Arch Hand Microsurg.
2019 Dec;24(4):388-393. 10.12790/ahm.2019.24.4.388.
Using a Pedicled Latissimus Dorsi Musculocutaneous Flap to Treat Infective Costochondritis Following Breast Reconstruction Using an Implant
- Affiliations
-
- 1Department of Plastic and Reconstructive Surgery, College of Medicine, The Catholic University of Korea, Seoul, Korea. ohdeuk1234@hanmail.net
- KMID: 2464476
- DOI: http://doi.org/10.12790/ahm.2019.24.4.388
Abstract
- Infectious costochondritis seldom occurs after breast reconstruction. The treatment requires wide debridement, appropriate wound cover, and antibiotic therapy. A 53-year-old female patient was referred due to an unhealed right breast wound. She had undergone right skin-sparing mastectomy followed by breast reconstruction with an implant. Pseudomonas aeruginosa was cultured from the wound discharge, and a computed tomography showed fluid collection underneath the pectoralis muscle with connection to the external opening as well as degenerated T4-T6 costal cartilages. Wide excision of infected tissue and costal cartilages followed by a pedicled latissimus dorsi musculocutaneous flap coverage were performed. The mastectomy wound allows a wider surgical view to prepare thoracodorsal vessels, and the harvesting the latissimus dorsi musculocutaneous flap can be more easily performed without excessive traction force or damage on pedicles. The coverage of pedicled flap was successful and the patient was injected antibiotics intravenously for 3 weeks without any postoperative complications.
MeSH Terms
Figure
-

Fig. 1 Preoperative clinical photo.
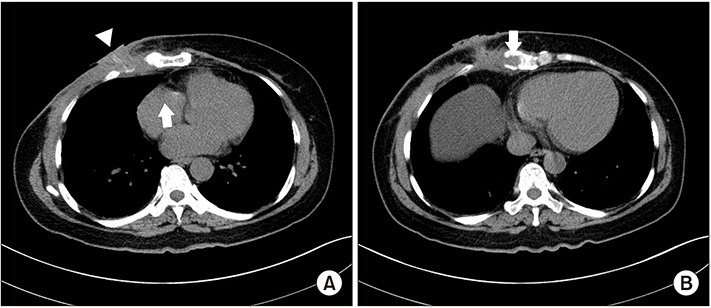
Fig. 2 Preoperative computed tomography. (A) A fluid collection underneath the pectoralis muscle (white arrow) with connecting tracts to the external opening (white arrowhead). (B) Degenerated T4–T6 costal cartilages (white arrow).

Fig. 3 Intraoperative photo: the pectoralis major muscle and 3 tracts to infected costal cartilage were resected.

Fig. 4 (A) Dissected thoracodorsal vessels. (B) The tendon inserted into the latissimus dorsi musculocutaneous was detached.

Fig. 5 Postoperative 4-month photographs without any complications.
Reference
-
1. van Schalkwyk AJ, van Wingerden JJ. A variant of Tietze's syndrome occurring after reconstructive breast surgery. Aesthetic Plast Surg. 1998; 22:430–432.
Article2. Moses MA, Banwell PE, Murphy JV, Quinlan MJ, Coleman DJ. Infective costochondritis following breast reconstruction. Plast Reconstr Surg. 2004; 114:1356–1357.
Article3. Chang DW, Youssef A, Cha S, Reece GP. Autologous breast reconstruction with the extended latissimus dorsi flap. Plast Reconstr Surg. 2002; 110:751–759. discussion 760-1.
Article4. Bakri K, Mardini S, Evans KK, Carlsen BT, Arnold PG. Workhorse flaps in chest wall reconstruction: the pectoralis major, latissimus dorsi, and rectus abdominis flaps. Semin Plast Surg. 2011; 25:43–54.
Article5. Thomas BP, Geddes CR, Tang M, Williams J, Morris SF. The vascular basis of the thoracodorsal artery perforator flap. Plast Reconstr Surg. 2005; 116:818–822.
Article6. Saint-Cyr M, Nagarkar P, Schaverien M, Dauwe P, Wong C, Rohrich RJ. The pedicled descending branch musclesparing latissimus dorsi flap for breast reconstruction. Plast Reconstr Surg. 2009; 123:13–24.
Article7. Aitken ME, Mustoe TA. Why change a good thing? Revisiting the fleur-de-lis reconstruction of the breast. Plast Reconstr Surg. 2002; 109:525–533. discussion 534-8.
Article8. Hokin JA, Silfverskiold KL. Breast reconstruction without an implant: results and complications using an extended latissimus dorsi flap. Plast Reconstr Surg. 1987; 79:58–66.9. Lee YJ, Kim HY, Han HH, et al. Comparison of dissection with harmonic scalpel and conventional bipolar electrocautery in deep inferior epigastric perforator flap surgery: A consecutive cohort study. J Plast Reconstr Aesthet Surg. 2017; 70:222–228.
Article10. Matthews B, Nalysnyk L, Estok R, et al. Ultrasonic and nonultrasonic instrumentation: a systematic review and meta-analysis. Arch Surg. 2008; 143:592–600.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Axillary Reconstruction Using a Pedicled Thoracodorsal Artery Perforator Flap Including Latissimus Dorsi Muscle Strip
- Breast Reconstruction with the Extended Latissimus Dorsi Musculocutancous Flap
- Reconstruction of an abdominal wall defect using a latissimus dorsi musculocutaneous free flap after high-intensity focused ultrasound: a case report
- Breast reconstruction using extended latissimus dorsi muscle flap
- Chest Wall and Breast Reconstruction in Poland's Syndrome
