Prosthetic rehabilitation of soft palate resection edentulous patient with maxillary obturator
- Affiliations
-
- 1Department of Prosthodontics, School of Dentistry, Seoul National University, Seoul, Republic of Korea. 0504heo@hanmail.net
- KMID: 2461156
- DOI: http://doi.org/10.4047/jkap.2019.57.4.475
Abstract
- This report is a case of 76-year old male patient who had difficulty in swallowing, pronunciation and suffered regurgitation of food. The patient lacks uvula and both tonsils, had short palatoglossal arch and soft palate, as well as defective left palatopharyngeal arch. The height and width of the soft palate defect were measured by reconstructing the Computed Tomography (CT) image in three dimensions. Phonation and soft palate obstructing ability were examined by nasometry and nasal endoscopy. Evaluations on phonetics and swallowing were done and improvements were shown. The patient was satisfied with the results of treatment.
MeSH Terms
Figure
-

Fig. 1 Initial photographs. (A) Maxillary occlusal view, (B) Mandibular occlusal view, (C) Panoramic radiograph, (D) Frontal view on right side, (E) Frontal view, (F) Frontal view on left side, (G, H) There is defect on soft palate and pharyngeal portion.
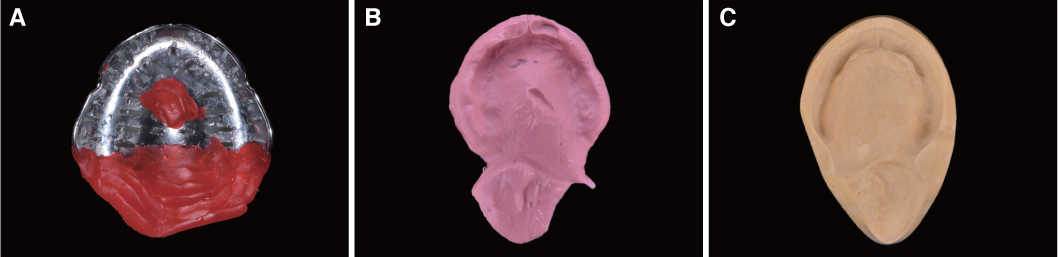
Fig. 2 Preliminary impression. (A) Tray and utility wax, (B) Impression using alginate, (C) Preliminary cast.

Fig. 3 (A) Impression for Master cast, (B) Master cast.
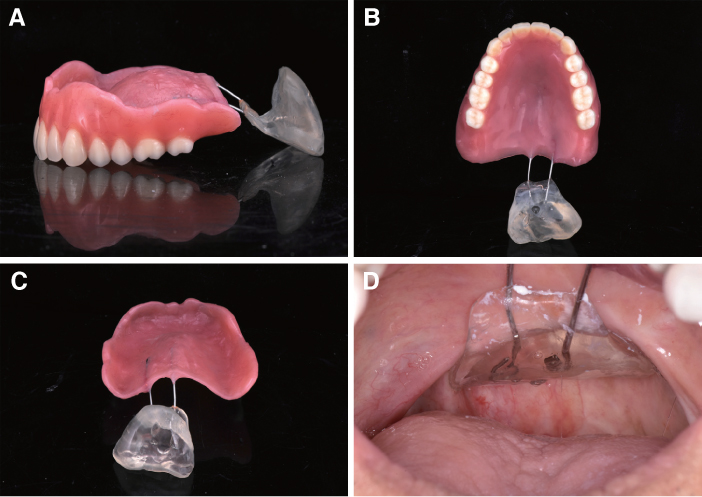
Fig. 4 Temporary denture. (A) Lateral view, (B) occlusal view, (C) Rear view, (D) Intraoral photo after delivery.

Fig. 5 (A) CT sagittal view, (B) CT horizontal view, (C, D) Reconstructing defect area image using Seg 3D.
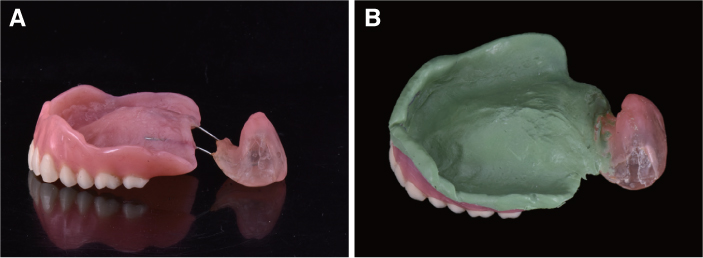
Fig. 6 (A) Functional impression for obturator area, (B) Impression for definitive obturator.
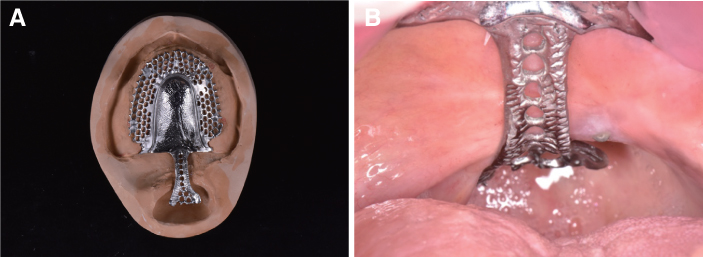
Fig. 7 Metal framework. (A) Upper framework including velar and pharyngeal part, (B) Intraoral try-in.
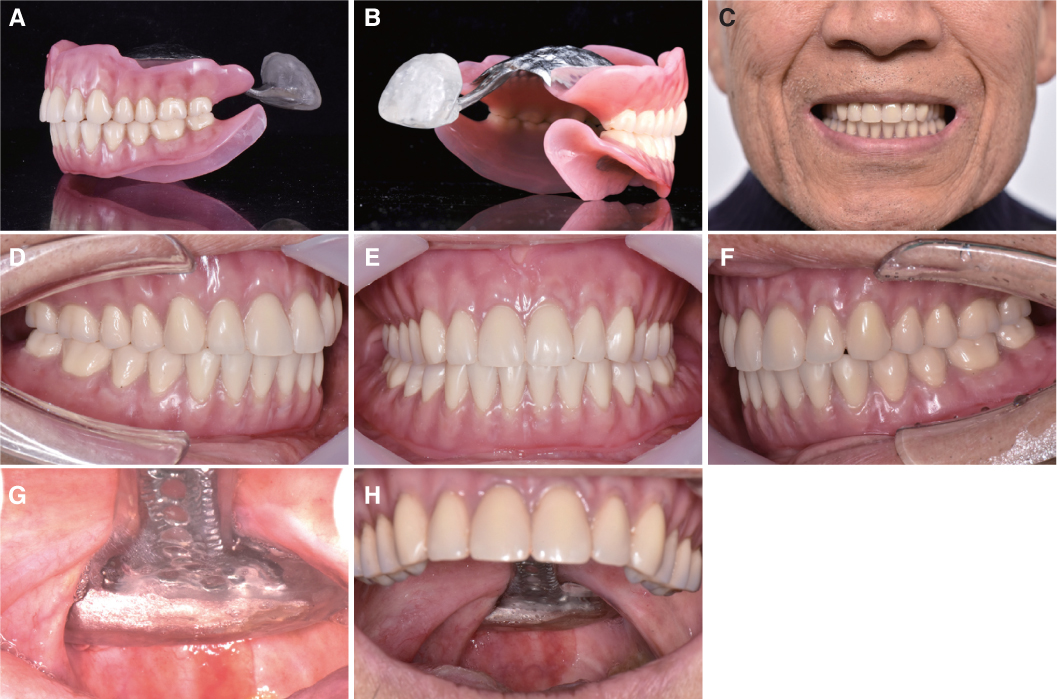
Fig. 8 Definitive prosthesis. (A) Lateral view, (B) Rear view, (C) External oral photo, (D) Frontal view on right side, (E) Frontal view, (F) Frontal view on left side, (G) velar and pharyngeal area, (H) Frontal view on velar and pharyngeal area.
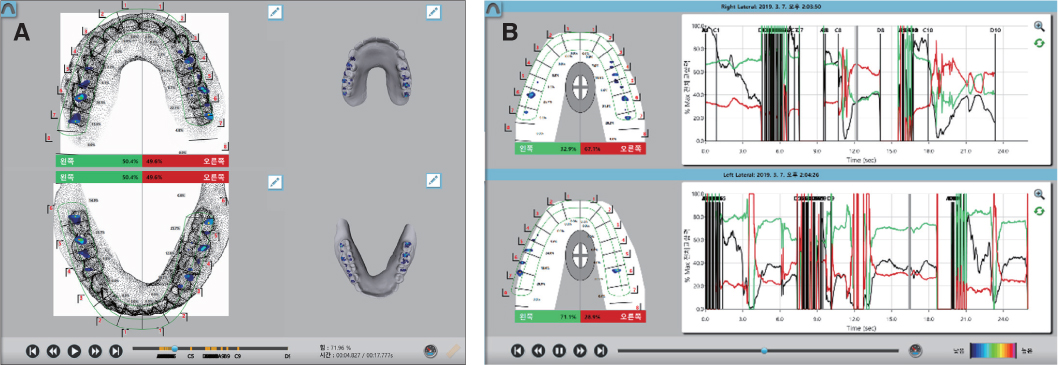
Fig. 9 T-scan result. (A) Centric occlusal, (B) Right and Left lateral excursion.
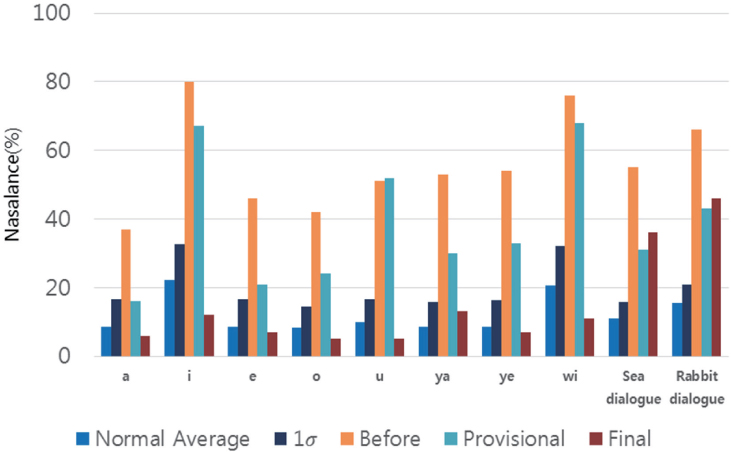
Fig. 10 Nasometry chart.
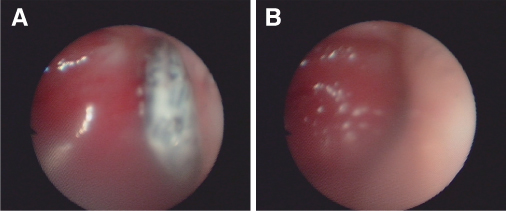
Fig. 11 Nasal endoscope image. (A) Rest state, (B) Closed state on pharyngeal area.
Reference
-
1. Schneider E, Shprintzen RJ. A survey of speech pathologists: current trends in the diagnosis and management of velopharyngeal insufficiency. Cleft Palate J. 1980; 17:249–253.2. Warren DW. A physiologic approach to cleft palate prosthesis. J Prosthet Dent. 1965; 15:770–778.
Article3. Desjardins RP. Obturator prosthesis design for acquired maxillary defects. J Prosthet Dent. 1978; 39:424–435.
Article4. Veau V, Borel S. Division palatine: Anatomie-chirurgie phonétique. Paris: Masson et Cie;1931. p. 568.5. Johns DF, Rohrich RJ, Awada M. Velopharyngeal incompetence: a guide for clinical evaluation. Plast Reconstr Surg. 2003; 112:1890–1897.6. Warren DW. Perci: a method for rating palatal efficiency. Cleft Palate J. 1979; 16:279–285.7. Raj N, Raj V, Aeran H. Interim palatal lift prosthesis as a constituent of multidisciplinary approach in the treatment of velopharyngeal incompetence. J Adv Prosthodont. 2012; 4:243–247.
Article8. Fletcher SG, Frost SD. Quantitative and graphic analysis of prosthetic treatment for “nasalance” in speech. J Prosthet Dent. 1974; 32:284–291.
Article9. Marshall RC, Jones RN. Effects of a palatal lift prosthesis upon the speech intelligibility of a dysarthric patient. J Prosthet Dent. 1971; 25:327–333.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Removable prosthetic rehabilitation in patient with maxillofacial defects caused by gunshot: A case report
- Prosthetic rehabilitation by double-processing technique for edentulous patient with soft palate defect after maxillectomy: A case report
- Prosthetic rehabilitation of partially edentulous patient after maxillectomy: A case report
- Prosthetic rehabilitation of a fully edentulous patient after maxillectomy: A case report
- Prosthetic rehabilitation using an obturator in a fully edentulous patient who had partial maxillectomy
