Emerging Techniques in Brain Tumor Imaging: What Radiologists Need to Know
- Affiliations
-
- 1Department of Radiology and Research Institute of Radiology, University of Ulsan College of Medicine, Asan Medical Center, Seoul 05505, Korea. radhskim@gmail.com
- KMID: 2458052
- DOI: http://doi.org/10.3348/kjr.2016.17.5.598
Abstract
- Among the currently available brain tumor imaging, advanced MR imaging techniques, such as diffusion-weighted MR imaging and perfusion MR imaging, have been used for solving diagnostic challenges associated with conventional imaging and for monitoring the brain tumor treatment response. Further development of advanced MR imaging techniques and postprocessing methods may contribute to predicting the treatment response to a specific therapeutic regimen, particularly using multi-modality and multiparametric imaging. Over the next few years, new imaging techniques, such as amide proton transfer imaging, will be studied regarding their potential use in quantitative brain tumor imaging. In this review, the pathophysiologic considerations and clinical validations of these promising techniques are discussed in the context of brain tumor characterization and treatment response.
MeSH Terms
Figure
-

Fig. 1 Illustration of diffusion characteristics and their image processing Fast diffusion within extracellular and extravascular space is calculated by monoexponential fitting of diffusion signals with b values of 0 and 1000 s/mm2. Very rapid diffusion due to capillary perfusion can be characterized by biexponential fitting of diffusion signals as function of multiple b values, especially those less than 200 s/mm2. Intracellular slow diffusion can be determined by biexponential fitting of diffusion signals with multiple high b values. IVIM = intravoxel incoherent motion

Fig. 2 DWI with low and high b values of presumed lymphoma in 38-year-old male A. Contrast-enhanced, axial, T1-weighted MR image shows contrast-enhancing mass in brain stem. B. DWI with b value of 1000 s/mm2 shows equivocal high-signal intensity in same lesion. C. DWI with b value of 3000 s/mm2 enhances DWI signal, high signal intensity in corresponding lesion. D. ADC is correspondingly low as DWI with higher b values increases effect on signal of obstacles to free diffusion present in tissue. ADC = apparent diffusion coefficient, DWI = diffusion-weighted MR imaging

Fig. 3 Different DWI signals within tumor necrosis of two glioblastomas A. Necrotic tumor component of glioblastoma usually shows low DWI signal (arrow) due to migration and apoptosis of hypoxic tumor cells. B. Tumor necrosis could also show high DWI signal (arrow) due to tumor coagulation necrosis or ischemia associated with vascular occlusion by tumor cells. DWI = diffusion-weighted MR imaging
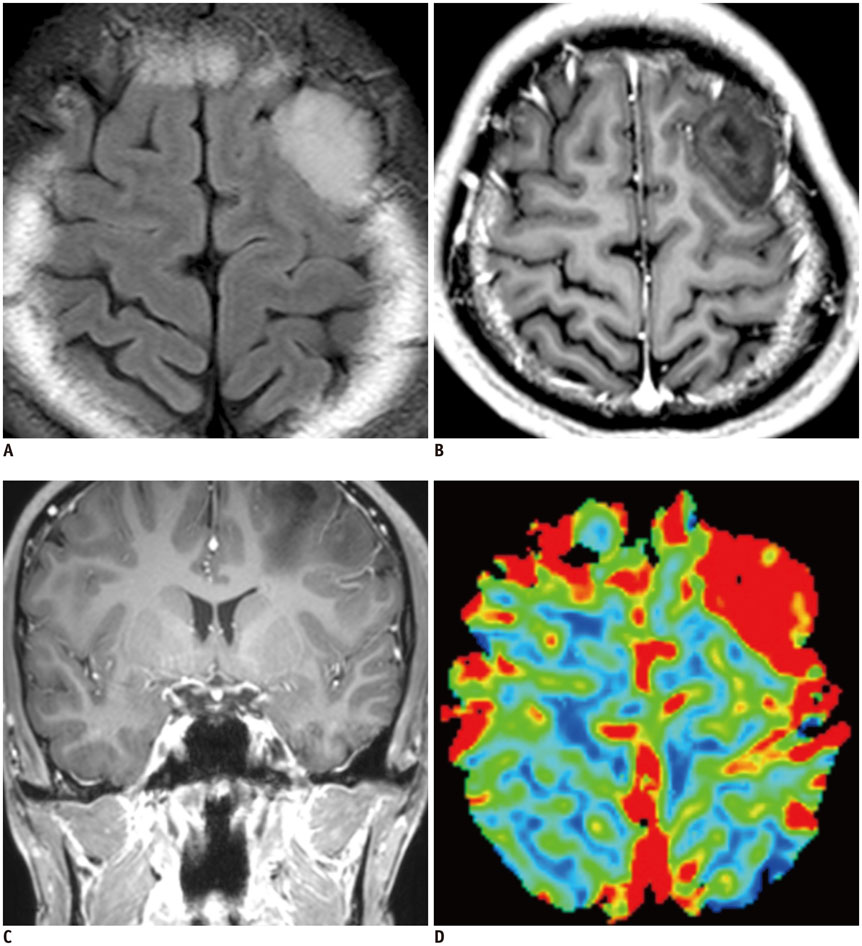
Fig. 4 Increased rCBV of anaplastic astrocytoma in 23-year-old male A. Intra-axial mass with high signal intensity seen on FLAIR, is noted in left frontal lobe. B, C. Mass dose not enhance on contrast-enhanced axial (B) and coronal (C), T1-weighted MR images. D. rCBV map derived from DSC perfusion MR imaging shows markedly increased rCBV in corresponding lesion, and thus reflecting larger luminal area of tumor microvessels. DSC = dynamic susceptibility contrast, FLAIR = fluid attenuated inversion recovery, rCBV = relative cerebral blood volume
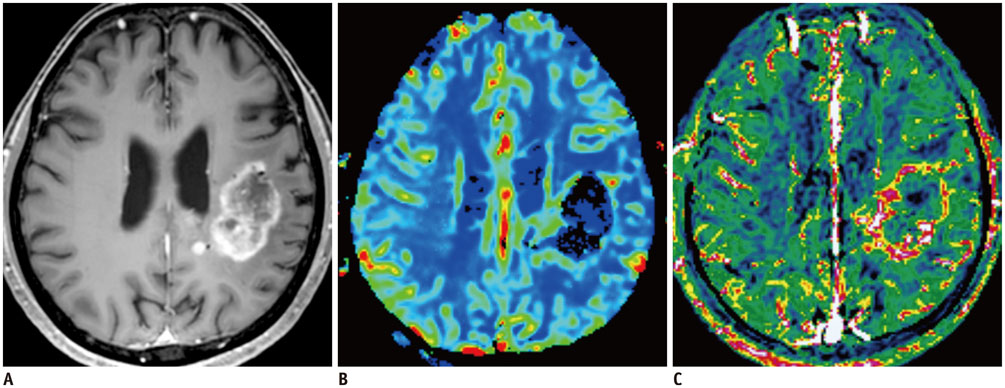
Fig. 5 Images obtained in 63-year-old female clinicoradiologically considered as having recurrent glioblastoma A. Contrast-enhanced, T1-weighted image acquired 17 months after concomitant chemoradiotherapy, shows necrotic, enhancing mass in left parietal lobe. B. DSC perfusion MR image shows equivocal increase of rCBV in corresponding lesion. C. Corresponding, contrast-enhanced, solid portion shows definite increase of permeability on DCE perfusion MR imaging, and thus suggesting tumor recurrence. DCE = dynamic contrast-enhanced, DSC = dynamic susceptibility contrast, rCBV = relative cerebral blood volume
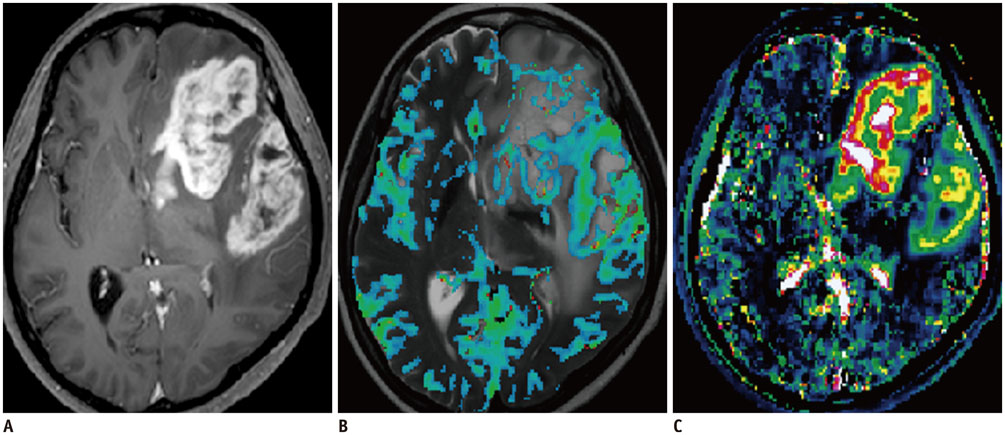
Fig. 6 Comparison of DSC and DCE perfusion MR images in 67-year-old female with glioblastoma A. Contrast-enhanced, axial, T1-weighted MR image shows necrotic, contrast-enhancing mass in left frontal and temporal lobes. B. DSC perfusion MR imaging shows heterogeneously increased rCBV in corresponding lesion. C. DCE perfusion MR imaging shows higher signal-to-noise ratio and spatial resolution of permeability distribution within same lesion, compared with that seen on DSC perfusion MR imaging. DCE = dynamic contrast-enhanced, DSC = dynamic susceptibility contrast, rCBV = relative cerebral blood volume

Fig. 7 Illustration of association between tumor vessel pattern and cerebral blood volume A. Immature, hyperpermeable, and tortuous tumor vessel pattern causes ineffective and heterogeneous tumor blood flow (arrow) which thus impedes delivery of chemotherapeutic drug to tumor. B. Increased homogeneity of tumor-vessel density and more well ordered arrangement of vessels increase tumor blood flow (arrow) and reduce its heterogeneity, and which improve drug delivery and efficacy. CBF = cerebral blood flow, DCE = dynamic contrast-enhanced

Fig. 8 Images obtained in 76-year-old male with glioblastoma A. T2-weighted MR image shows intra-axial mass with surrounding edema in right parietal lobe. B. DWI shows high signal intensity in corresponding lesion, and thus suggesting high tumor cellularity. C. Contrast-enhanced, axial, T1-weighted MR image shows necrotic, contrast-enhancing mass in same lesion. D. Contrast-enhanced SWI shows additional information regarding microhemorrhage and tumor microvessels around tumor necrosis seen on contrast-enhanced, T1-weighted image. DWI = diffusion-weighted MR imaging, SWI = susceptibility-weighted imaging

Fig. 9 Images obtained in 47-year-old male with anaplastic oligodendroglioma A, B. T2-weighted MR image (A) and contrast enhanced, T1-weighted image (B) show intra-axial lesion with internal hemorrhage in left frontal lobe. C. Pre-contrast SWI demonstrates rim of low signal intensity in corresponding lesion. D. Contrast-enhanced SWI shows additional linear or dot-like structures of low signal intensity (arrows), suggesting tumor microvessels as well as unchanged lesion of low signal intensity (arrowhead), and suggesting microhemorrhage. SWI = susceptibility-weighted imaging

Fig. 10 Illustration of amide proton transfer mechanism Amide protons are saturated at their specific resonance frequency with selective radiofrequency pulse. Saturated proton is then transferred to surrounding free water and consequently water signal decrease is calculated for indirect estimation of amount of amide proton.

Fig. 11 Images obtained in 55-year-old male with glioblastoma A. Contrast-enhanced, axial, T1-weighted MR image shows contrast-enhancing lesion around fourth ventricle. B-E. All of advanced MR images including DWI (B), DSC perfusion MR image (C), DCE perfusion MR image (D), and amide proton transfer image (E) show increased parametric values, although different distribution within corresponding contrast-enhancing lesion. DCE = dynamic contrast-enhanced, DSC = dynamic susceptibility contrast, DWI = diffusion-weighted MR imaging
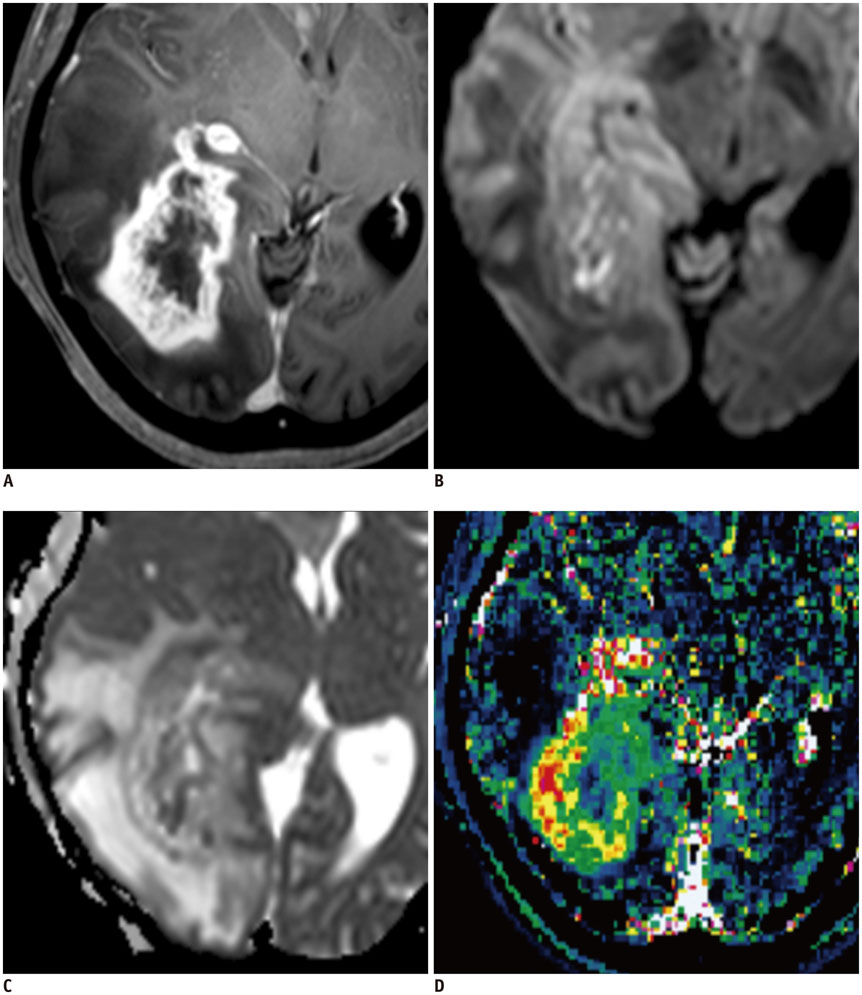
Fig. 12 Images obtained in 57-year-old female with recurrent glioblastoma A. Contrast-enhanced, T1-weighted image acquired five months after concomitant chemoradiotherapy shows necrotic, enhancing mass in right temporo-occipital lobe. B, C. DWI (B) and ADC (C) show linear area of diffusion restriction surrounding tumor necrosis, possibly indicating viable, compact tumor cells. D. DCE perfusion MR image shows increase of permeability in corresponding, contrast-enhancing lesion around area of diffusion restriction, and reflecting immature tumor vessel. ADC = apparent diffusion coefficient, DCE = dynamic contrast-enhanced, DWI = diffusion-weighted MR imaging
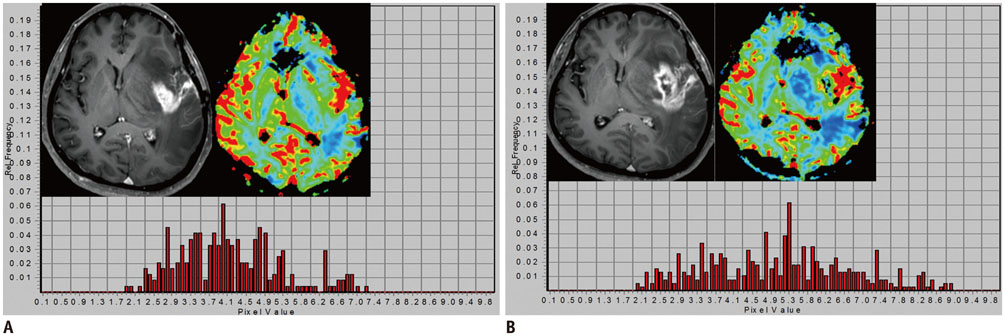
Fig. 13 Images obtained in 55-year-old female with recurrent glioblastoma A. At seven weeks after concomitant chemoradiotherapy, histogram from normalized rCBV for entire, corresponding, contrast-enhancing lesion reveals heterogeneous distribution of normalized rCBV values. B. At 15 weeks after concomitant chemoradiotherapy, histogram showed more heterogeneous distribution of normalized rCBV values compared with those seen in previous study, and thus suggesting tumor progression. rCBV = relative cerebral blood volume
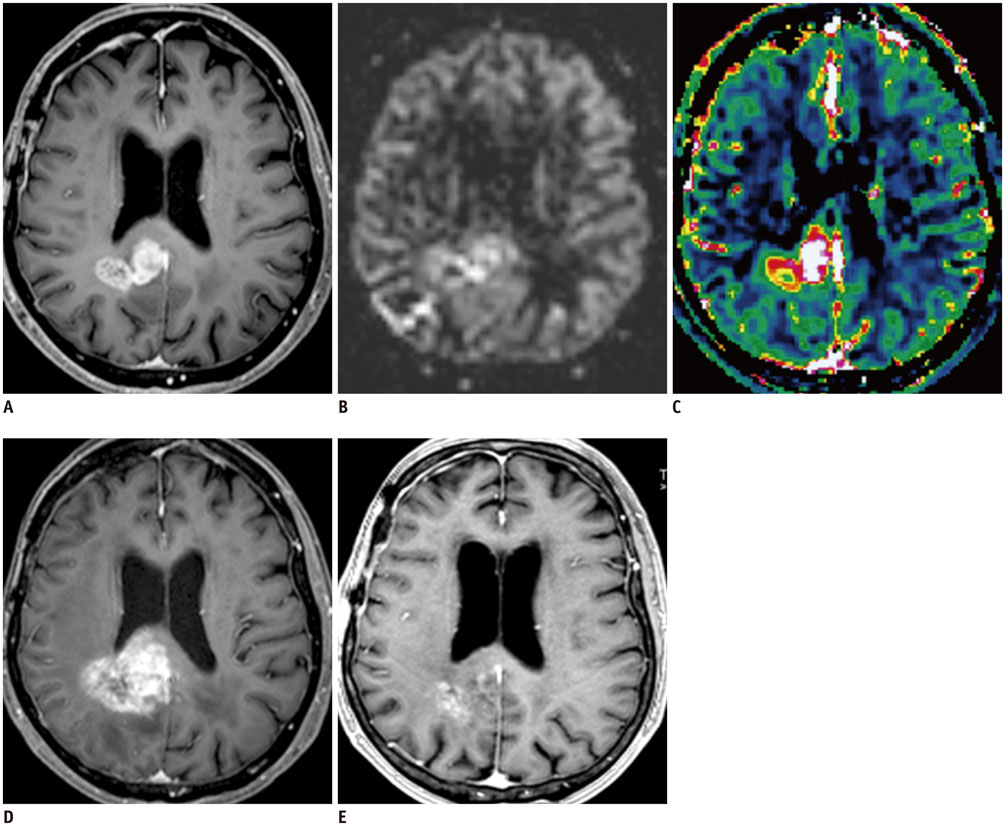
Fig. 14 Images obtained in 75-year-old female with pseudoprogression A. Contrast-enhanced, T1-weighted image acquired five weeks after concomitant chemoradiotherapy shows enhancing mass in right parieto-occipital lobe. B, C. ASL (B) and DCE perfusion MR imaging (C) show increased CBF and permeability in corresponding contrast-enhanced lesion, respectively, and thus indicating effective drug delivery. D. After two cycles of adjuvant temozolomide, extent of enhancing lesion increased. E. After four cycles of adjuvant temozolomide, enlarged, enhancing lesion was stabilized, and thus suggesting pseudoprogression. ASL = arterial spin labeling, CBF = cerebral blood flow, DCE = dynamic contrast-enhanced
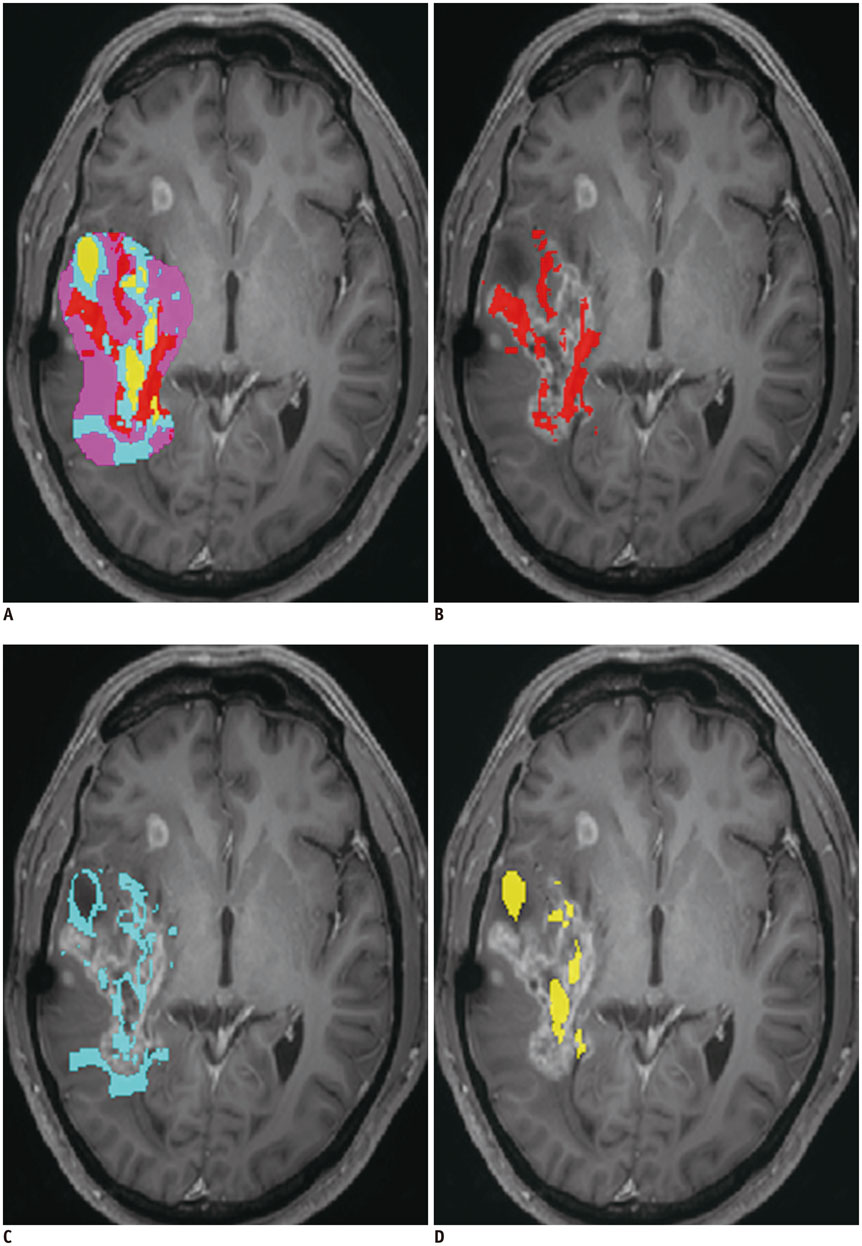
Fig. 15 Tumor clustering in 59-year-old female with recurrent glioblastoma A. Contrast-enhancing mass is segmented and clustered with combination of ADC, rCBV, and permeability parameters on voxel-by-voxel basis. B. Volume fraction of presumed tumor cluster is highest (45%), compared with other clusters (C, D), and thus suggesting tumor recurrence. ADC = apparent diffusion coefficient, rCBV = relative cerebral blood volume
Cited by 5 articles
-
Quality of Radiomic Features in Glioblastoma Multiforme: Impact of Semi-Automated Tumor Segmentation Software
Myungeun Lee, Boyeong Woo, Michael D. Kuo, Neema Jamshidi, Jong Hyo Kim
Korean J Radiol. 2017;18(3):498-509. doi: 10.3348/kjr.2017.18.3.498.Efficacy of Maximum Intensity Projection of Contrast-Enhanced 3D Turbo-Spin Echo Imaging with Improved Motion-Sensitized Driven-Equilibrium Preparation in the Detection of Brain Metastases
Yun Jung Bae, Byung Se Choi, Kyung Mi Lee, Yeon Hong Yoon, Leonard Sunwoo, Cheolkyu Jung, Jae Hyoung Kim
Korean J Radiol. 2017;18(4):699-709. doi: 10.3348/kjr.2017.18.4.699.Splenial Lesions of the Corpus Callosum: Disease Spectrum and MRI Findings
Sung Eun Park, Dae Seob Choi, Hwa Seon Shin, Hye Jin Baek, Ho Cheol Choi, Ji Eun Kim, Hye Young Choi, Mi Jung Park
Korean J Radiol. 2017;18(4):710-721. doi: 10.3348/kjr.2017.18.4.710.Optimal Factors of Diffusion Tensor Imaging Predicting Corticospinal Tract Injury in Patients with Brain Tumors
Zhi-gang Min, Chen Niu, Qiu-li Zhang, Ming Zhang, Yu-cheng Qian
Korean J Radiol. 2017;18(5):844-851. doi: 10.3348/kjr.2017.18.5.844.Age of Data in Contemporary Research Articles Published in Representative General Radiology Journals
Ji Hun Kang, Dong Hwan Kim, Seong Ho Park, Jung Hwan Baek
Korean J Radiol. 2018;19(6):1172-1178. doi: 10.3348/kjr.2018.19.6.1172.
Reference
-
1. Jahng GH, Li KL, Ostergaard L, Calamante F. Perfusion magnetic resonance imaging: a comprehensive update on principles and techniques. Korean J Radiol. 2014; 15:554–577.2. Park SH, Han PK, Choi SH. Physiological and functional magnetic resonance imaging using balanced steady-state free precession. Korean J Radiol. 2015; 16:550–559.3. Iima M, Le Bihan D. Clinical intravoxel incoherent motion and diffusion MR imaging: past, present, and future. Radiology. 2016; 278:13–32.4. Jensen JH, Helpern JA, Ramani A, Lu H, Kaczynski K. Diffusional kurtosis imaging: the quantification of non-gaussian water diffusion by means of magnetic resonance imaging. Magn Reson Med. 2005; 53:1432–1440.5. Hu LS, Eschbacher JM, Dueck AC, Heiserman JE, Liu S, Karis JP, et al. Correlations between perfusion MR imaging cerebral blood volume, microvessel quantification, and clinical outcome using stereotactic analysis in recurrent high-grade glioma. AJNR Am J Neuroradiol. 2012; 33:69–76.6. Gilad AA, Israely T, Dafni H, Meir G, Cohen B, Neeman M. Functional and molecular mapping of uncoupling between vascular permeability and loss of vascular maturation in ovarian carcinoma xenografts: the role of stroma cells in tumor angiogenesis. Int J Cancer. 2005; 117:202–211.7. Ellingson BM, Malkin MG, Rand SD, Connelly JM, Quinsey C, LaViolette PS, et al. Validation of functional diffusion maps (fDMs) as a biomarker for human glioma cellularity. J Magn Reson Imaging. 2010; 31:538–548.8. Sugahara T, Korogi Y, Kochi M, Ikushima I, Shigematu Y, Hirai T, et al. Usefulness of diffusion-weighted MRI with echo-planar technique in the evaluation of cellularity in gliomas. J Magn Reson Imaging. 1999; 9:53–60.9. Filli L, Wurnig M, Nanz D, Luechinger R, Kenkel D, Boss A. Whole-body diffusion kurtosis imaging: initial experience on non-Gaussian diffusion in various organs. Invest Radiol. 2014; 49:773–778.10. LaViolette PS, Mickevicius NJ, Cochran EJ, Rand SD, Connelly J, Bovi JA, et al. Precise ex vivo histological validation of heightened cellularity and diffusion-restricted necrosis in regions of dark apparent diffusion coefficient in 7 cases of high-grade glioma. Neuro Oncol. 2014; 16:1599–1606.11. Choi H, Paeng JC, Cheon GJ, Park CK, Choi SH, Min HS, et al. Correlation of 11C-methionine PET and diffusion-weighted MRI: is there a complementary diagnostic role for gliomas? Nucl Med Commun. 2014; 35:720–726.12. Rose S, Fay M, Thomas P, Bourgeat P, Dowson N, Salvado O, et al. Correlation of MRI-derived apparent diffusion coefficients in newly diagnosed gliomas with [18F]-fluoro-L-dopa PET: what are we really measuring with minimum ADC? AJNR Am J Neuroradiol. 2013; 34:758–764.13. Hayashida Y, Hirai T, Morishita S, Kitajima M, Murakami R, Korogi Y, et al. Diffusion-weighted imaging of metastatic brain tumors: comparison with histologic type and tumor cellularity. AJNR Am J Neuroradiol. 2006; 27:1419–1425.14. Shim WH, Kim HS, Choi CG, Kim SJ. Comparison of apparent diffusion coefficient and intravoxel incoherent motion for differentiating among glioblastoma, metastasis, and lymphoma focusing on diffusion-related parameter. PLoS One. 2015; 10:e0134761.15. Federau C, Maeder P, O'Brien K, Browaeys P, Meuli R, Hagmann P. Quantitative measurement of brain perfusion with intravoxel incoherent motion MR imaging. Radiology. 2012; 265:874–881.16. Notohamiprodjo M, Chandarana H, Mikheev A, Rusinek H, Grinstead J, Feiweier T, et al. Combined intravoxel incoherent motion and diffusion tensor imaging of renal diffusion and flow anisotropy. Magn Reson Med. 2015; 73:1526–1532.17. Raab P, Hattingen E, Franz K, Zanella FE, Lanfermann H. Cerebral gliomas: diffusional kurtosis imaging analysis of microstructural differences. Radiology. 2010; 254:876–881.18. Dean BL, Drayer BP, Bird CR, Flom RA, Hodak JA, Coons SW, et al. Gliomas: classification with MR imaging. Radiology. 1990; 174:411–415.19. Falangola MF, Jensen JH, Babb JS, Hu C, Castellanos FX, Di Martino A, et al. Age-related non-Gaussian diffusion patterns in the prefrontal brain. J Magn Reson Imaging. 2008; 28:1345–1350.20. Kim SJ, Choi CG, Kim JK, Yun SC, Jahng GH, Jeong HK, et al. Effects of MR parameter changes on the quantification of diffusion anisotropy and apparent diffusion coefficient in diffusion tensor imaging: evaluation using a diffusional anisotropic phantom. Korean J Radiol. 2015; 16:297–303.21. Daumas-Duport C, Scheithauer B, O'Fallon J, Kelly P. Grading of astrocytomas. A simple and reproducible method. Cancer. 1988; 62:2152–2165.22. Maier SE, Sun Y, Mulkern RV. Diffusion imaging of brain tumors. NMR Biomed. 2010; 23:849–864.23. Iima M, Yano K, Kataoka M, Umehana M, Murata K, Kanao S, et al. Quantitative non-Gaussian diffusion and intravoxel incoherent motion magnetic resonance imaging: differentiation of malignant and benign breast lesions. Invest Radiol. 2015; 50:205–211.24. Birner P, Piribauer M, Fischer I, Gatterbauer B, Marosi C, Ambros PF, et al. Vascular patterns in glioblastoma influence clinical outcome and associate with variable expression of angiogenic proteins: evidence for distinct angiogenic subtypes. Brain Pathol. 2003; 13:133–143.25. Korkolopoulou P, Patsouris E, Kavantzas N, Konstantinidou AE, Christodoulou P, Thomas-Tsagli E, et al. Prognostic implications of microvessel morphometry in diffuse astrocytic neoplasms. Neuropathol Appl Neurobiol. 2002; 28:57–66.26. Wesseling P, van der Laak JA, Link M, Teepen HL, Ruiter DJ. Quantitative analysis of microvascular changes in diffuse astrocytic neoplasms with increasing grade of malignancy. Hum Pathol. 1998; 29:352–358.27. Wesseling P, van der Laak JA, de Leeuw H, Ruiter DJ, Burger PC. Quantitative immunohistological analysis of the microvasculature in untreated human glioblastoma multiforme. Computer-assisted image analysis of whole-tumor sections. J Neurosurg. 1994; 81:902–909.28. Barajas RF Jr, Phillips JJ, Parvataneni R, Molinaro A, Essock-Burns E, Bourne G, et al. Regional variation in histopathologic features of tumor specimens from treatment-naive glioblastoma correlates with anatomic and physiologic MR Imaging. Neuro Oncol. 2012; 14:942–954.29. Hyodo F, Chandramouli GV, Matsumoto S, Matsumoto K, Mitchell JB, Krishna MC, et al. Estimation of tumor microvessel density by MRI using a blood pool contrast agent. Int J Oncol. 2009; 35:797–804.30. Wilmes LJ, Pallavicini MG, Fleming LM, Gibbs J, Wang D, Li KL, et al. AG-013736, a novel inhibitor of VEGF receptor tyrosine kinases, inhibits breast cancer growth and decreases vascular permeability as detected by dynamic contrast-enhanced magnetic resonance imaging. Magn Reson Imaging. 2007; 25:319–327.31. Boxerman JL, Schmainda KM, Weisskoff RM. Relative cerebral blood volume maps corrected for contrast agent extravasation significantly correlate with glioma tumor grade, whereas uncorrected maps do not. AJNR Am J Neuroradiol. 2006; 27:859–867.32. Donahue KM, Krouwer HG, Rand SD, Pathak AP, Marszalkowski CS, Censky SC, et al. Utility of simultaneously acquired gradient-echo and spin-echo cerebral blood volume and morphology maps in brain tumor patients. Magn Reson Med. 2000; 43:845–853.33. Choi HS, Ahn SS, Shin NY, Kim J, Kim JH, Lee JE, et al. Permeability parameters measured with dynamic contrast-enhanced MRI: correlation with the extravasation of evans blue in a rat model of transient cerebral ischemia. Korean J Radiol. 2015; 16:791–797.34. Tofts PS. Modeling tracer kinetics in dynamic Gd-DTPA MR imaging. J Magn Reson Imaging. 1997; 7:91–101.35. Brix G, Griebel J, Kiessling F, Wenz F. Tracer kinetic modelling of tumour angiogenesis based on dynamic contrast-enhanced CT and MRI measurements. Eur J Nucl Med Mol Imaging. 2010; 37:Suppl 1. S30–S51.36. Patankar TF, Haroon HA, Mills SJ, Balériaux D, Buckley DL, Parker GJ, et al. Is volume transfer coefficient (K(trans)) related to histologic grade in human gliomas? AJNR Am J Neuroradiol. 2005; 26:2455–2465.37. Marzola P, Degrassi A, Calderan L, Farace P, Crescimanno C, Nicolato E, et al. In vivo assessment of antiangiogenic activity of SU6668 in an experimental colon carcinoma model. Clin Cancer Res. 2004; 10:739–750.38. Klemm F, Joyce JA. Microenvironmental regulation of therapeutic response in cancer. Trends Cell Biol. 2015; 25:198–213.39. Sorensen AG, Batchelor TT, Zhang WT, Chen PJ, Yeo P, Wang M, et al. A "vascular normalization index" as potential mechanistic biomarker to predict survival after a single dose of cediranib in recurrent glioblastoma patients. Cancer Res. 2009; 69:5296–5300.40. Jain RK. Normalizing tumor microenvironment to treat cancer: bench to bedside to biomarkers. J Clin Oncol. 2013; 31:2205–2218.41. Sorensen AG, Emblem KE, Polaskova P, Jennings D, Kim H, Ancukiewicz M, et al. Increased survival of glioblastoma patients who respond to antiangiogenic therapy with elevated blood perfusion. Cancer Res. 2012; 72:402–407.42. Detre JA, Zhang W, Roberts DA, Silva AC, Williams DS, Grandis DJ, et al. Tissue specific perfusion imaging using arterial spin labeling. NMR Biomed. 1994; 7:75–82.43. Noguchi T, Yoshiura T, Hiwatashi A, Togao O, Yamashita K, Nagao E, et al. Perfusion imaging of brain tumors using arterial spin-labeling: correlation with histopathologic vascular density. AJNR Am J Neuroradiol. 2008; 29:688–693.44. Warmuth C, Gunther M, Zimmer C. Quantification of blood flow in brain tumors: comparison of arterial spin labeling and dynamic susceptibility-weighted contrast-enhanced MR imaging. Radiology. 2003; 228:523–532.45. Haacke EM, Xu Y, Cheng YC, Reichenbach JR. Susceptibility weighted imaging (SWI). Magn Reson Med. 2004; 52:612–618.46. Mittal S, Wu Z, Neelavalli J, Haacke EM. Susceptibility-weighted imaging: technical aspects and clinical applications, part 2. AJNR Am J Neuroradiol. 2009; 30:232–252.47. Sehgal V, Delproposto Z, Haacke EM, Tong KA, Wycliffe N, Kido DK, et al. Clinical applications of neuroimaging with susceptibility-weighted imaging. J Magn Reson Imaging. 2005; 22:439–450.48. Barth M, Nöbauer-Huhmann IM, Reichenbach JR, Mlynárik V, Schöggl A, Matula C, et al. High-resolution three-dimensional contrast-enhanced blood oxygenation level-dependent magnetic resonance venography of brain tumors at 3 Tesla: first clinical experience and comparison with 1.5 Tesla. Invest Radiol. 2003; 38:409–414.49. Fahrendorf D, Schwindt W, Wölfer J, Jeibmann A, Kooijman H, Kugel H, et al. Benefits of contrast-enhanced SWI in patients with glioblastoma multiforme. Eur Radiol. 2013; 23:2868–2879.50. Sampetrean O, Saga I, Nakanishi M, Sugihara E, Fukaya R, Onishi N, et al. Invasion precedes tumor mass formation in a malignant brain tumor model of genetically modified neural stem cells. Neoplasia. 2011; 13:784–791.51. Jones CK, Schlosser MJ, van Zijl PC, Pomper MG, Golay X, Zhou J. Amide proton transfer imaging of human brain tumors at 3T. Magn Reson Med. 2006; 56:585–592.52. Henkelman RM, Stanisz GJ, Graham SJ. Magnetization transfer in MRI: a review. NMR Biomed. 2001; 14:57–64.53. van Zijl PC, Yadav NN. Chemical exchange saturation transfer (CEST): what is in a name and what isn't? Magn Reson Med. 2011; 65:927–948.54. Zhou J, Zhu H, Lim M, Blair L, Quinones-Hinojosa A, Messina SA, et al. Three-dimensional amide proton transfer MR imaging of gliomas: initial experience and comparison with gadolinium enhancement. J Magn Reson Imaging. 2013; 38:1119–1128.55. Togao O, Yoshiura T, Keupp J, Hiwatashi A, Yamashita K, Kikuchi K, et al. Amide proton transfer imaging of adult diffuse gliomas: correlation with histopathological grades. Neuro Oncol. 2014; 16:441–448.56. Sagiyama K, Mashimo T, Togao O, Vemireddy V, Hatanpaa KJ, Maher EA, et al. In vivo chemical exchange saturation transfer imaging allows early detection of a therapeutic response in glioblastoma. Proc Natl Acad Sci U S A. 2014; 111:4542–4547.57. Park JE, Kim HS, Park KJ, Kim SJ, Kim JH, Smith SA. Pre- and posttreatment glioma: comparison of amide proton transfer imaging with MR spectroscopy for biomarkers of tumor proliferation. Radiology. 2016; 278:514–523.58. Chenevert TL, McKeever PE, Ross BD. Monitoring early response of experimental brain tumors to therapy using diffusion magnetic resonance imaging. Clin Cancer Res. 1997; 3:1457–1466.59. Lee EK, Choi SH, Yun TJ, Kang KM, Kim TM, Lee SH, et al. Prediction of response to concurrent chemoradiotherapy with temozolomide in glioblastoma: application ofimmediate post-operative dynamic susceptibility contrast and diffusion-weighted MR imaging. Korean J Radiol. 2015; 16:1341–1348.60. Ellingson BM, Sahebjam S, Kim HJ, Pope WB, Harris RJ, Woodworth DC, et al. Pretreatment ADC histogram analysis is a predictive imaging biomarker for bevacizumab treatment but not chemotherapy in recurrent glioblastoma. AJNR Am J Neuroradiol. 2014; 35:673–679.61. High WA, Ayers RA, Cowper SE. Gadolinium is quantifiable within the tissue of patients with nephrogenic systemic fibrosis. J Am Acad Dermatol. 2007; 56:710–712.62. Kanda T, Ishii K, Kawaguchi H, Kitajima K, Takenaka D. High signal intensity in the dentate nucleus and globus pallidus on unenhanced T1-weighted MR images: relationship with increasing cumulative dose of a gadolinium-based contrast material. Radiology. 2014; 270:834–841.63. Kim DY, Kim HS, Goh MJ, Choi CG, Kim SJ. Utility of intravoxel incoherent motion MR imaging for distinguishing recurrent metastatic tumor from treatment effect following gamma knife radiosurgery: initial experience. AJNR Am J Neuroradiol. 2014; 35:2082–2090.64. Kim HS, Suh CH, Kim N, Choi CG, Kim SJ. Histogram analysis of intravoxel incoherent motion for differentiating recurrent tumor from treatment effect in patients with glioblastoma: initial clinical experience. AJNR Am J Neuroradiol. 2014; 35:490–497.65. Bai Y, Lin Y, Tian J, Shi D, Cheng J, Haacke EM, et al. Grading of gliomas by using monoexponential, biexponential, and stretched exponential diffusion-weighted MR imaging and diffusion kurtosis MR imaging. Radiology. 2016; 278:496–504.66. Van Cauter S, Veraart J, Sijbers J, Peeters RR, Himmelreich U, De Keyzer F, et al. Gliomas: diffusion kurtosis MR imaging in grading. Radiology. 2012; 263:492–501.67. Brandsma D, Stalpers L, Taal W, Sminia P, van den Bent MJ. Clinical features, mechanisms, and management of pseudoprogression in malignant gliomas. Lancet Oncol. 2008; 9:453–461.68. Sanghera P, Perry J, Sahgal A, Symons S, Aviv R, Morrison M, et al. Pseudoprogression following chemoradiotherapy for glioblastoma multiforme. Can J Neurol Sci. 2010; 37:36–42.69. Kong DS, Kim ST, Kim EH, Lim DH, Kim WS, Suh YL, et al. Diagnostic dilemma of pseudoprogression in the treatment of newly diagnosed glioblastomas: the role of assessing relative cerebral blood flow volume and oxygen-6-methylguanine-DNA methyltransferase promoter methylation status. AJNR Am J Neuroradiol. 2011; 32:382–387.70. Chamberlain MC. Pseudoprogression in glioblastoma. J Clin Oncol. 2008; 26:4359. author reply 4359-4360.71. Baek HJ, Kim HS, Kim N, Choi YJ, Kim YJ. Percent change of perfusion skewness and kurtosis: a potential imaging biomarker for early treatment response in patients with newly diagnosed glioblastomas. Radiology. 2012; 264:834–843.72. Wang S, Martinez-Lage M, Sakai Y, Chawla S, Kim SG, Alonso-Basanta M, et al. Differentiating tumor progression from pseudoprogression in patients with glioblastomas using diffusion tensor imaging and dynamic susceptibility contrast MRI. AJNR Am J Neuroradiol. 2016; 37:28–36.73. Mangla R, Singh G, Ziegelitz D, Milano MT, Korones DN, Zhong J, et al. Changes in relative cerebral blood volume 1 month after radiation-temozolomide therapy can help predict overall survival in patients with glioblastoma. Radiology. 2010; 256:575–584.74. Radbruch A, Bendszus M, Wick W, Heiland S. Comment to: parametric response map as an imaging biomarker to distinguish progression from pseudoprogression in high-grade glioma: pitfalls in perfusion MRI in brain tumors: Tsien C, Galbán CJ, Chenevert TL, Johnson TD, Hamstra DA, Sundgren PC, Junck L, Meyer CR, Rehemtulla A, Lawrence T, Ross BD. J Clin Oncol. 2010;28:2293-9. Clin Neuroradiol. 2010; 20:183–184.75. Cheng HL, Wallis C, Shou Z, Farhat WA. Quantifying angiogenesis in VEGF-enhanced tissue-engineered bladder constructs by dynamic contrast-enhanced MRI using contrast agents of different molecular weights. J Magn Reson Imaging. 2007; 25:137–145.76. Leach MO, Brindle KM, Evelhoch JL, Griffiths JR, Horsman MR, Jackson A, et al. Assessment of antiangiogenic and antivascular therapeutics using MRI: recommendations for appropriate methodology for clinical trials. Br J Radiol. 2003; 76:Spec No 1. S87–S91.77. Kim HS, Goh MJ, Kim N, Choi CG, Kim SJ, Kim JH. Which combination of MR imaging modalities is best for predicting recurrent glioblastoma? Study of diagnostic accuracy and reproducibility. Radiology. 2014; 273:831–843.78. Narang J, Jain R, Arbab AS, Mikkelsen T, Scarpace L, Rosenblum ML, et al. Differentiating treatment-induced necrosis from recurrent/progressive brain tumor using nonmodel-based semiquantitative indices derived from dynamic contrast-enhanced T1-weighted MR perfusion. Neuro Oncol. 2011; 13:1037–1046.79. Li C, Ai B, Li Y, Qi H, Wu L. Susceptibility-weighted imaging in grading brain astrocytomas. Eur J Radiol. 2010; 75:e81–e85.80. Park MJ, Kim HS, Jahng GH, Ryu CW, Park SM, Kim SY. Semiquantitative assessment of intratumoral susceptibility signals using non-contrast-enhanced high-field high-resolution susceptibility-weighted imaging in patients with gliomas: comparison with MR perfusion imaging. AJNR Am J Neuroradiol. 2009; 30:1402–1408.81. Pinker K, Noebauer-Huhmann IM, Stavrou I, Hoeftberger R, Szomolanyi P, Karanikas G, et al. High-resolution contrast-enhanced, susceptibility-weighted MR imaging at 3T in patients with brain tumors: correlation with positron-emission tomography and histopathologic findings. AJNR Am J Neuroradiol. 2007; 28:1280–1286.82. Hori M, Ishigame K, Kabasawa H, Kumagai H, Ikenaga S, Shiraga N, et al. Precontrast and postcontrast susceptibility-weighted imaging in the assessment of intracranial brain neoplasms at 1.5 T. Jpn J Radiol. 2010; 28:299–304.83. Park JE, Kim HS, Park KJ, Choi CG, Kim SJ. Histogram analysis of amide proton transfer imaging to identify contrast-enhancing low-grade brain tumor that mimics high-grade tumor: increased accuracy of MR perfusion. Radiology. 2015; 277:151–161.84. Park KJ, Kim HS, Park JE, Shim WH, Kim SJ, Smith SA. Added value of amide proton transfer imaging to conventional and perfusion MR imaging for evaluating the treatment response of newly diagnosed glioblastoma. Eur Radiol. 2016; 02. 16. [Epub]. DOI: 10.1007/s00330-016-4261-2.85. Jung V, Romeike BF, Henn W, Feiden W, Moringlane JR, Zang KD, et al. Evidence of focal genetic microheterogeneity in glioblastoma multiforme by area-specific CGH on microdissected tumor cells. J Neuropathol Exp Neurol. 1999; 58:993–999.86. Park JE, Kim HS, Goh MJ, Kim SJ, Kim JH. Pseudoprogression in patients with glioblastoma: assessment by using volume-weighted voxel-based multiparametric clustering of MR imaging data in an independent test set. Radiology. 2015; 275:792–802.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Advanced Magnetic Resonance Imaging for Pediatric Brain Tumors: Current Imaging Techniques and Interpretation Algorithms
- Basics for Pediatric Brain Tumor Imaging: Techniques and Protocol Recommendations
- Modern Brain Tumor Imaging
- Current Applications and Future Perspectives of Brain Tumor Imaging
- Texture, Morphology, and Statistical Analysis to Differentiate Primary Brain Tumors on Two-Dimensional Magnetic Resonance Imaging Scans Using Artificial Intelligence Techniques
