Combination Treatment of Stereotactic Body Radiation Therapy and Immature Dendritic Cell Vaccination for Augmentation of Local and Systemic Effects
- Affiliations
-
- 1Department of Radiation Oncology, Dongnam Institute of Radiological & Medical Sciences, Busan, Korea. drasdf19@gmail.com
- 2Department of Microbiology, Dong-A University College of Medicine, Busan, Korea.
- 3Department of Research Center, Dongnam Institute of Radiological & Medical Sciences, Busan, Korea.
- KMID: 2464393
- DOI: http://doi.org/10.4143/crt.2018.186
Abstract
- PURPOSE
The purpose of this study was to investigate the efficacy of stereotactic body radiation therapy (SBRT) as a tumor-associated antigen (TAA) presentation method for dendritic cell (DC) sensitization and evaluate its effect in combination with immunotherapy using an intratumoral injection of immature DCs (iDCs).
MATERIALS AND METHODS
CT-26 colon carcinoma cell was used as a cancer cell line. Annexin V staining and phagocytosis assays were performed to determine the appropriate radiation dose and incubation time to generate TAAs. BALB/c mice were used for in vivo experiments. Cancer cells were injected into the right legs and left flanks to generate primary and metastatic tumors, respectively. The mice were subjected to radiation therapy (RT) alone, intradermal injection of electroporated DCs alone, or RT in combination with iDC intratumoral injection (RT/iDC). Tumor growth measurement and survival rate analysis were performed. Enzyme-linked immunospot and cytotoxicity assays were performed to observe the effect of different treatments on the immune system.
RESULTS
Annexin V staining and phagocytosis assays showed that 15 Gy radiation dose and 48 hours of incubation was appropriate for subsequent experiments. Maximum DC sensitization and T-cell stimulation was observed with RT as compared to other TAA preparation methods. In vivo assays revealed statistically significant delay in the growth of both primary and metastatic tumors in the RT/iDC group. The overall survival rate was the highest in the RT/iDC group.
CONCLUSION
The combination of SBRT and iDC vaccination may enhance treatment effects. Clinical trials and further studies are warranted in the future.
MeSH Terms
Figure
-
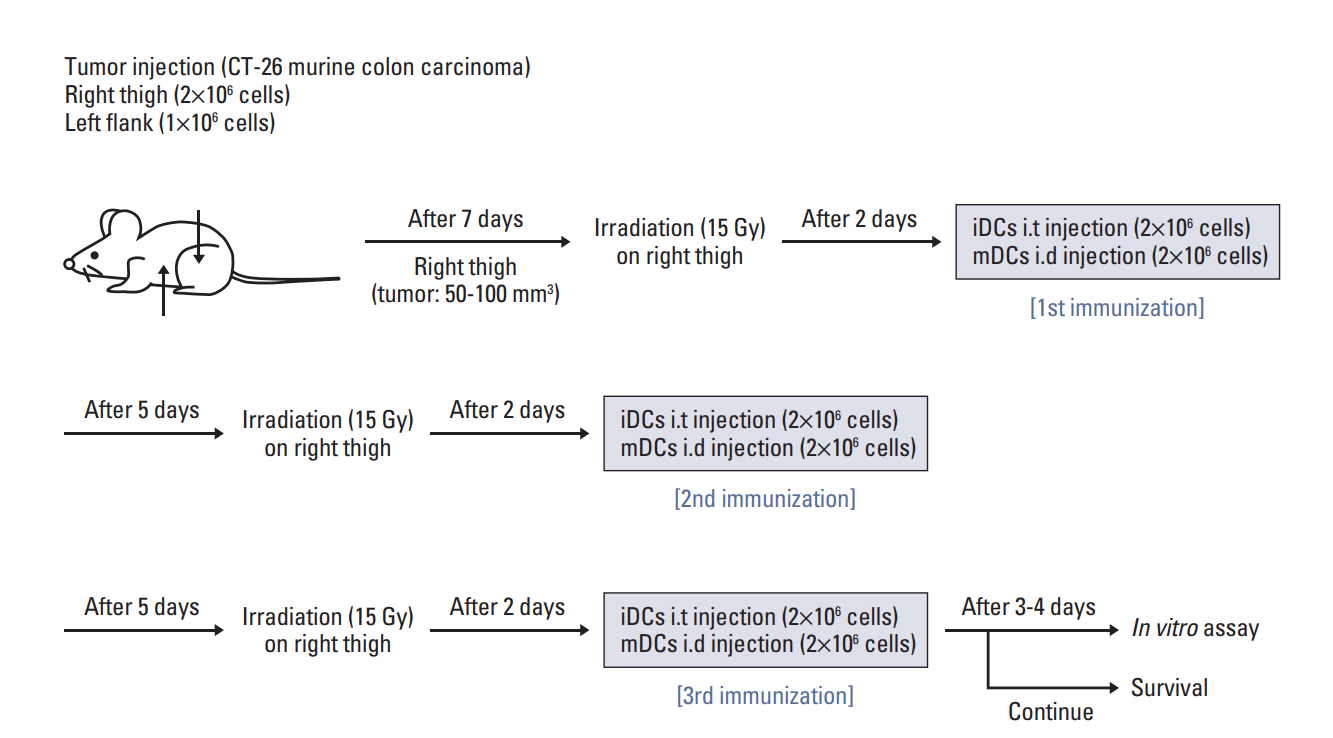
Fig. 1. Schematic diagram of the combination treatment with irradiation and immature dendritic cell injection. Murine CT-26 colon carcinoma cells were inoculated into the right hind legs and left flanks of BALB/c mice. After 7 days of injection, treatment was initiated according to the treatment protocol of each group. The treatment was repeated weekly for three cycles.
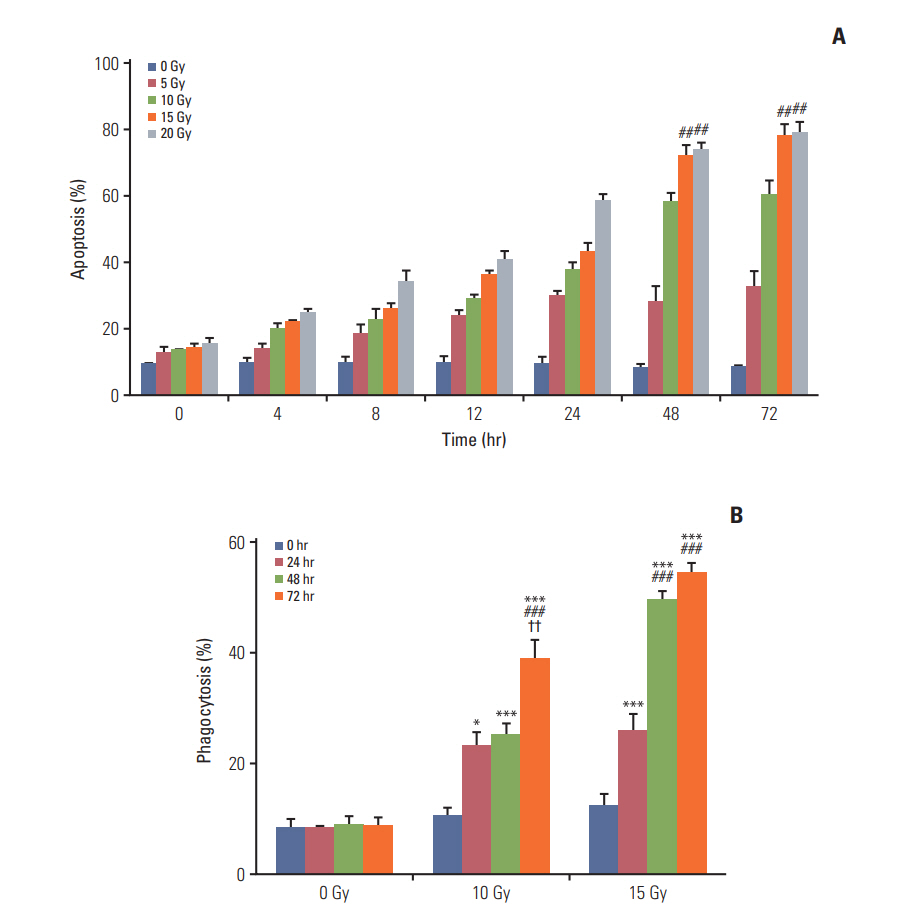
Fig. 2. Annexin V staining assay and phagocytosis assay. (A) Annexin V staining assay. Percentage apoptosis after irradiation increased with an increase in the radiation dose and incubation time. A slight difference was observed between 48 and 72 hours of incubation time. After 48-hour incubation, 15 and 20 Gy of irradiation had no significant difference in the percentage of apoptosis and exhibited significantly higher effect than 10 Gy of irradiation (p < 0.01). 10 Gy vs. 15 or 20 Gy (##p < 0.01). (B) Phagocytosis assay. A statistically significant increase in the percentage of phagocytosis was observed with an increase in the radiation dose within 48-hour incubation. After 48-hour incubation, 15 and 20 Gy of radiation showed no difference in phagocytosis. 0-Hour incubation vs. other groups (*p < 0.05, ***p < 0.001), 24-hour incubation vs. 48- or 72-hour incubation (###p < 0.001), 48-hour incubation vs. 72-hour incubation (††p < 0.01)
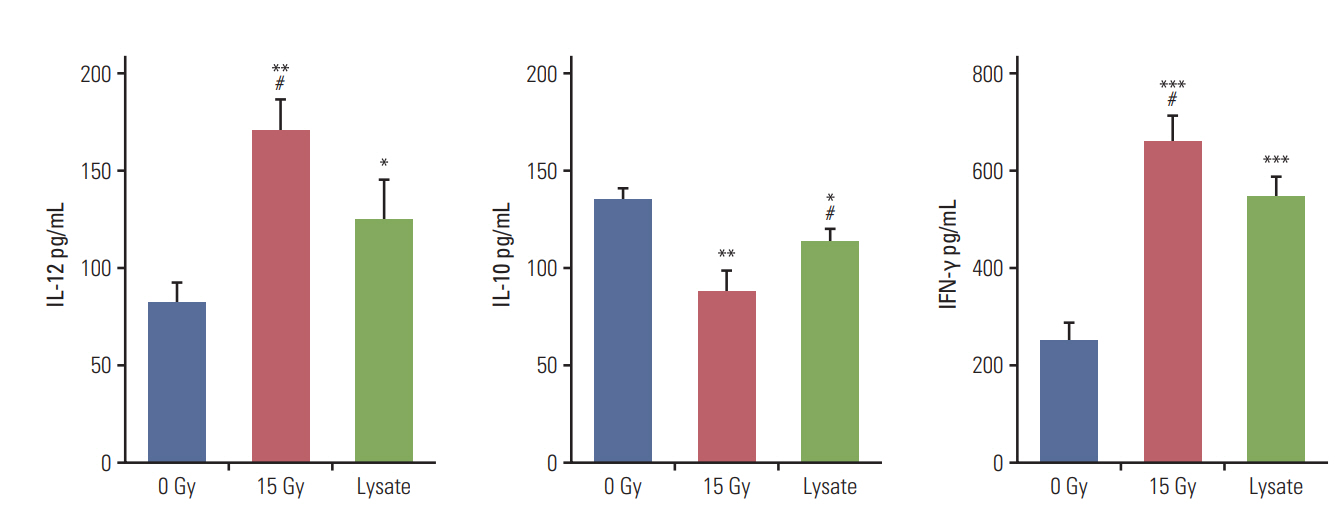
Fig. 3. Cytokine release assay. The assay was performed to verify the effectiveness of irradiation as a method to sensitize dendritic cells to present tumor-associated antigens and stimulate T cells. Tumor cell lysates were used as the positive control. The group irradiated with 15 Gy showed significantly higher interleukin (IL)-12 and interferon γ (IFN-γ) levels and lower IL-10 level than other groups. Murine CT-26 colon carcinoma cells alone with or without irradiation did not show detectable levels of the cytokines. 0 Gy vs. other groups (*p < 0.05, **p < 0.01, ***p < 0.001), 15 Gy vs. lysate (#p < 0.05).

Fig. 4. Volumes of right thigh and left flank tumors. Volumes of the right thigh tumors and the left flank tumors considered as primary tumors and distant metastatic tumors, respectively and both were measured from the date of tumor cell inoculation at an interval of 2 or 3 days. (A) Volumes of the right thigh tumors. Statistically significant difference in the tumor growth delay was observed in all groups compared with the control group. Maximum tumor growth regression was observed in the radiation therapy in combination with immature dendritic cell intratumoral injection (RT/iDC) and radiation therapy alone (RTA) groups; statistically significant difference was not reported between these two groups. (B) Volumes of the left flank tumors. The tumor growth regression was statistically significant in the RT/iDC and mature dendritic cell (mDC) groups. No difference was observed between the tumor volumes in the RTA and control groups. The RT/iDC group showed significant tumor growth delay compared with the mDC group (p < 0.001). Control vs. other groups (***p < 0.001), RTA vs. mDC or RT/iDC (###p < 0.001), mDC vs. RT/iDC (†††p < 0.001).
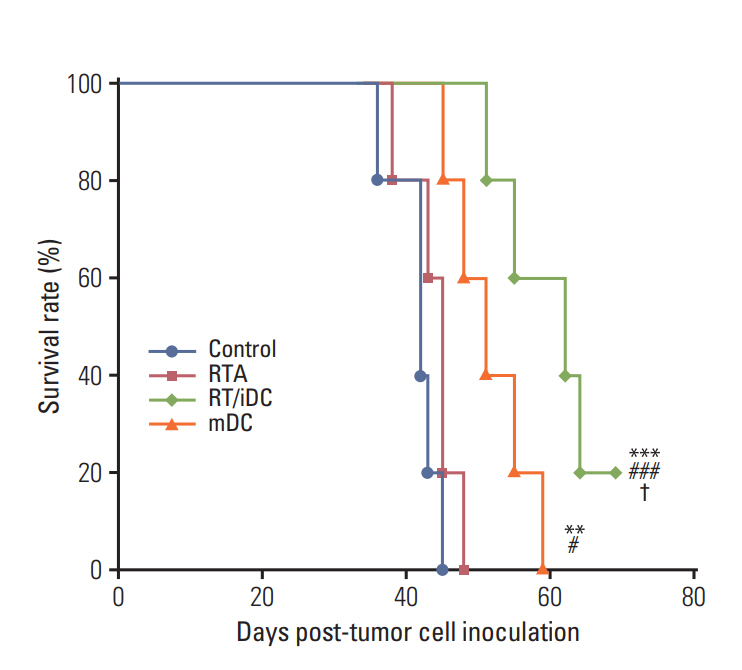
Fig. 5. Kaplan-Meier survival curve. Overall survival rate was prolonged in the radiation therapy in combination with immature dendritic cell intratumoral injection (RT/ iDC) and mature dendritic cell (mDC) groups. There was no survival gain in the radiation therapy alone (RTA) group. Most prolonged overall survival rates were observed in the RT/iDC group. Control vs. other groups (**p < 0.01, ***p < 0.001), RTA vs. mDC or RT/iDC (#p < 0.05, ###p < 0.001), mDC vs. RT/iDC (†p < 0.05).
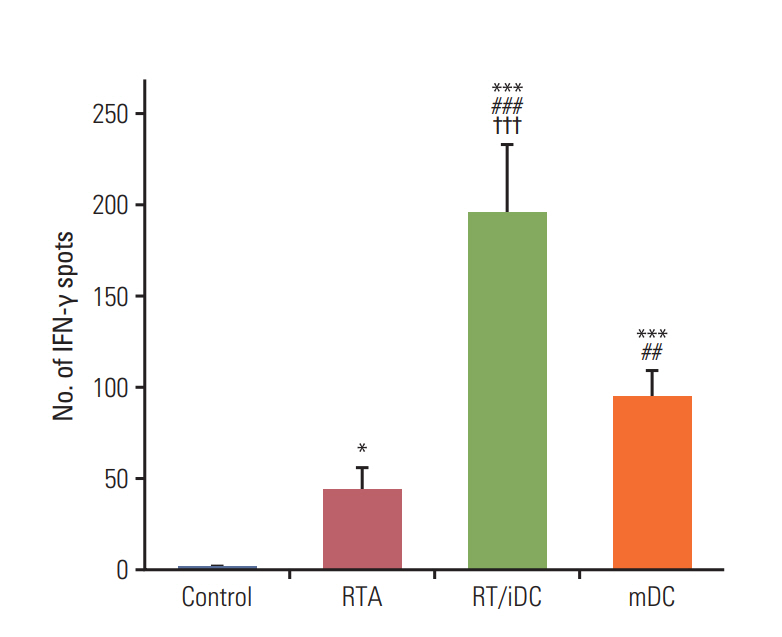
Fig. 6. Tumor-specific interferon γ (IFN-γ)‒secreting T cells. IFN-γ secretion was assessed using the enzymelinked immunospot assay. As IFN-γ secretion increased in the stimulated T cells, the analysis of IFN-γ secretion revealed the degree of T-cell stimulation after each treatment. IFN-γ level was the highest in radiation therapy in combination with immature dendritic cell intratumoral injection (RT/iDC) group, followed by the mature dendritic cell (mDC) group. A significant increase in IFN-γ level was also observed in the radiation therapy alone (RTA) group (p < 0.05). Control vs. other groups (*p < 0.05, ***p < 0.001), RTA vs. mDC or RT/iDC (##p < 0.01, ###p < 0.001), mDC vs. RT/iDC (†††p < 0.001).
Reference
-
References
1. Datta J, Terhune JH, Lowenfeld L, Cintolo JA, Xu S, Roses RE, et al. Optimizing dendritic cell-based approaches for cancer immunotherapy. Yale J Biol Med. 2014; 87:491–518.2. Palucka K, Banchereau J. Cancer immunotherapy via dendritic cells. Nat Rev Cancer. 2012; 12:265–77.
Article3. Zarnani AH, Torabi-Rahvar M, Bozorgmehr M, Zareie M, Mojtabavi N. Improved efficacy of a dendritic cell-based vaccine against a murine model of colon cancer: the helper protein effect. Cancer Res Treat. 2015; 47:518–26.
Article4. Kim SK, Yun CH, Han SH. Enhanced anti-cancer activity of human dendritic cells sensitized with gamma-irradiationinduced apoptotic colon cancer cells. Cancer Lett. 2013; 335:278–88.
Article5. Asavaroengchai W, Kotera Y, Mule JJ. Tumor lysate-pulsed dendritic cells can elicit an effective antitumor immune response during early lymphoid recovery. Proc Natl Acad Sci U S A. 2002; 99:931–6.
Article6. Fields RC, Shimizu K, Mule JJ. Murine dendritic cells pulsed with whole tumor lysates mediate potent antitumor immune responses in vitro and in vivo. Proc Natl Acad Sci U S A. 1998; 95:9482–7.7. Son CH, Bae JH, Shin DY, Lee HR, Yang K, Park YS. Antitumor effect of dendritic cell loaded ex vivo and in vivo with tumor-associated antigens in lung cancer model. Immunol Invest. 2014; 43:447–62.8. Demaria S, Ng B, Devitt ML, Babb JS, Kawashima N, Liebes L, et al. Ionizing radiation inhibition of distant untreated tumors (abscopal effect) is immune mediated. Int J Radiat Oncol Biol Phys. 2004; 58:862–70.
Article9. Koo T, Kim IA. Radiotherapy and immune checkpoint blockades: a snapshot in 2016. Radiat Oncol J. 2016; 34:250–9.
Article10. Siva S, MacManus MP, Martin RF, Martin OA. Abscopal effects of radiation therapy: a clinical review for the radiobiologist. Cancer Lett. 2015; 356:82–90.
Article11. Demaria S, Formenti SC. Sensors of ionizing radiation effects on the immunological microenvironment of cancer. Int J Radiat Biol. 2007; 83:819–25.
Article12. Deloch L, Derer A, Hartmann J, Frey B, Fietkau R, Gaipl US. Modern radiotherapy concepts and the impact of radiation on immune activation. Front Oncol. 2016; 6:141.
Article13. Derer A, Deloch L, Rubner Y, Fietkau R, Frey B, Gaipl US. Radio-immunotherapy-induced immunogenic cancer cells as basis for induction of systemic anti-tumor immune responses: pre-clinical evidence and ongoing clinical applications. Front Immunol. 2015; 6:505.
Article14. O'Garra A. Cytokines induce the development of functionally heterogeneous T helper cell subsets. Immunity. 1998; 8:275–83.15. Igietseme JU, Ananaba GA, Bolier J, Bowers S, Moore T, Belay T, et al. Suppression of endogenous IL-10 gene expression in dendritic cells enhances antigen presentation for specific Th1 induction: potential for cellular vaccine development. J Immunol. 2000; 164:4212–9.
Article16. Weiss EM, Frey B, Rodel F, Herrmann M, Schlucker E, Voll RE, et al. Ex vivo- and in vivo-induced dead tumor cells as modulators of antitumor responses. Ann N Y Acad Sci. 2010; 1209:109–17.17. Chi KH, Liu SJ, Li CP, Kuo HP, Wang YS, Chao Y, et al. Combination of conformal radiotherapy and intratumoral injection of adoptive dendritic cell immunotherapy in refractory hepatoma. J Immunother. 2005; 28:129–35.
Article18. Slota M, Lim JB, Dang Y, Disis ML. ELISpot for measuring human immune responses to vaccines. Expert Rev Vaccines. 2011; 10:299–306.
Article19. Benedict SH, Yenice KM, Followill D, Galvin JM, Hinson W, Kavanagh B, et al. Stereotactic body radiation therapy: the report of AAPM Task Group 101. Med Phys. 2010; 37:4078–101.
Article20. Kang J, Demaria S, Formenti S. Current clinical trials testing the combination of immunotherapy with radiotherapy. J Immunother Cancer. 2016; 4:51.
Article21. Sharabi AB, Tran PT, Lim M, Drake CG, Deweese TL. Stereotactic radiation therapy combined with immunotherapy: augmenting the role of radiation in local and systemic treatment. Oncology (Williston Park). 2015; 29:331–40.22. Yovino S, Kleinberg L, Grossman SA, Narayanan M, Ford E. The etiology of treatment-related lymphopenia in patients with malignant gliomas: modeling radiation dose to circulating lymphocytes explains clinical observations and suggests methods of modifying the impact of radiation on immune cells. Cancer Invest. 2013; 31:140–4.
Article23. Krysko O, Love Aaes T, Bachert C, Vandenabeele P, Krysko DV. Many faces of DAMPs in cancer therapy. Cell Death Dis. 2013; 4:e631.
Article24. Proskuryakov SY, Konoplyannikov AG, Gabai VL. Necrosis: a specific form of programmed cell death? Exp Cell Res. 2003; 283:1–16.
Article25. Vandenabeele P, Galluzzi L, Vanden Berghe T, Kroemer G. Molecular mechanisms of necroptosis: an ordered cellular explosion. Nat Rev Mol Cell Biol. 2010; 11:700–14.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Top Ten Lessons Learned from Trials in Oligometastatic Cancers
- Role of Radiation Therapy for Non-small Cell Lung Cancer: Focused on Stereotactic Ablative Radiation Therapy in Stage I
- Stereotactic Body Radiotherapy for Early Stage Lung Cancer
- A Case of Achieving Complete Remission with Stereotactic Body Radiation Therapy in Patients with Hepatocellular Carcinoma with Macrovascular Invasion after Repeated Transarerial Chemoembolization
- Stereotactic Body Radiation Therapy for Hepatocellular Carcinoma
