Effects of Prolotherapy on Medial Collateral Ligament Bursitis of the Knee Joint Identified with High Resolution Ultrasound
- Affiliations
-
- 1Dr. Kim's Orthopaedic Clinic, Jincheon, Korea. topofos@naver.com
- KMID: 2461239
- DOI: http://doi.org/10.4055/jkoa.2019.54.5.469
Abstract
- Medial knee joint pain is a common problem in the field of orthopedics. In these patients, a high resolution ultrasound examination can reveal medial collateral ligament (MCL) bursitis, meniscal cyst, degeneration changes to the MCL and meniscal protrusion etc. Prolotherapy is effective in these patients. The author performed prolotherapy for MCL bursitis of the knee joint, and confirmed the disappearance of the bursitis using high resolution ultrasound.
Figure
-
Figure 1 Radiographics of the right knee. (A) Anteroposterior; (B) Lateral; (C) Skyline. No definite bony abnormality.
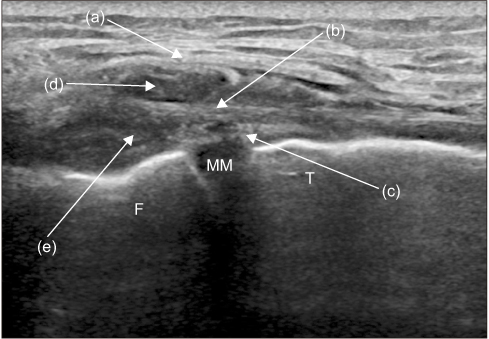
Figure 2 Long axis scan (before prolotherapy). Inhomogeneous hypoechoic lesion on the knee medial side. Crural fascia (a), superficial medial collateral ligament (MCL) (b), deep MCL (c), hypoechoic lesion between the crural fascia and superficial fiber of the MCL (d), hypoechoic lesion between the superficial fiber of the MCL and deep fiber of the MCL (e). F, femur; MM, medial meniscus; T, tibia.
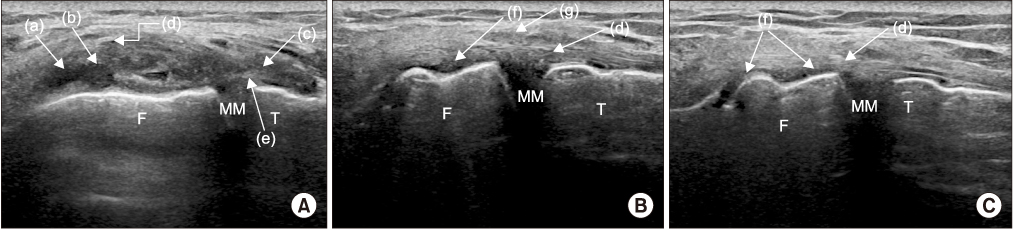
Figure 3 Long axis scan. (A) Before prolotherapy. (B, C) After prolotherapy (5 months later). Inhomogeneous hypoechoic lesion on the knee medial side (a–c), superficial fiber of the medial collateral ligament (MCL) (d), deep fiber of the MCL (e), disappearance of previous hypoechoic lesion (f), crural fascia (g). F, femur; MM, medial meniscus; T, tibia.
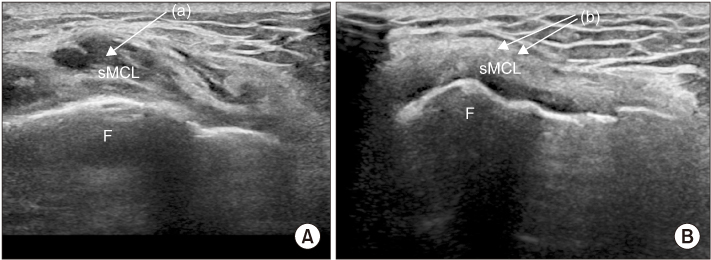
Figure 4 Short axis scan. (A) Before prolotherapy. (B) After prolotherapy (5 months later). Inhomogeneous hypoechoic lesion on the knee medial side (a), the disappearance of previous hypoechoic lesion (b). F, femur; sMCL, superficial fiber of the medial collateral ligament.
Reference
-
1. Estrada M, Royero M, Arismendy D, Alzate JB. Cystic lesions of the knee. Pictorial Review. Rev Colomb Radiol. 2015; 26:4121–4132.2. Ombregt L. A system of orthopaedic medicine. 3rd ed. Edinburgh: Curchill Livingstone;2013. p. 668–670.3. Ombregt L. A system of orthopaedic medicine. 3rd ed. Edinburgh: Curchill Livingstone;2013. p. 105–106.4. Ravin TH, Cantieri MS, Pasquarello GJ. Principles of prolotherapy. Denver: American Academy of MuSculoskeltal Medicine;2008. p. 9–10.5. Lee JK, Yao L. Tibial collateral ligament bursa: MR imaging. Radiology. 1991; 178:855–857.6. Jose J, Schallert E, Lesniak B. Sonographically guided therapeutic injection for primary medial (tibial) collateral bursitis. J Ultrasound Med. 2011; 30:257–261.7. Shon MS, Yoo JC. Prolotherapy in orthopedic field. J Korean Orthop Ultrasound Soc. 2011; 4:101–110.8. Kim YU. Prolotherapy for the lower extremities. J Korean Orthop Ultrasound Soc. 2009; 2:37–44.9. Fullerton BD. High-resolution ultrasound and magnetic resonance imaging to document tissue repair after prolotherapy: a report of 3 cases. Arch Phys Med Rehabil. 2008; 89:377–385.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Effects of Prolotherapy on Knee Joint Pain due to Ligament Laxity
- Radiologic analysis of the medial collateral ligament rupture
- An Operative Treatment of Injured Medial Structures of the Knee
- Comparative Analysis of Medial Collateral Ligament Grade III injury of the Knee
- Anchoring to the Crural Fascia for Avulsion of the Medial Collateral Ligament from the Tibia
