The Anomalous Left Brachiocephalic Vein in Adults
- Affiliations
-
- 1Department of Radiology, Sooncheonhyang University Cheonan Hospital, Cheonan, Korea. ytokim@schmc.ac.kr
- KMID: 2459019
- DOI: http://doi.org/10.3348/jksr.2019.80.5.942
Abstract
- PURPOSE
To classify anomalous left brachiocephalic vein (LBCV) in adult without cardiac anomaly, and evaluate CT findings of anomalous LBCV.
MATERIALS AND METHODS
This study included 32 patients who were diagnosed anomalous LBCV using MDCT between March 2005 and August 2016. Subaortic LBCV divided into group I (with normal LBCV) and group II (without normal LBCV). We evaluated age, sex, diameters and diameter ratios of superior vena cava (SVC) and subaortic LBCV, the entering sites to SVC of subaortic LBCV and the azygos vein, and vascular tortuosity of subaortic LBCV.
RESULTS
There were included 29 subaortic LBCV and 3 retroesophageal LBCV. There were not statistically significant in age, sex, diameter of SVC between subaortic groups (p > 0.05). The diameters of subaortic LBCV were thinner in group I. Diameter ratios of subaortic LBCV were lower in group I. The entering site of subaortic LBCV was higher than azygos vein in group I (64%) and same as azygos vein in group II (67%). Vascular tortuosity of subaortic LBCV was in 7 cases of group I.
CONCLUSION
It is important for radiologists to be familiar with CT findings of anomalous LBCV, since the radiologists give information of uncommon or rare anomalous LBCV to clinician.
Figure
-
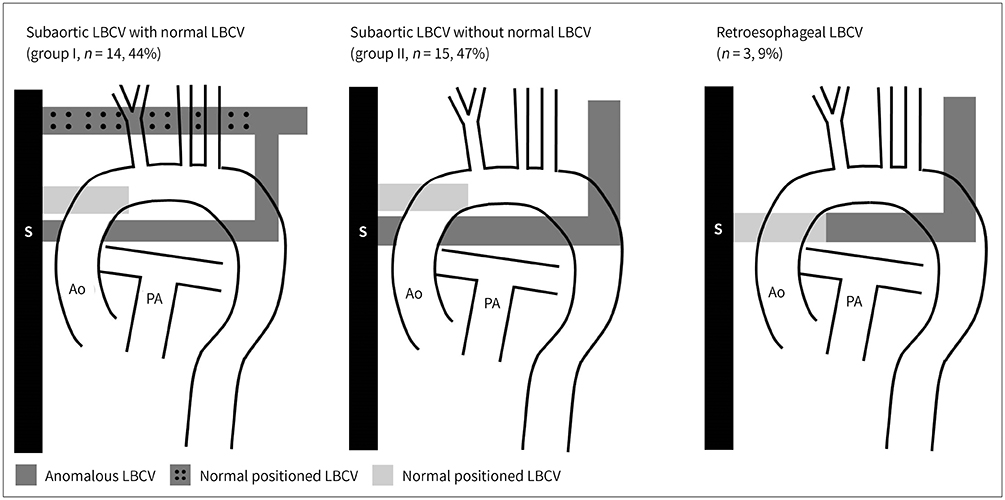
Fig. 1 Types of anomalous LBCVs. Anomalous LBCV includes subaortic and retroesophageal LBCVs. Subaortic LBCV is defined as an anomalous LBCV passing beneath the aortic arch and anterior to the trachea and esophagus regardless of the presence of a normal LBCV, because the normal venous structure entering the superior vena cava is not in the subaortic area. Therefore, a subaortic LBCV is classified into two types according to the presence of a normal LBCV. Retroesophageal LBCV is defined as an anomalous LBCV passing inferiorly along the aortic arch and running posterior to the trachea and esophagus without the presence of a normal LBCV, because the LBCV communicates with the azygos vein through the left superior intercostal vein and accessory hemiazygos vein in some individuals with a normal LBCV. Ao = aorta, LBCV = left brachiocephalic vein, PA = pulmonary artery, S = superior vena cava
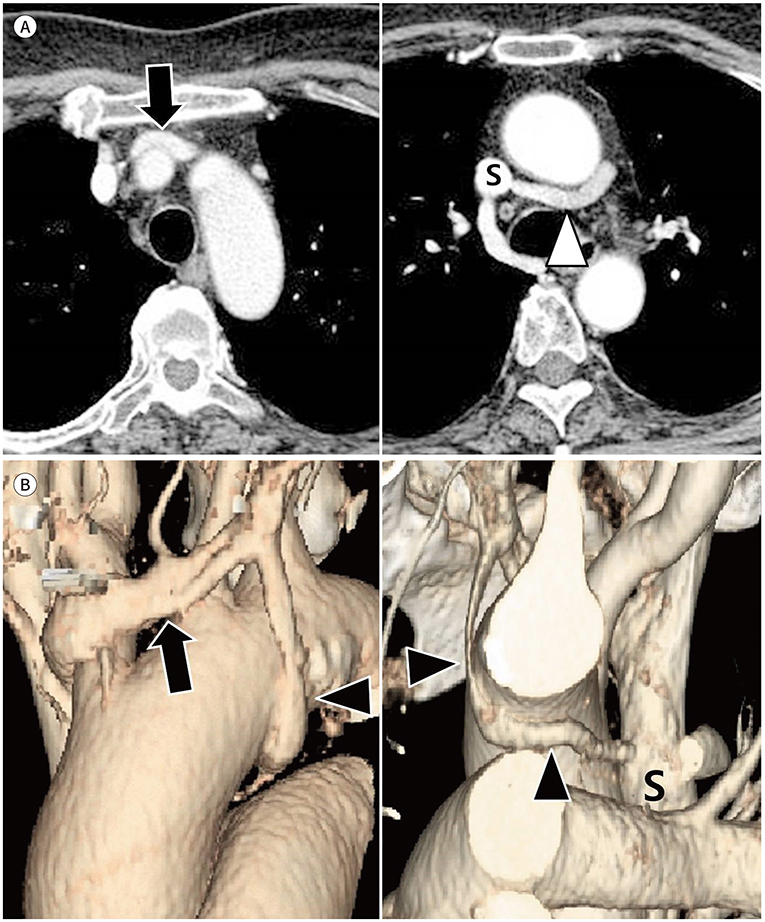
Fig. 2 Subaortic LBCV with a normal LBCV in a 64-year-old woman. A, B. Serial axial (A) and volume-rendering (B) images show a normally positioned LBCV (arrows) and a subaortic LBCV (arrowhead; A) draining to the superior vena cava. A small subaortic LBCV has a curvilinear course (arrowheads; B). The maximum diameter and diameter of the entering site of the subaortic LBCV are 6.07 mm and 5.82 mm respectively. The mean diameter of the superior vena cava is 15.95 mm. LBCV = left brachiocephalic vein, S = superior vena cava
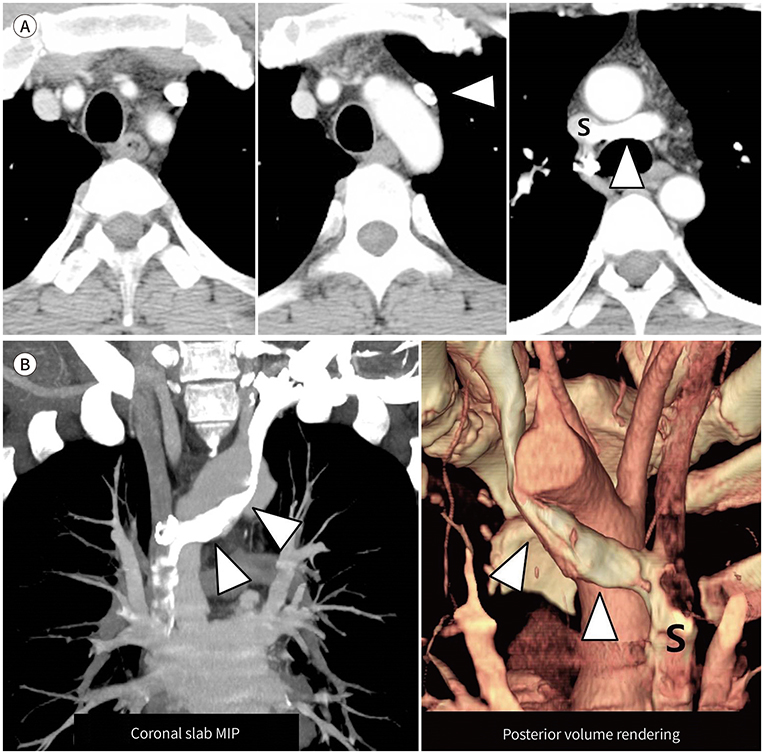
Fig. 3 Subaortic LBCV without a normal LBCV in a 43-year-old man. A. Serial axial images show a subaortic LBCV (arrowheads) running between the ascending thoracic aorta and trachea. A normally positioned LBCV is absent anterior to the aortic arch and thoracic great vessels. The maximum diameter and diameter of the entering site of the subaortic LBCV are 15.39 mm and 7.3 mm, respectively. The mean diameter of the superior vena cava is 17.99 mm. B. Coronal slab MIP and posterior volume-rendering images show that an subaortic LBCV (arrowheads) passes below the aortic arch and posterior to the ascending thoracic aorta, draining to the superior vena cava. LBCV = left brachiocephalic vein, MIP = maximum intensity projection, S = superior vena cava
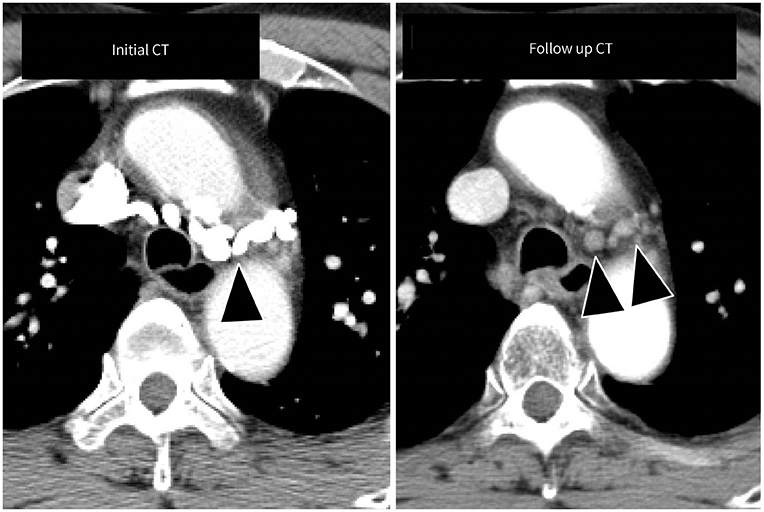
Fig. 4 Tortuous subaortic LBCV in a 74-year-old man. A tortuous subaortic LBCV is well visualized on the initial axial CT (arrowheads), but it cannot be seen on the follow up CT. This difference is caused by the injection site of the intravenous contrast media. When the initial CT was performed, intravenous contrast media was injected through the left arm. The follow up CT was performed after injection of intravenous contrast media through the right arm. On the follow up CT, the unenhanced subaortic LBCV mimics mediastinal lymph nodes. LBCV = left brachiocephalic vein
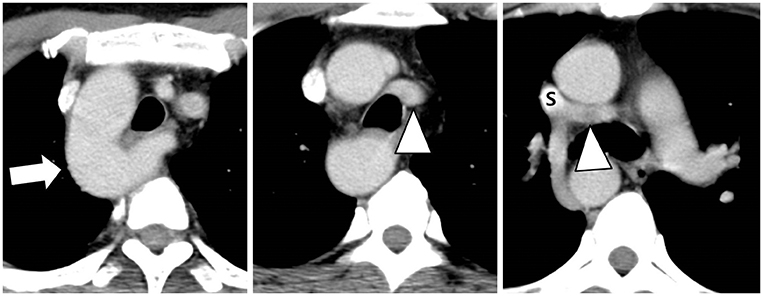
Fig. 5 Subaortic LBCV with the right aortic arch in a 42-year-old man. Serial axial images show a right-sided aortic arch (arrow) and a subaortic LBCV (arrowheads) draining to the superior vena cava. LBCV = left brachiocephalic vein, S = superior vena cava
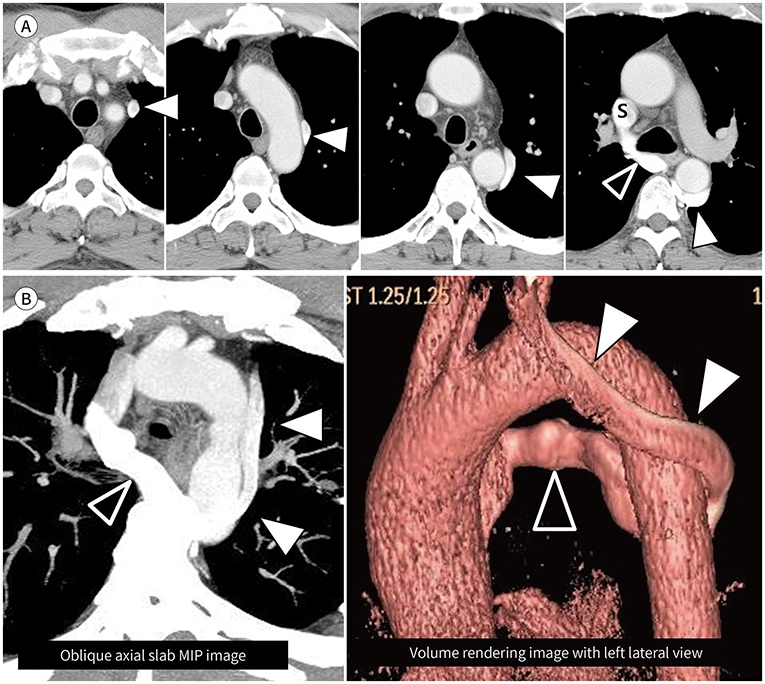
Fig. 6 Retroesophageal LBCV in a 57-year-old man. A. Serial axial images show a subaortic LBCV (arrowheads) running lateral to the aortic arch and posterior to the descending thoracic aorta and esophagus and draining to the superior vena cava through the azygos vein (open arrowhead). A normally positioned LBCV is absent. B. Oblique axial slab MIP and volume-rendering image with a left lateral view show a retroesophageal LBCV (arrowheads) looping around the aortic arch and descending thoracic aorta and joining the azygos vein (open arrowheads). LBCV = left brachiocephalic vein, MIP = maximum intensity projection, S = superior vena cava
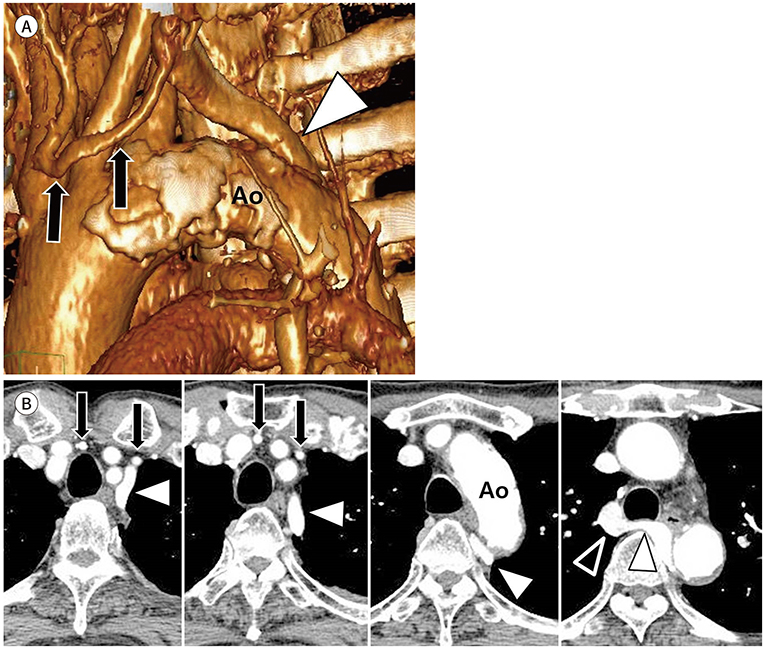
Fig. 7 Retroesophageal LBCV in a 78-year-old man. A. Volume-rendering image with a left lateral view shows the retroesophageal LBCV (arrowhead) running medial to the Ao. Note the thyroidal veins (arrows) between the thoracic great vessels. B. On serial axial images, an anomalous LBCV (arrowheads) passes medial to the Ao and turns posterior to the esophagus, joining the azygos vein (open arrowhead) before draining to the superior vena cava. A normally positioned LBCV is absent. Note the thyroidal veins (arrows) between the thoracic great vessels. Ao = aortic arch, LBCV = left brachiocephalic vein, S = superior vena cava
Reference
-
1. Kershner L. Morphologie der vena cava inferior. Anat Anz. 1888; 3:808–823.2. Curtil A, Tronc F, Champsaur G, Bozio A, Sassolas F, Carret JP, et al. The left retro-aortic brachiocephalic vein: morphologic data and diagnostic ultrasound in 27 cases. Surg Radiol Anat. 1999; 21:251–254.
Article3. Sinkovskaya E, Abuhamad A, Horton S, Chaoui R, Karl K. Fetal left brachiocephalic vein in normal and abnormal conditions. Ultrasound Obstet Gynecol. 2012; 40:542–548.
Article4. Chen SJ, Liu KL, Chen HY, Chiu IS, Lee WJ, Wu MH, et al. Anomalous brachiocephalic vein: CT, embryology, and clinical implications. AJR Am J Roentgenol. 2005; 184:1235–1240.
Article5. Takada Y, Narimatsu A, Kohno A, Kawai C, Hara H, Harasawa A, et al. Anomalous left brachiocephalic vein: CT findings. J Comput Assist Tomogr. 1992; 16:893–896.6. Chern MS, Ko JS, Tsai A, Wu MH, Teng MM, Chang CY. Aberrant left brachiocephalic vein: CT imaging findings and embryologic correlation. Eur Radiol. 1999; 9:1835–1839.
Article7. Ming Z, Aimin S, Rui H. Evaluation of the anomalous retroesophageal left brachiocephalic vein in Chinese children using multidetector CT. Pediatr Radiol. 2009; 39:343–347.
Article8. Yigit AE, Haliloglu M, Karcaaltincaba M, Ariyurek MO. Retrotracheal aberrant left brachiocephalic vein: CT findings. Pediatr Radiol. 2008; 38:322–324.
Article9. Gerlis LM, Ho SY. Anomalous subaortic position of the brachiocephalic (innominate) vein: a review of published reports and report of three new cases. Br Heart J. 1989; 61:540–545.
Article10. Choi JY, Jung MJ, Kim YH, Noh CI, Yun YS. Anomalous subaortic position of the brachiocephalic vein (innominate vein): an echocardiographic study. Br Heart J. 1990; 64:385–387.
Article11. Mill MR, Wilcox BR, Detterbeck FC, Anderson RH. Anomalous course of the left brachiocephalic vein. Ann Thorac Surg. 1993; 55:600–602.
Article12. Adachi B. Anatomie der Japaner: II, das Venensystem der Japaner. Kyoto: Kyoto University Press;1933. p. 83–87.13. Smallhorn JF, Zielinsky P, Freedom RM, Rowe RD. Abnormal position of the brachiocephalic vein. Am J Cardiol. 1985; 55:234–236.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Double Left Brachiocephalic Veins with Persistent Left Superior Vena Cava: A Case Report
- Circumaortic Left Brachiocephalic Vein: CT Findings
- An Unusual Cause of Left Brachiocephalic Vein Occlusion: Extrinsic Compression by the Aortic Arch in a Hemodialysis Patient
- Anomalous Pulmonary Venous Return Accompanied by Normal Superior Pulmonary Veins in the Left Upper Lobe: A Case Report
- Subaortic Left Brachiocephalic Vein
