Diagnosis and non-operative treatment of shoulder pain
- Affiliations
-
- 1Department of Physical Medicine and Rehabilitation, Seoul Metropolitan Government-Seoul National University Boramae Medical Center, Seoul National University College of Medicine, Seoul, Korea. shiuk.lee@gmail.com
- KMID: 2465357
- DOI: http://doi.org/10.5124/jkma.2019.62.12.629
Abstract
- The shoulder is the third most common region in which musculoskeletal pain occurs, involving symptoms that cause a decrease in quality of life and a reduced ability to perform activities of daily life if untreated. Many lesions cause shoulder pain; therefore, we included those commonly encountered in primary care clinics. We aimed to describe the diagnosis and non-operative or conservative treatment modalities of rotator cuff tendinopathy, impingement syndrome, rotator cuff tear, adhesive capsulitis, biceps tendonitis, and acromioclavicular arthritis. Exercise has been reported to be effective for the treatment of impingement syndrome, and the effect of exercise has been shown to reduce pain. Both home-based self-exercise and exercise supervised by professionals are equally effective. Types of exercise should include stretching, active, active-assistive, and resistive exercise. Ten repetitions per set for 3 sets of each exercise should be prescribed initially post-injury. Repetition and resistance should be increased as strength grows. The use of ultrasonography for the diagnosis of shoulder pain has increased recently. Corticosteroid injection under ultrasonographic guidance is effective in reducing pain.
MeSH Terms
Figure
-
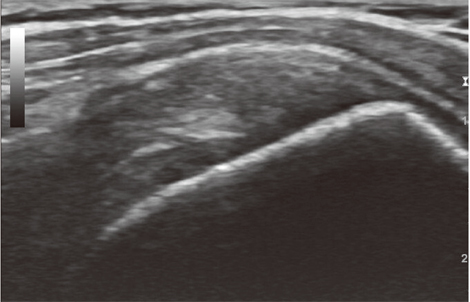
Figure 1 An ultrasonography image indicating tendinopathy of the supraspi-natus tendon.

Figure 2 Pendulum exercise for the shoulder. Informed consent was obtained from the study participant.

Figure 3 (A) Anterior shoulder stretching exercise. (B) Posterior shoulder stretching exercise. Informed consent was obtained from the subject.
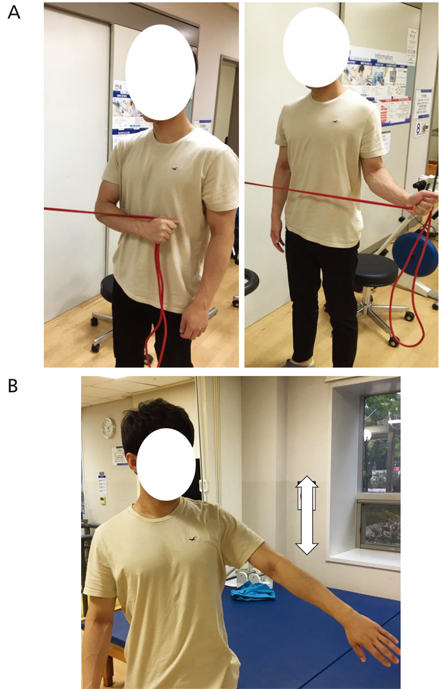
Figure 4 (A) Internal and external rotator strengthening exercise using an elastic band. (B) Scaption exercise of the shoulder. Informed consent was obtained from the participant.

Figure 5 (A) Chair press. (B) Upright rows. Informed consent was obtained from the participant.
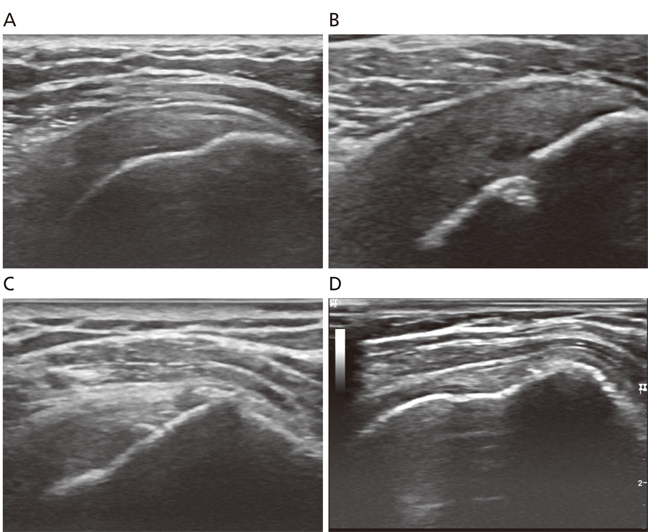
Figure 6 Ultrasonography of a supraspinatus tendon tear. (A) Normal tendon. (B) Articular side partial tear. (C) Bursal side partial tear. (D) Full thickness tear.
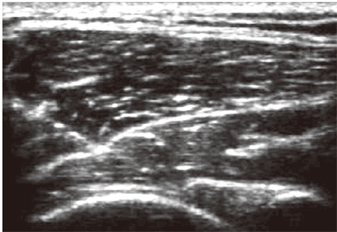
Figure 7 Intraarticular injection in the shoulder under ultrasonographic guidance.
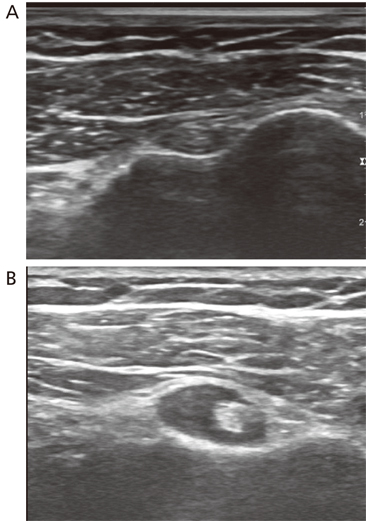
Figure 8 Ultrasonographic image of the biceps brachii tendon, transverse plane. (A) Normal. (B) Effusion.
Reference
-
1. Urwin M, Symmons D, Allison T, Brammah T, Busby H, Roxby M, Simmons A, Williams G. Estimating the burden of musculoskeletal disorders in the community: the comparative prevalence of symptoms at different anatomical sites, and the relation to social deprivation. Ann Rheum Dis. 1998; 57:649–655.
Article2. Laslett LL, Burnet SP, Jones JA, Redmond CL, McNeil JD. Musculoskeletal morbidity: the growing burden of shoulder pain and disability and poor quality of life in diabetic outpatients. Clin Exp Rheumatol. 2007; 25:422–429.3. Neer CS 2nd. Impingement lesions. Clin Orthop Relat Res. 1983; (173):70–77.
Article4. Bigliani LU, Levine WN. Subacromial impingement syndrome. J Bone Joint Surg Am. 1997; 79:1854–1868.5. Burbank KM, Stevenson JH, Czarnecki GR, Dorfman J. Chronic shoulder pain: part I. Evaluation and diagnosis. Am Fam Physician. 2008; 77:453–460.6. Naredo E, Aguado P, De Miguel E, Uson J, Mayordomo L, Gijon-Baños J, Martin-Mola E. Painful shoulder: comparison of physical examination and ultrasonographic findings. Ann Rheum Dis. 2002; 61:132–136.
Article7. Arroll B, Goodyear-Smith F. Corticosteroid injections for painful shoulder: a meta-analysis. Br J Gen Pract. 2005; 55:224–228.8. Kuhn JE. Exercise in the treatment of rotator cuff impingement: a systematic review and a synthesized evidence-based rehabilitation protocol. J Shoulder Elbow Surg. 2009; 18:138–160.
Article9. Neer CS 2nd. Anterior acromioplasty for the chronic impingement syndrome in the shoulder. 1972. J Bone Joint Surg Am. 2005; 87:1399.
Article10. Murrell GA, Walton JR. Diagnosis of rotator cuff tears. Lancet. 2001; 357:769–770.
Article11. Burk DL Jr, Karasick D, Kurtz AB, Mitchell DG, Rifkin MD, Miller CL, Levy DW, Fenlin JM, Bartolozzi AR. Rotator cuff tears: prospective comparison of MR imaging with arthrography, sonography, and surgery. AJR Am J Roentgenol. 1989; 153:87–92.
Article12. Jacobson JA. Fundamentals of musculoskeletal ultrasound. 2nd ed. Philadelphia: Elsevier/Saunders;2013.13. Redler LH, Dennis ER. Treatment of adhesive capsulitis of the shoulder. J Am Acad Orthop Surg. 2019; 27:e544–e554.
Article14. Arkkila PE, Kantola IM, Viikari JS, Rönnemaa T. Shoulder capsulitis in type I and II diabetic patients: association with diabetic complications and related diseases. Ann Rheum Dis. 1996; 55:907–914.
Article15. Lee HJ. Differential diagnosis of common shoulder pain. J Korean Med Assoc. 2014; 57:653–660.
Article16. Nam HS, Lee SU. Conservative management of shoulder pain with common causes. J Korean Med Assoc. 2014; 57:661–666.
Article17. Rizk TE, Gavant ML, Pinals RS. Treatment of adhesive capsulitis (frozen shoulder) with arthrographic capsular distension and rupture. Arch Phys Med Rehabil. 1994; 75:803–807.
Article
