Morel-Lavallée Lesion in the Sacrococcygeal Area with Associated Coccygeal Fracture
- Affiliations
-
- 1Department of Neurosurgery, College of Medicine, Chosun University, Gwangju, Korea. chosunns@chosun.ac.kr
- 2Department of Plasticsurgery, College of Medicine, Chosun University, Gwangju, Korea.
- 3Department of Neurosurgery, Dong-A Hospital, Gwangju, Korea.
- KMID: 2461133
- DOI: http://doi.org/10.13004/kjnt.2019.15.e16
Abstract
- A Morel-Lavallée lesion is a posttraumatic, closed internal degloving injury caused by shearing force abruptly separating the skin and superficial fascia from the deep fascia and creating a potential space. Blood, lymphatic fluid, and debris collect and fill the space. The most commonly affected sites are the thigh, knee, hip, and pelvic area, but the lesion can occur anywhere in the body. Among various treatments, surgical procedure is a good option if the lesion is chronic and a thick peripheral capsule has developed. We report an uncommon case of a chronic Morel-Lavallée lesion in the sacrococcygeal area, a rarely reported location, with an associated coccygeal fracture and dislocation.
Keyword
Figure
-

FIGURE 1 Lateral radiograph of the sacrococcygeal area shows fracture and dislocation of the coccyx (red arrow).

FIGURE 2 Photograph shows an extensive swelling lesion at the midline of the sacrococcygeal area.
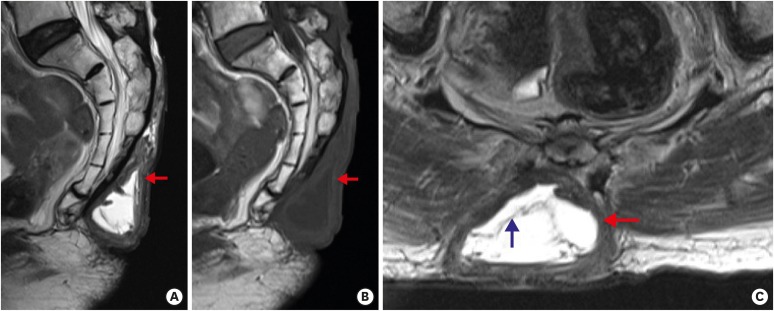
FIGURE 3 Magnetic resonance imaging of the lesion. Sagittal T2-weighted (A), sagittal T1-weighted (B), and axial T2-weighted (C) images demonstrate a fluid collection above the deep fascia, with high signal intensity on T2-weighted images and low signal intensity on T1-weighted images in the sacrococcygeal area. There is a hypointense thick peripheral capsule (red arrow) with internal septations (blue arrow).

FIGURE 4 Postoperative photograph immediately after removal of the fluctuant mass and closure of wound with a flap. A suction drainage tube is seen in the left gluteal area.
Reference
-
1. Bansal A, Bhatia N, Singh A, Singh AK. Doxycycline sclerodesis as a treatment option for persistent Morel-Lavallée lesions. Injury. 2013; 44:66–69. PMID: 22204771.
Article2. Bomela LN, Basson H, Motsitsi NS. Morel-Lavallée lesion: a review. SA Orthop J. 2008; 7:34–41.3. De Coninck T, Vanhoenacker F, Verstraete K. Imaging features of Morel-Lavallée lesions. J Belg Soc Radiol. 2017; 101:15.
Article4. Diviti S, Gupta N, Hooda K, Sharma K, Lo L. Morel-Lavallee lesions: review of pathophysiology, clinical findings, imaging findings and management. J Clin Diagn Res. 2017; 11:TE01–TE04.5. Greenhill D, Haydel C, Rehman S. Management of Morel-Lavallée lesions. Orthop Clin North Am. 2016; 47:115–125. PMID: 26614926.6. Hudson DA. Missed closed degloving injuries: late presentation as a contour deformity. Plast Reconstr Surg. 1996; 98:334–337. PMID: 8764723.
Article7. Hussein K, White B, Sampson M, Gupta S. Pictorial review of Morel-Lavallée lesions. J Med Imaging Radiat Oncol. 2019; 63:212–215. PMID: 30652431.
Article8. Kalaci A, Karazincir S, Yanat AN. Long-standing Morel-Lavallée lesion of the thigh simulating a neoplasm. Clin Imaging. 2007; 31:287–291. PMID: 17599627.9. Lin HL, Lee WC, Kuo LC, Chen CW. Closed internal degloving injury with conservative treatment. Am J Emerg Med. 2008; 26:254.e5–254.e6.
Article10. Luria S, Applbaum Y, Weil Y, Liebergall M, Peyser A. Talc sclerodhesis of persistent Morel-Lavallée lesions (posttraumatic pseudocysts): case report of 4 patients. J Orthop Trauma. 2006; 20:435–438. PMID: 16825972.11. Mellado JM, Pérez del Palomar L, Díaz L, Ramos A, Saurí A. Long-standing Morel-Lavallée lesions of the trochanteric region and proximal thigh: MRI features in five patients. AJR Am J Roentgenol. 2004; 182:1289–1294. PMID: 15100134.
Article12. Mulcahy MJ, Ball JR. The Morel-Lavallée lesion in thoracolumbar spine trauma-two index cases. J Spine Surg. 2018; 4:654–657. PMID: 30547132.
Article13. Penaud A, Quignon R, Danin A, Bahé L, Zakine G. Alcohol sclerodhesis: an innovative treatment for chronic Morel-Lavallée lesions. J Plast Reconstr Aesthet Surg. 2011; 64:e262–e264. PMID: 21741333.
Article14. Rha EY, Kim DH, Kwon H, Jung SN. Morel-Lavallee lesion in children. World J Emerg Surg. 2013; 8:60. PMID: 24377750.
Article15. Spain JA, Rheinboldt M, Parrish D, Rinker E. Morel-Lavallée injuries: a multimodality approach to imaging characteristics. Acad Radiol. 2017; 24:220–225. PMID: 28087046.16. Tejwani SG, Cohen SB, Bradley JP. Management of Morel-Lavallee lesion of the knee: twenty-seven cases in the national football league. Am J Sports Med. 2007; 35:1162–1167. PMID: 17351119.17. Tseng S, Tornetta P 3rd. Percutaneous management of Morel-Lavallee lesions. J Bone Joint Surg Am. 2006; 88:92–96.
Article18. Tsur A, Galin A, Kogan L, Loberant N. Morel-Lavallée syndrome after crush injury. Harefuah. 2006; 145:111–113. 166PMID: 16509414.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Extensive Multiple Morel-Lavallée Lesions: A Case Report
- Occurrence and Surgical Treatment of Massive Morel-Lavallée Lesion after Large-Volume Liposuction: A Rare Clinical Case
- Hemorrhagic Shock in a Patient with a Morel-Lavallée Lesion Combined with Active Arterial Bleeding without Fracture
- Coccygeal Morphology on Multislice Computed Tomography in a Tertiary Hospital in India
- Sclerotherapy Using Abnobaviscum for the Extensive Recurrent Chronic Morel-Lavallée Lesions - A Case Report -
