Uterine Artery Embolization for Leiomyomas and Adenomyosis: A Pictorial Essay Based on Our Experience from 1300 Cases
- Affiliations
-
- 1Department of Radiology, Research Institute of Radiological Science, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea. mdkim@yuhs.ac
- KMID: 2459165
- DOI: http://doi.org/10.3348/kjr.2019.0205
Abstract
- Since its introduction in 1995, uterine artery embolization (UAE) has become an established option for the treatment of leiomyomas. Identification of a leiomyoma using arteriography improves the ability to perform effective UAE. UAE is not contraindicated in a pedunculated subserosal leiomyoma. UAE in a cervical leiomyoma remains a challenging procedure. A leiomyoma with high signal intensity on T2-weighted imaging responds well to UAE, but a malignancy with similar radiological features should not be misdiagnosed as a leiomyoma. Administration of gonadotropin-releasing hormone agonists before UAE is useful in selected patients and is not a contraindication for the procedure. The risk of subsequent re-intervention 5 years after UAE is approximately 10%, which represents an acceptable profile. UAE for adenomyosis is challenging; initial embolization using small particles can achieve better success than that by using larger particles. An intravenous injection of dexamethasone prior to UAE, followed by a patient-controlled analgesia pump and intra-arterial administration of lidocaine after the procedure, are useful techniques to control pain. Dexmedetomidine is an excellent supplemental sedative, showing a fentanyl-sparing effect without causing respiratory depression. UAE for symptomatic leiomyoma is safe and can be an alternative to surgery in most patients with a low risk of re-intervention.
Keyword
MeSH Terms
-
Adenomyosis*
Analgesia, Patient-Controlled
Angiography
Dexamethasone
Dexmedetomidine
Gonadotropin-Releasing Hormone
Humans
Injections, Intravenous
Leiomyoma*
Lidocaine
Magnetic Resonance Imaging
Respiratory Insufficiency
Uterine Artery Embolization*
Uterine Artery*
Uterus
Dexamethasone
Dexmedetomidine
Gonadotropin-Releasing Hormone
Lidocaine
Figure
-
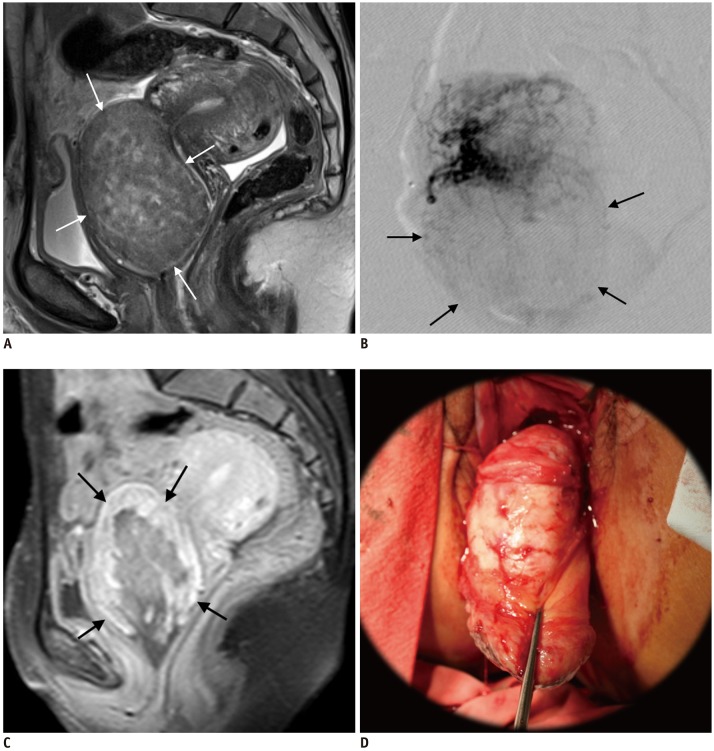
Fig. 1 44-year-old woman presenting with heavy bleeding due to cervical leiomyoma.A. Sagittal T2WI MRI shows 7-cm cervical leiomyoma (arrows). B. Uterine arteriography reveals hypovascular leiomyoma (arrows). C. One month after UAE, patient presented with vaginal expulsion of leiomyoma, which was partially infarcted and viable (arrows) on contrast-enhanced MRI. D. Hysteroscopic resection was performed under general anesthesia. T2WI = T2-weighted imaging, UAE = uterine artery embolization
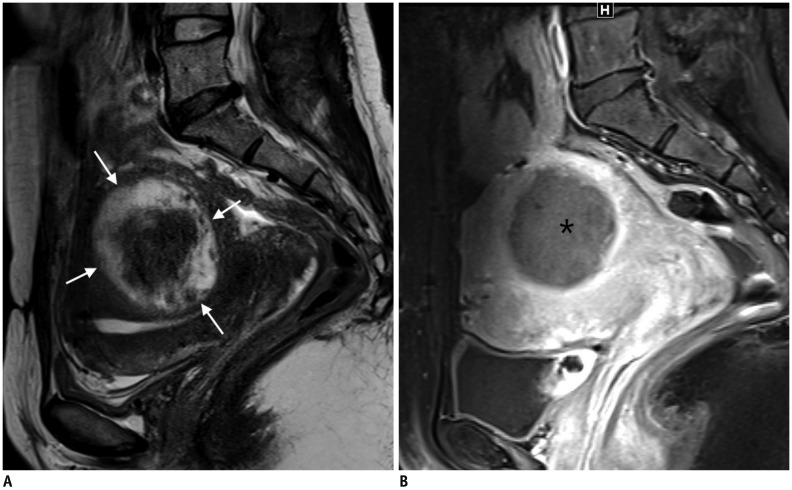
Fig. 2 Leiomyoma with high SI on T2WI.A. 41-year-old woman with leiomyoma with high SI on T2WI (arrows). B. Patient underwent failed HiFU. UAE was performed, and 3-month follow-up MRI showed complete necrosis of leiomyoma (asterisk). HiFU = high-intensity focused ultrasound, SI = signal intensity
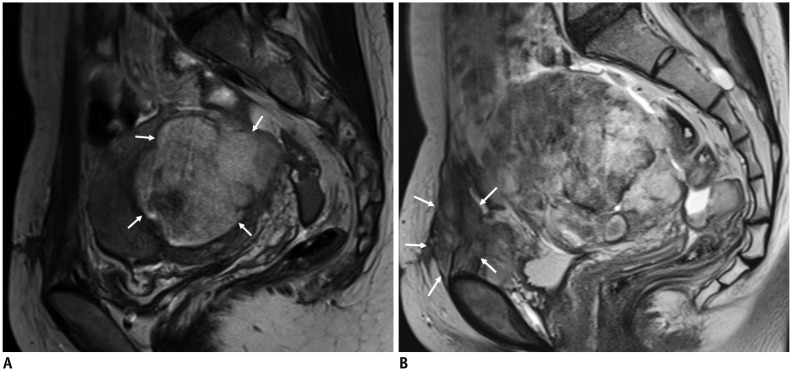
Fig. 3 UAE for malignant tumors misdiagnosed as leiomyomas.31-year-old woman underwent myomectomy at another hospital 4 months prior, and histopathological examination revealed leiomyoma.A. MRI showed tumor 7 cm in size (arrows) with high SI; thus, leiomyoma was diagnosed based on pathologic report. B. 3-month follow-up MRI after UAE revealed exacerbation of uterine tumor with peritoneal seeding (arrows) as well as seeding along incision scar. Spindle cell sarcoma of uterus was confirmed.
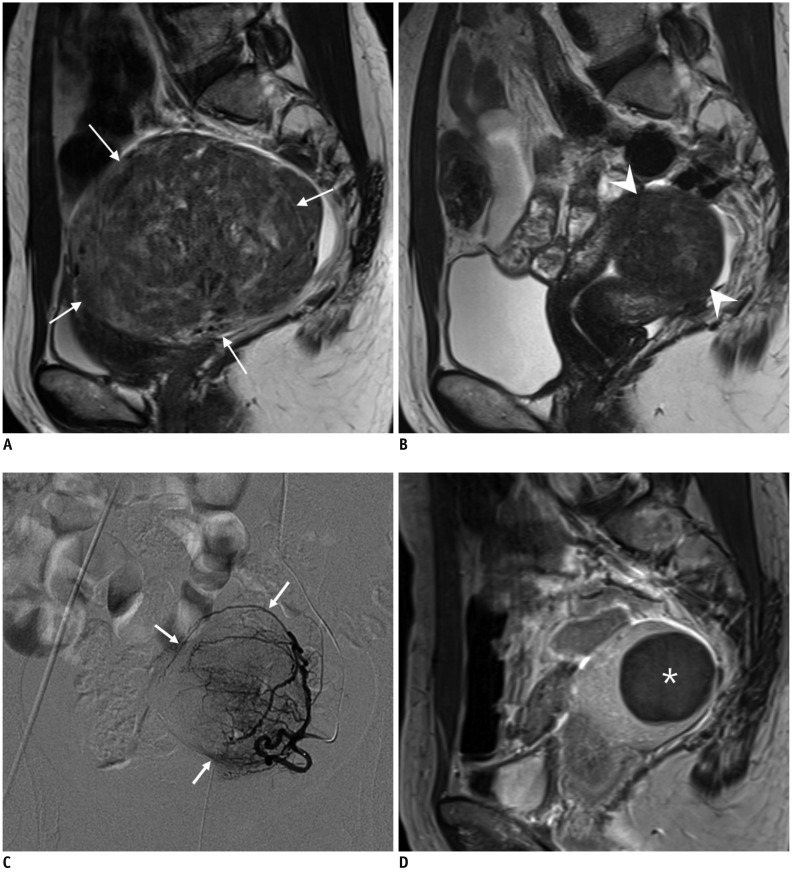
Fig. 4 GnRH agonists for large leiomyoma prior to UAE.A. 46-year-old woman presented with voiding difficulty. MRI revealed 10-cm large leiomyoma (arrows). B. After two doses of GnRH agonists, leiomyoma reduced to 4.7 cm in size (arrowheads), 85% volume reductio. C. Left uterine arteriography demonstrated leiomyoma (arrows). D. Complete infarction of leiomyoma (asterisk) was seen on 3-month follow-up MRI. GnRH = gonadotropin-releasing hormone
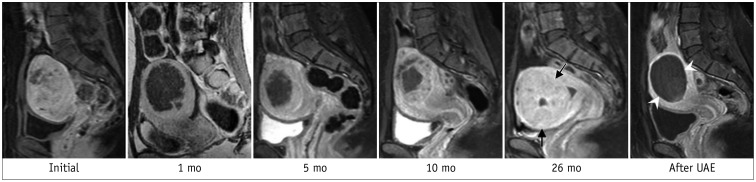
Fig. 5 44-year-old woman presenting with recurrent leiomyoma after HiFU.Serial MRI revealed complete regrowth of leiomyoma (arrows) 26 months after HiFU. Patient underwent UAE, and 3-month follow-up MRI revealed complete infarction of leiomyoma (arrowheads). mo = month
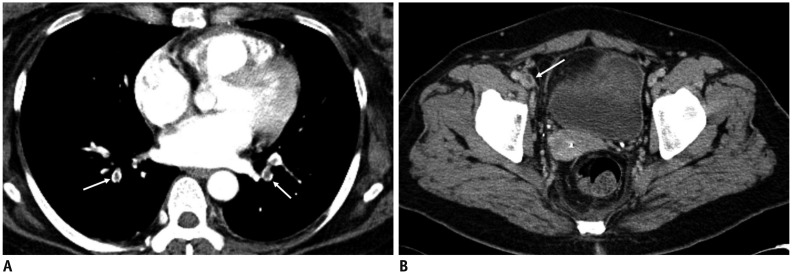
Fig. 6 Pulmonary embolism after UAE for adenomyosis.40-year-old woman with adenomyosis who was taking oral contraceptive pills for 3 weeks underwent UAE. Ten days after UAE, patient experienced dyspnea, and CT (A) revealed multiple pulmonary emboli (arrows) and thrombosis (arrow) of right common femoral vein (B). (Courtesy of Dr. Yeon Jaewoo at Bundang Jaeseng General Hospital).
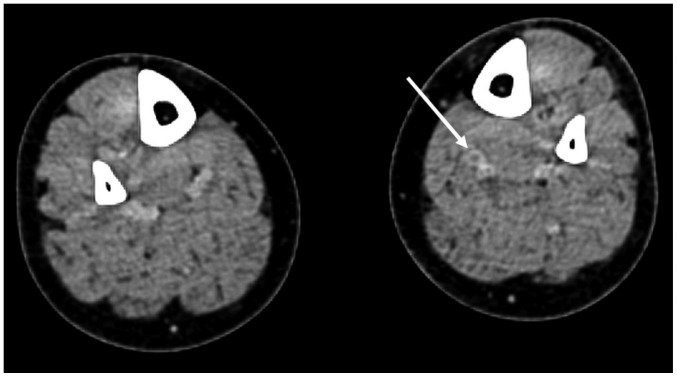
Fig. 7 Identification of DVT before UAE.50-year-old woman with adenomyosis and leiomyoma presented with uterine bleeding. She had been treated with oral contraceptives for 2 weeks. D-dimer level was 1143 ng/mL (normal range: 0–243 ng/mL), and CT scan of her lower extremities revealed venous thrombosis (arrow) in left lower leg. Renal cell carcinoma was detected incidentally (not shown). Partial nephrectomy was performed. One-month follow-up CT scan demonstrated complete occlusion of inferior vena cava filter and progression of thrombosis along both common iliac veins (not shown). DVT = deep vein thrombosis
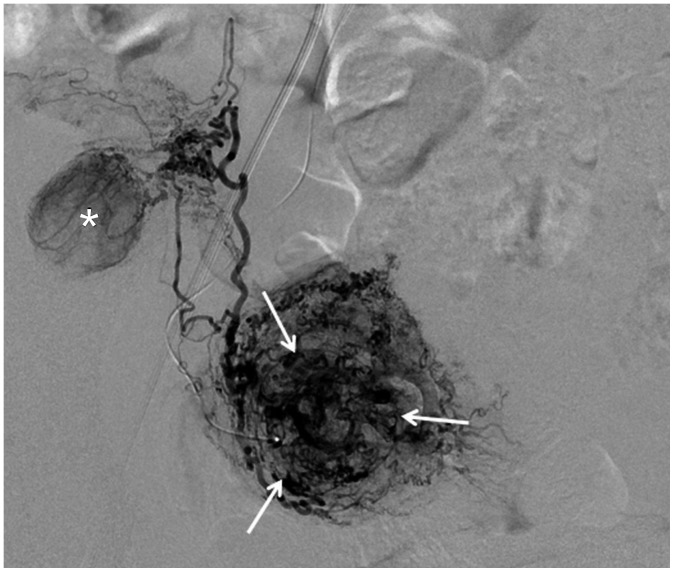
Fig. 8 Identification of leiomyoma in angiography.Uterine arteriography reveals leiomyoma (arrows). Right ovary (asterisk) is seen, representing example of Type III utero-ovarian anastomosis based on Razavi's classification.
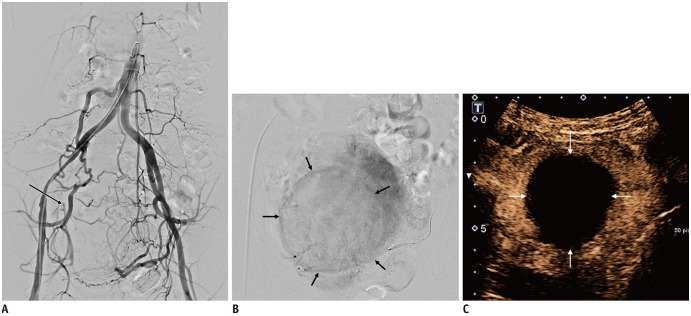
Fig. 9 Leiomyoma receiving blood flow from unilateral uterine artery.43-year-old woman underwent kidney transplantation 15 years prior. A. Abdominal aortography showed total occlusion of right internal iliac artery with reconstitution of right uterine artery (arrow) via collaterals. B. On selective uterine arteriography on left side, leiomyoma (arrows) received blood flow exclusively from left uterine artery. C. Complete devascularization of leiomyoma (arrows) is noted at 3-month follow-up contrast-enhanced ultrasound scan. Contrast-enhanced ultrasound instead of MRI was used due to end-stage renal disease.
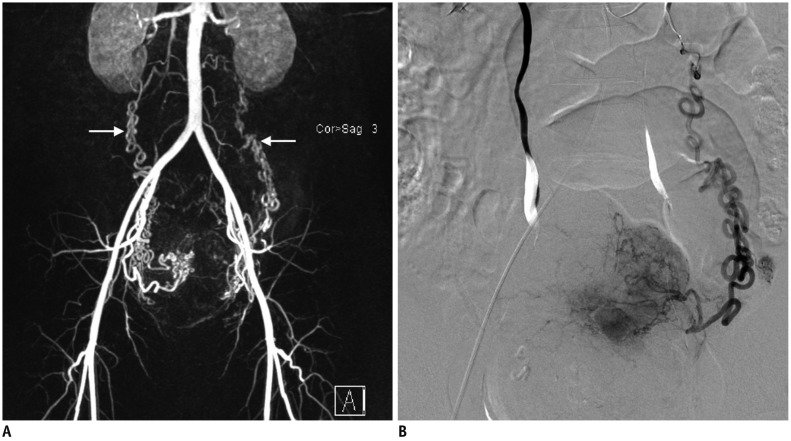
Fig. 10 Ovarian artery collateral to leiomyoma in uterine fundus.44-year-old woman presented with multiple leiomyomas. A. MR angiography revealed hypertrophy of both uterine and ovarian (arrows) arteries. B. Leiomyoma on uterine fundus was supplied by left ovarian artery (Type II anastomosis). MR = magnetic resonance
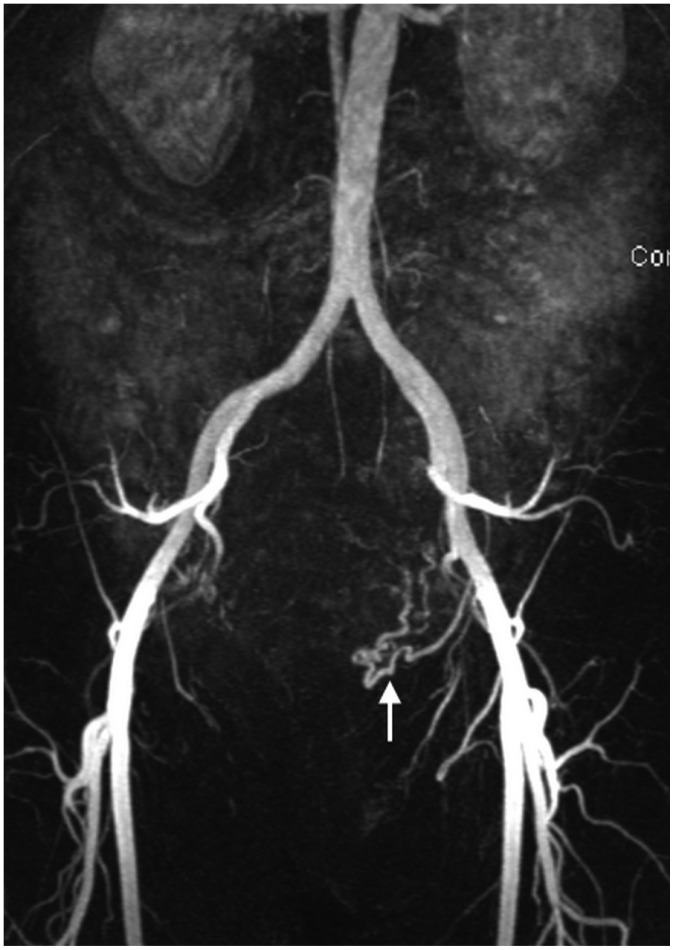
Fig. 11 Aplasia of right uterine artery.MR angiography revealed presence of only left uterine artery (arrow). Patient required right ovarian artery embolization.

Fig. 12 Leiomyoma becoming endocavitary after UAE.52-year-old woman had dysfunctional uterine bleeding. A. Sagittal T2WI revealed 7-cm pedunculated submucosal leiomyoma (arrows). B. One month after UAE, patient presented with cramping abdominal pain. Gadolinium-enhanced MRI revealed complete necrosis of submucosal leiomyoma (asterisk), which had become endocavitary, along with widening of cervix, suggesting ongoing expulsion. Three cervical dilatation and curettage procedures were needed to completely remove necrotic leiomyoma.
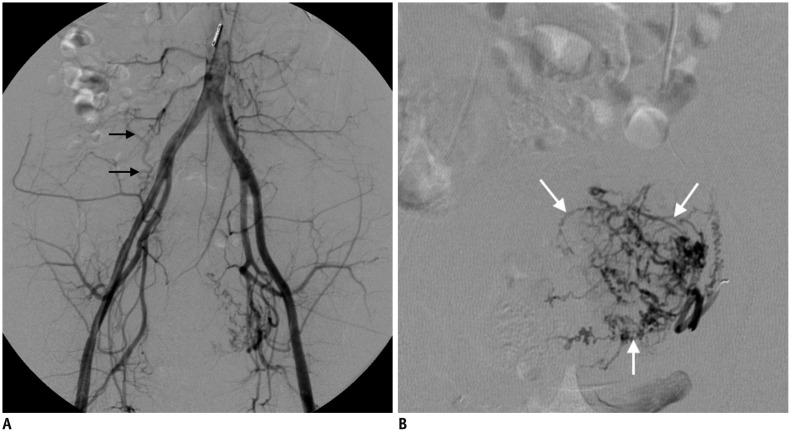
Fig. 13 Repeated UAE.43-year-old woman who had undergone UAE for leiomyomas 8 years prior presented with evidence of recurrent leiomyomas.A. Aortography revealed total occlusion of right uterine artery and hypertrophied right ovarian artery (arrows). B. Left uterine artery was partially recanalized, but multiple fine collaterals (arrows) supplied leiomyoma and uterus. Follow-up MRI performed after repeated UAE showed that procedure was ineffective (not shown).
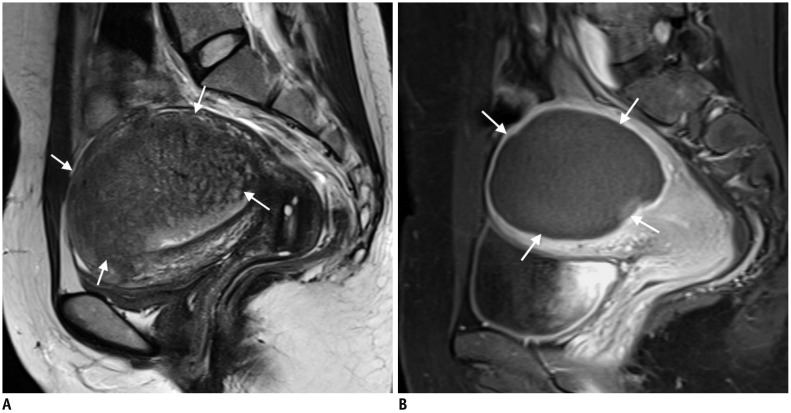
Fig. 14 38-year-old woman with adenomyosis presenting with vaginal bleeding and pain during menstruation.A. MRI revealed focal adenomyosis (arrows) with homogeneous, continuous, junctional zone thickening from endometrium. B. After embolization using small polyvinyl alcohol particles (1-2-3 protocol), complete necrosis of adenomyosis (arrows) was seen on 3-month follow-up MRI. Patient's status has been stable for 5 years.
Reference
-
1. Stewart EA. Clinical practice. Uterine fibroids. N Engl J Med. 2015; 372:1646–1655. PMID: 25901428.2. American College of Obstetricians and Gynecologists. ACOG practice bulletin. Alternatives to hysterectomy in the management of leiomyomas. Obstet Gynecol. 2008; 112(2 Pt 1):387–400. PMID: 18669742.3. Dariushnia SR, Nikolic B, Stokes LS, Spies JB. Society of Interventional Radiology Standards of Practice Committee. Quality improvement guidelines for uterine artery embolization for symptomatic leiomyomata. J Vasc Interv Radiol. 2014; 25:1737–1747. PMID: 25442136.
Article4. van Overhagen H, Reekers JA. Uterine artery embolization for symptomatic leiomyomata. Cardiovasc Intervent Radiol. 2015; 38:536–542. PMID: 25465064.
Article5. Kim YS, Han K, Kim MD, Kim GM, Kwon JH, Lee J, et al. Uterine artery embolization for pedunculated subserosal leiomyomas: evidence of safety and efficacy. J Vasc Interv Radiol. 2018; 29:497–501. PMID: 29477623.
Article6. Sinha R, Sundaram M, Lakhotia S, Hegde A. Cervical myomectomy with uterine artery ligation at its origin. J Minim Invasive Gynecol. 2009; 16:604–608. PMID: 19835802.
Article7. Takeuchi H, Kitade M, Kikuchi I, Shimanuki H, Kumakiri J, Kobayashi Y, et al. A new enucleation method for cervical myoma via laparoscopy. J Minim Invasive Gynecol. 2006; 13:334–336. PMID: 16825077.
Article8. Scheurig-Muenkler C, Wagner M, Franiel T, Hamm B, Kroencke TJ. Effect of uterine artery embolization on uterine and leiomyoma perfusion: evidence of transient myometrial ischemia on magnetic resonance imaging. J Vasc Interv Radiol. 2010; 21:1347–1353. PMID: 20685136.
Article9. Kim MD, Lee M, Jung DC, Park SI, Lee MS, Won JY, et al. Limited efficacy of uterine artery embolization for cervical leiomyomas. J Vasc Interv Radiol. 2012; 23:236–240. PMID: 22177843.
Article10. Murase E, Siegelman ES, Outwater EK, Perez-Jaffe LA, Tureck RW. Uterine leiomyomas: histopathologic features, MR imaging findings, differential diagnosis, and treatment. Radiographics. 1999; 19:1179–1197. PMID: 10489175.
Article11. Burn PR, McCall JM, Chinn RJ, Vashisht A, Smith JR, Healy JC. Uterine fibroleiomyoma: MR imaging appearances before and after embolization of uterine arteries. Radiology. 2000; 214:729–734. PMID: 10715038.
Article12. Chang S, Kim MD, Lee M, Lee MS, Park SI, Won JY, et al. Uterine artery embolization for symptomatic fibroids with high signal intensity on T2-weighted MR imaging. Korean J Radiol. 2012; 13:618–624. PMID: 22977330.
Article13. Funaki K, Fukunishi H, Funaki T, Kawakami C. Mid-term outcome of magnetic resonance-guided focused ultrasound surgery for uterine myomas: from six to twelve months after volume reduction. J Minim Invasive Gynecol. 2007; 14:616–621. PMID: 17848324.
Article14. Coffin P, Ascher S, Spies J. Risk of uterine malignancy in a population presenting for uterine artery embolization. J Vasc Interv Radiol. 2016; 27:S18.
Article15. Kainsbak J, Hansen ES, Dueholm M. Literature review of outcomes and prevalence and case report of leiomyosarcomas and non-typical uterine smooth muscle leiomyoma tumors treated with uterine artery embolization. Eur J Obstet Gynecol Reprod Biol. 2015; 191:130–137. PMID: 26117442.
Article16. Katsumori T, Nakajima K, Mihara T. Is a large fibroid a high-risk factor for uterine artery embolization? AJR Am J Roentgenol. 2003; 181:1309–1314. PMID: 14573425.
Article17. Worthington-Kirsch RL, Andrews RT, Siskin GP, Shlansky-Goldberg R, Lipman JC, Goodwin SC, et al. II. Uterine fibroid embolization: technical aspects. Tech Vasc Interv Radiol. 2002; 5:17–34. PMID: 12098105.
Article18. Kim MD, Lee M, Lee MS, Park SI, Wonq JY, Lee DY, et al. Uterine artery embolization of large fibroids: comparative study of procedure with and without pretreatment gonadotropin-releasing hormone agonists. AJR Am J Roentgenol. 2012; 199:441–446. PMID: 22826410.
Article19. Yang CH, Lee JN, Hsu SC, Kuo CH, Tsai EM. Effect of hormone replacement therapy on uterine fibroids in postmenopausal women--a 3-year study. Maturitas. 2002; 43:35–39. PMID: 12270580.
Article20. Lee SJ, Kim MD, Kim GM, Won JY, Park SI, Lee DY. Uterine artery embolization for symptomatic fibroids in postmenopausal women. Clin Imaging. 2016; 40:106–109. PMID: 26372352.
Article21. Nikolic B, Kessler CM, Jacobs HM, Abbara S, Ammann AM, Neeman Z, et al. Changes in blood coagulation markers associated with uterine artery embolization for leiomyomata. J Vasc Interv Radiol. 2003; 14(9 Pt 1):1147–1153. PMID: 14514806.
Article22. Hamoda H, Tait P, Edmonds DK. Fatal pulmonary embolus after uterine artery fibroid embolisation. Cardiovasc Intervent Radiol. 2009; 32:1080–1082. PMID: 19449063.
Article23. Lanocita R. A fatal complication of percutaneous transcatheter embolization for treatment of uterine fibroids. In : Second international symposium on embolization of uterine myomata; 1999 September 16–18; Boston, MA, USA.24. Chang S, Lee MS, Kim MD, Yoon CJ, Jung DC, Lee M, et al. Inferior mesenteric artery collaterals to the uterus during uterine artery embolization: prevalence, risk factors, and clinical outcomes. J Vasc Interv Radiol. 2013; 24:1353–1360. PMID: 23891048.
Article25. Lee MS, Kim MD, Lee M, Won JY, Park SI, Lee DY, et al. Contrast-enhanced MR angiography of uterine arteries for the prediction of ovarian artery embolization in 349 patients. J Vasc Interv Radiol. 2012; 23:1174–1179. PMID: 22920980.
Article26. Razavi MK, Wolanske KA, Hwang GL, Sze DY, Kee ST, Dake MD. Angiographic classification of ovarian artery-to-uterine artery anastomoses: initial observations in uterine fibroid embolization. Radiology. 2002; 224:707–712. PMID: 12202703.
Article27. Kim SY, Chang CH, Lee JS, Kim YJ, Kim MD, Han DW. Comparison of the efficacy of dexmedetomidine plus fentanyl patient-controlled analgesia with fentanyl patient-controlled analgesia for pain control in uterine artery embolization for symptomatic fibroid tumors or adenomyosis: a prospective, randomized study. J Vasc Interv Radiol. 2013; 24:779–786. PMID: 23707085.
Article28. Kim SY, Koo BN, Shin CS, Ban M, Han K, Kim MD. The effects of single-dose dexamethasone on inflammatory response and pain after uterine artery embolisation for symptomatic fibroids or adenomyosis: a randomised controlled study. BJOG. 2016; 123:580–587. PMID: 26667403.
Article29. Noel-Lamy M, Tan KT, Simons ME, Sniderman KW, Mironov O, Rajan DK. Intraarterial lidocaine for pain control in uterine artery embolization: a prospective, randomized study. J Vasc Interv Radiol. 2017; 28:16–22. PMID: 27884686.
Article30. Yoon J, Valenti D, Muchantef K, Cabrera T, Toonsi F, Torres C, et al. Superior hypogastric nerve block as post-uterine artery embolization analgesia: a randomized and double-blind clinical trial. Radiology. 2018; 289:248–254. PMID: 29989515.
Article31. Rasuli P, Jolly EE, Hammond I, French GJ, Preston R, Goulet S, et al. Superior hypogastric nerve block for pain control in outpatient uterine artery embolization. J Vasc Interv Radiol. 2004; 15:1423–1429. PMID: 15590800.
Article32. Pereira K, Salamo RM, Morel-Ovalle LM, Patel N, Patel R. Ropivacaine-induced local anesthetic systemic toxicity after superior hypogastric nerve block for pain control after uterine artery embolization. J Vasc Interv Radiol. 2018; 29:1315–1317. PMID: 30146211.
Article33. Park HR, Kim MD, Kim NK, Kim HJ, Yoon SW, Park WK, et al. Uterine restoration after repeated sloughing of fibroids or vaginal expulsion following uterine artery embolization. Eur Radiol. 2005; 15:1850–1854. PMID: 15729564.
Article34. van der Kooij SM, Hehenkamp WJ, Volkers NA, Birnie E, Ankum WM, Reekers JA. Uterine artery embolization vs hysterectomy in the treatment of symptomatic uterine fibroids: 5-year outcome from the randomized EMMY trial. Am J Obstet Gynecol. 2010; 203:105.e1–105.e13. PMID: 20579960.
Article35. Moss JG, Cooper KG, Khaund A, Murray LS, Murray GD, Wu O, et al. Randomised comparison of uterine artery embolisation (UAE) with surgical treatment in patients with symptomatic uterine fibroids (REST trial): 5-year results. BJOG. 2011; 118:936–944. PMID: 21481151.
Article36. Yoon JK, Han K, Kim MD, Kim GM, Kwon JH, Won JY, et al. Five-year clinical outcomes of uterine artery embolization for symptomatic leiomyomas: an analysis of risk factors for reintervention. Eur J Radiol. 2018; 109:83–87. PMID: 30527317.
Article37. Kim MD, Kim YM, Kim HC, Cho JH, Kang HG, Lee C, et al. Uterine artery embolization for symptomatic adenomyosis: a new technical development of the 1-2-3 protocol and predictive factors of MR imaging affecting outcomes. J Vasc Interv Radiol. 2011; 22:497–502. PMID: 21377897.
Article38. Jung DC, Kim MD, Oh YT, Won JY, Lee DY. Prediction of early response to uterine arterial embolisation of adenomyosis: value of T2 signal intensity ratio of adenomyosis. Eur Radiol. 2012; 22:2044–2049. PMID: 22527376.
Article39. Bae SH, Kim MD, Kim GM, Lee SJ, Park SI, Won JY, et al. Uterine artery embolization for adenomyosis: percentage of necrosis predicts midterm clinical recurrence. J Vasc Interv Radiol. 2015; 26:1290–1296.e2. PMID: 26074028.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Uterine Arterial Embolization for the Treatment of Uterine Leiomyomas
- Uterine Arterial Embolization for the Treatment of Leiomyomas Accompanying with Adenomyosis
- A Case of Vaginal Expulsion of Submucosal Fibroid after Uterine Artery Embolization
- Long-term MR Imaging after Uterine Artery Embolization for Symptomatic Adenomyosis
- Spontaneous Uterine Rupture after Uterine Artery Embolization for the Treatment of Uterine Myomas
