The Effect of Pain Reduction during Headframe Fixation for Stereotactic Radiosurgery by the Preceded Local Anesthesia under the Needle Cap Guidance
- Affiliations
-
- 1Department of Neurosurgery & Medical Research Institute, Pusan National University Hospital, Pusan National University School of Medicine, Busan, Korea. mdcwh@naver.com
- 2Department of Neurosurgery, Pusan National University Yangsan Hospital, Pusan National University School of Medicine, Yangsan, Korea.
- KMID: 2461186
- DOI: http://doi.org/10.14791/btrt.2019.7.e31
Abstract
- BACKGROUND
Gamma knife radiosurgery (GKRS) has become a major alternative in the neurosurgical field. However, many patients complained of considerable discomfort during the fixation of rigid headframe. This study investigated whether our modified procedure could reduce fixation-related pain.
METHODS
Sixty-six patients who underwent GKRS were enrolled in this study. Thirty-one patients (Group A) underwent the conventional subcutaneous infiltration technique, and 35 patients (Group B) did the modified procedure. In group A, the headframe was held in position by an assistant, and local anesthetics were injected subcutaneously using a 23-gauge spinal needle at pinning sites. Subsequently, pins were applied according to measurements based on spinal needle depth. In group B, with the frame held in position by an assistant, pin sites were marked with a surgical pen under the guidance of needle cap placed on the pin holes. The head frame was then removed, and local anesthetics were injected subcutaneously and periosteally at each marked pin site using a 26-gauge needle. The headframe was then repositioned 5 minutes after local infiltration, and pins were applied according to measurements based on spinal needle depth. To evaluate pain severity during procedures, visual analogue scale (VAS) scores were recorded during local infiltration and frame placement with pins. The pain scores of the two groups were analyzed statistically.
RESULTS
Group B had a significantly lower VAS score during frame placement than group A (7.26 vs. 3.61; p<0.001), and mean VAS score at local infiltration was also significantly lower in group B (4.74 vs. 3.74; p=0.008).
CONCLUSION
Patients in group B experienced significantly less pain than those in group A during pin placement. Pre-fixation time advanced local anesthesia might reduce pain during stereotactic procedures, and the use of a 26-gauge needle appeared in less pain during local infiltration.
Figure
-

Fig. 1 Pin sites were marked with surgical pen under the guidance of needle cap positioned through the pin hole in the frame bar.
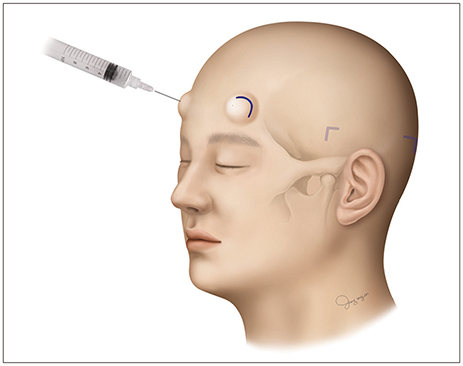
Fig. 2 Local anesthetic solution was injected periosteally and subcutaneously at each marked pin site using a 26 gauge sharp-beveled needle.

Fig. 3 Pin length was measured by spinal needle depth, before applying to the marking sites of patient head.
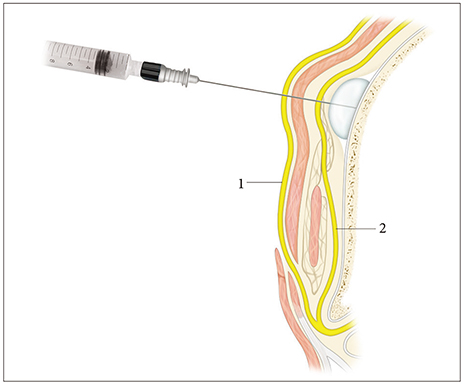
Fig. 4 Anesthetic solution was injected into the periosteal space and formed a bleb-like cyst. 1, medial branch of the supraorbital nerve; 2, lateral branch of the supraorbital nerve.
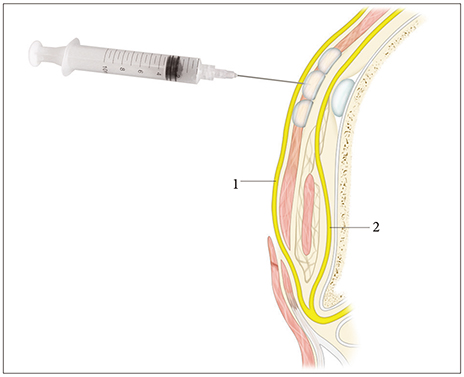
Fig. 5 Anesthetic solution was injected into the periosteal and subcutaneous spaces to anesthetize medial and lateral branches of the supraorbital nerve. 1, medial branch of the supraorbital nerve; 2, lateral branch of the supraorbital nerve.
Reference
-
1. Guridi J, Obeso JA, Rodriguez-Oroz MC, Lozano AA, Manrique M. L-dopa-induced dyskinesia and stereotactic surgery for Parkinson's disease. Neurosurgery. 2008; 62:311–323. discussion 323-5.
Article2. Kondziolka D, Lunsford LD, Flickinger JC. The application of stereotactic radiosurgery to disorders of the brain. Neurosurgery. 2008; 62 Suppl 2:707–719. discussion 719-20.
Article3. Kondziolka D, Martin JJ, Flickinger JC, et al. Long-term survivors after gamma knife radiosurgery for brain metastases. Cancer. 2005; 104:2784–2791.
Article4. Kondziolka D, Perez B, Flickinger JC, Habeck M, Lunsford LD. Gamma knife radiosurgery for trigeminal neuralgia: results and expectations. Arch Neurol. 1998; 55:1524–1529.5. Nicolato A, Foroni R, Pellegrino M, et al. Gamma knife radiosurgery in meningiomas of the posterior fossa. Experience with 62 treated lesions. Minim Invasive Neurosurg. 2001; 44:211–217.
Article6. Wang DD, Lau D, Rolston JD, Englot DJ, Sneed PK, McDermott MW. Pain experience using conventional versus angled anterior posts during stereotactic head frame placement for radiosurgery. J Clin Neurosci. 2014; 21:1538–1542.
Article7. Liang CL, Lu K, Liliang PC, Chung MC, Chi SC, Chen HJ. Topical anesthetic EMLA for postoperative wound pain in stereotactic gamma knife radiosurgery: a perspective, randomized, placebo-controlled study. Minim Invasive Neurosurg. 2011; 54:75–78.
Article8. Duenas SM, Pun J, Radwan HA, Akerman M, Schulder M. A randomized trial on the efficacy of topical anesthesia for pain reduction during frame placement for gamma knife radiosurgery. Stereotact Funct Neurosurg. 2016; 94:259–264.
Article9. Watson R, Leslie K. Nerve blocks versus subcutaneous infiltration for stereotactic frame placement. Anesth Analg. 2001; 92:424–427.
Article10. Konofaos P, Soto-Miranda MA, Ver Halen J, Fleming JC. Supratrochlear and supraorbital nerves: an anatomical study and applications in the head and neck area. Ophthalmic Plast Reconstr Surg. 2013; 29:403–408.11. Knize DM. A study of the supraorbital nerve. Plast Reconstr Surg. 1995; 96:564–569.
Article12. Malet T, Braun M, Fyad JP, George JL. Anatomic study of the distal supraorbital nerve. Surg Radiol Anat. 1997; 19:377–384.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Stereotactic Body Radiotherapy for Early Stage Lung Cancer
- Ultrasound-guided Fine-needle Aspiration Biopsy of Thyroid Nodules: Comparison of the Pain Scale according to the Application of Local Anesthesia
- The Role of Stereotactic Radiosurgery in Metastasis to the Spine
- The mixed era of stereotactic radiosurgery and radiotherapy
- Evaluation of an Experimentally Designed Stereotactic Guidance System for Determining Needle Entry Point during Uniplanar Fluoroscopy-guided Intervention
