomerulonephritis, IGA*
Hematuria
Humans
Immunoglobulin A*
Immunoglobulin G
Methylprednisolone
Nephritis*
Proteinuria
Antibodies
Antigen-Antibody Complex
Cyclophosphamide
Immunoglobulin A
Immunoglobulin G
Methylprednisolone
Figure
-

Fig. 1. (A) Light microscopy shows encircling cellular crescents (periodic acid–Schiff staining). Imunofluorescence shows linear deposition of IgG along the glomerular basement membrane (GBM) (B) and granular deposition of IgA in mesangial spaces (C). (D) Electron microscopy shows a diffusely wrinkled GBM and mesangial electron-dense deposition (arrow) (uranyl acetate/lead citrate staining, ×8,000).
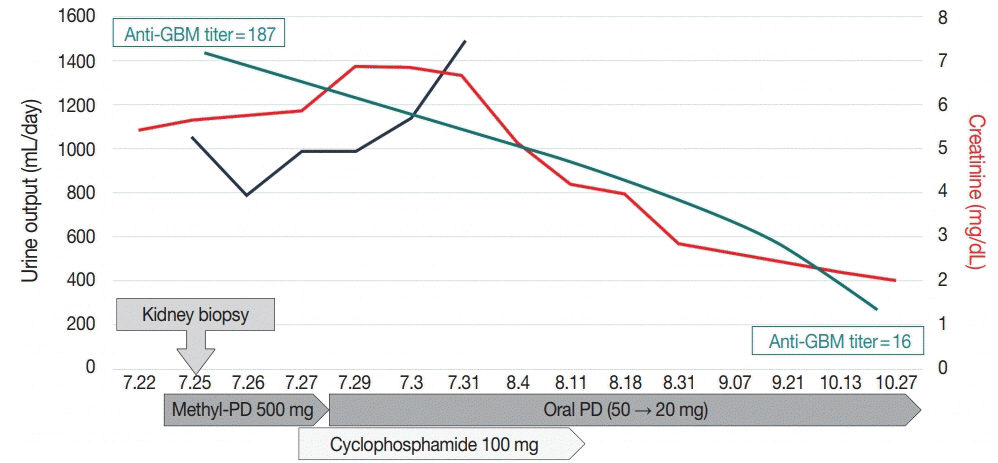
Fig. 2. Clinical course of the patient. GBM, glomerular basement membrane; PD, prednisolone.
Reference
-
1. Jennette JC, D'Agati VD, Olson JL, Silva FG. Heptinstall's pathology of the kidney. Philadelphia: Lippincott Williams & Wilkins;2014. p. 661–2.2. Cui Z, Zhao MH, Wang SX, Liu G, Zou WZ, Wang HY. Concurrent antiglomerular basement membrane disease and immune complex glomerulonephritis. Ren Fail. 2006; 28:7–14.
Article3. Rutgers A, Slot M, van Paassen P, van Breda Vriesman P, Heeringa P, Tervaert JW. Coexistence of anti-glomerular basement membrane antibodies and myeloperoxidase-ANCAs in crescentic glomerulonephritis. Am J Kidney Dis. 2005; 46:253–62.
Article4. Alchi B, Griffiths M, Sivalingam M, Jayne D, Farrington K. Predictors of renal and patient outcomes in anti-GBM disease: clinicopathologic analysis of a two-centre cohort. Nephrol Dial Transplant. 2015; 30:814–21.
Article5. Trpkov K, Abdulkareem F, Jim K, Solez K. Recurrence of anti-GBM antibody disease twelve years after transplantation associated with de novo IgA nephropathy. Clin Nephrol. 1998; 49:124–8.6. Wechsler E, Yang T, Jordan SC, Vo A, Nast CC. Anti-glomerular basement membrane disease in an HIV-infected patient. Nat Clin Pract Nephrol. 2008; 4:167–71.
Article7. Wang A, Wang Y, Wang G, Zhou Z, Xun Z, Tan X. Mesangial IgA deposits indicate pathogenesis of anti-glomerular basement membrane disease. Mol Med Rep. 2012; 5:1212–4.
Article8. Yamaguchi H, Takizawa H, Ogawa Y, Takada T, Yamaji I, Ura N. A case report of the anti-glomerular basement membrane glomerulonephritis with mesangial IgA deposition. CEN Case Rep. 2013; 2:6–10.
Article9. Gao B, Li M, Xia W, Wen Y, Qu Z. Rapidly progressive glomerulonephritis due to anti-glomerular basement membrane disease accompanied by IgA nephropathy: a case report. Clin Nephrol. 2014; 81:138–41.
Article10. Troxell ML, Houghton DC. Atypical anti-glomerular basement membrane disease. Clin Kidney J. 2016; 9:211–21.
Article11. Ge YT, Liao JL, Liang W, Xiong ZY. Anti-glomerular basement membrane disease combined with IgA nephropathy complicated with reversible posterior leukoencephalopathy syndrome: an unusual case. Am J Case Rep. 2015; 16:849–53.
Article12. Xu D, Wu J, Wu J, et al. Novel therapy for anti-glomerular basement membrane disease with IgA nephropathy: a case report. Exp Ther Med. 2016; 11:1889–92.
Article13. Emancipator SN, Lamm ME. IgA nephropathy: pathogenesis of the most common form of glomerulonephritis. In : Rubin E, Damjanov I, editors. Pathol reviews. Clifton: The Humana Press;1990. p. 113–28.14. Kamimura H, Honda K, Nitta K, et al. Glomerular expression of alpha2(IV) and alpha5(IV) chains of type IV collagen in patients with IgA nephropathy. Nephron. 2002; 91:43–50.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of IgA Nephropathy Associated with Thin Basement Membrane Disease
- IgA nephropathy combined with thin basement membrane nephropathy in children
- A Clinical and Pathological Study of Recurrent Hematuria in Childhood
- A Case of Adult Minimal Change Nephrotic Syndrome Associated with Thin Basement Membrane Nephropathy
- Changes of immune indices in children with recurrent gross hematuria (IgA nephropathy and non-IgA nephropathy) and Henoch-Schonlein purpura nephritis
