Recent Advances in Ureteral Stents
- Affiliations
-
- 1Department of Radiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. jhshin@amc.seoul.kr
- KMID: 2457443
- DOI: http://doi.org/10.3348/jksr.2019.80.4.631
Abstract
- A ureteral stent is widely used to drain ureteral obstructions, which allows urine to bypass the obstruction. The double J stent, a representative ureteral stent, has undergone many advancements in material and design recently. In addition, indications of double J stent insertion have been broadly expanded to improve urinary obstruction before and after extracorporeal shock wave lithotripsy and to maintain ureteral patency after a ureteral surgery or treatment of a ureteral fistula. The recently developed metallic ureteral stents showed excellent long-term patency in patients with malignant ureteral strictures. Therefore, metallic stents could be an alternative to double J stents in select patients. In this review article, we describe the materials, designs, indications, details of the antegrade ureteral stenting procedure, and outcomes of the double J stent and metallic stent procedures.
MeSH Terms
Figure
-
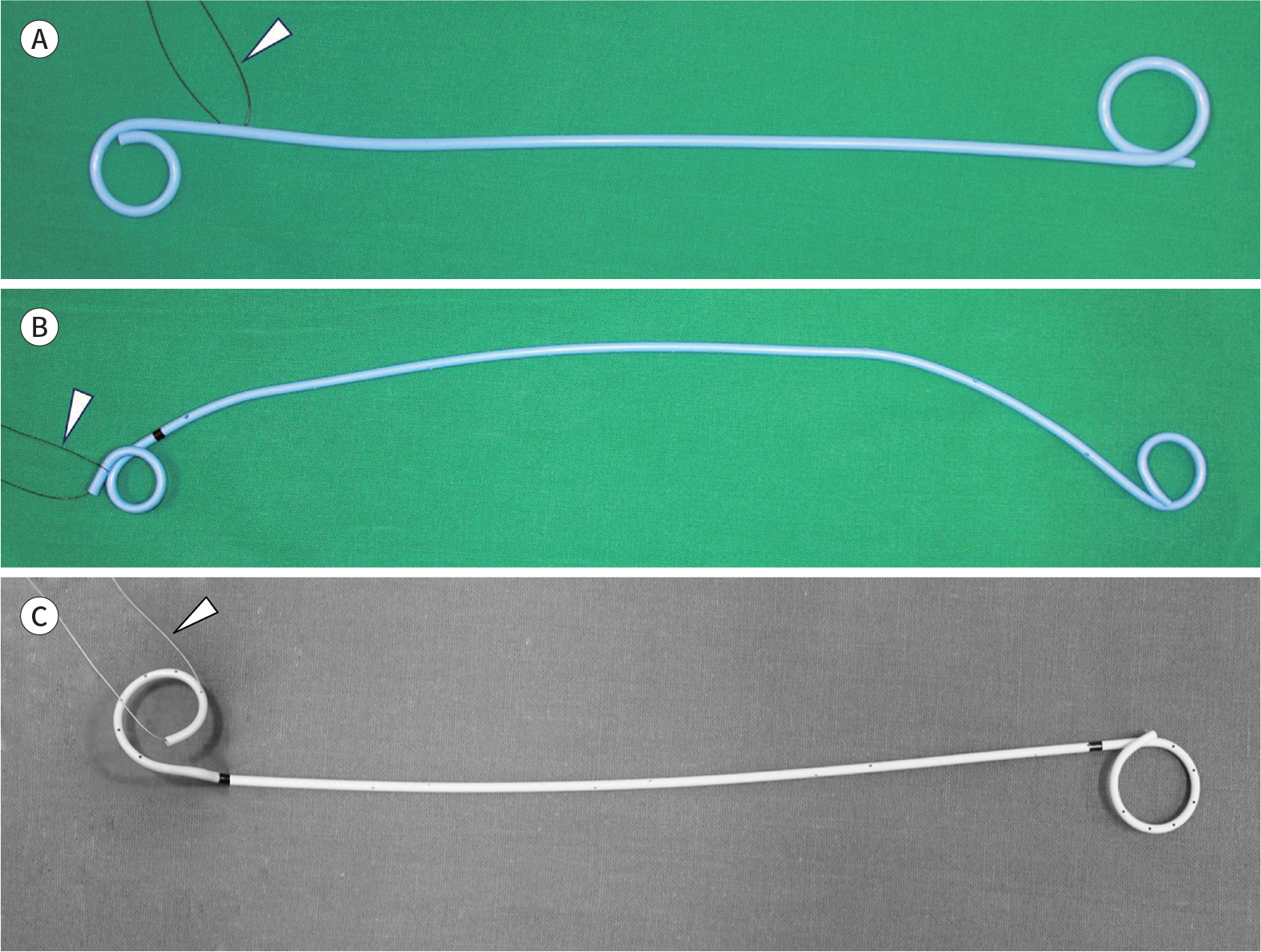
Fig. 1. Representative double J stents. A. Flexima ureteral stent. The proximal end of the shaft is sutured (arrowhead), with a pigtail loop in the renal pelvis. No radiopaque bands or side holes are present at the shaft. B. Percuflex ureteral stent. The proximal end of the pigtail is sutured (arrowhead). A radiopaque band (proximal shaft) and side holes are present at the shaft. C. Sof-flex ureteral stent. The proximal end of the pigtail is sutured (arrowhead). Two radiopaque bands (proximal and distal shaft) and side holes are present at the shaft.
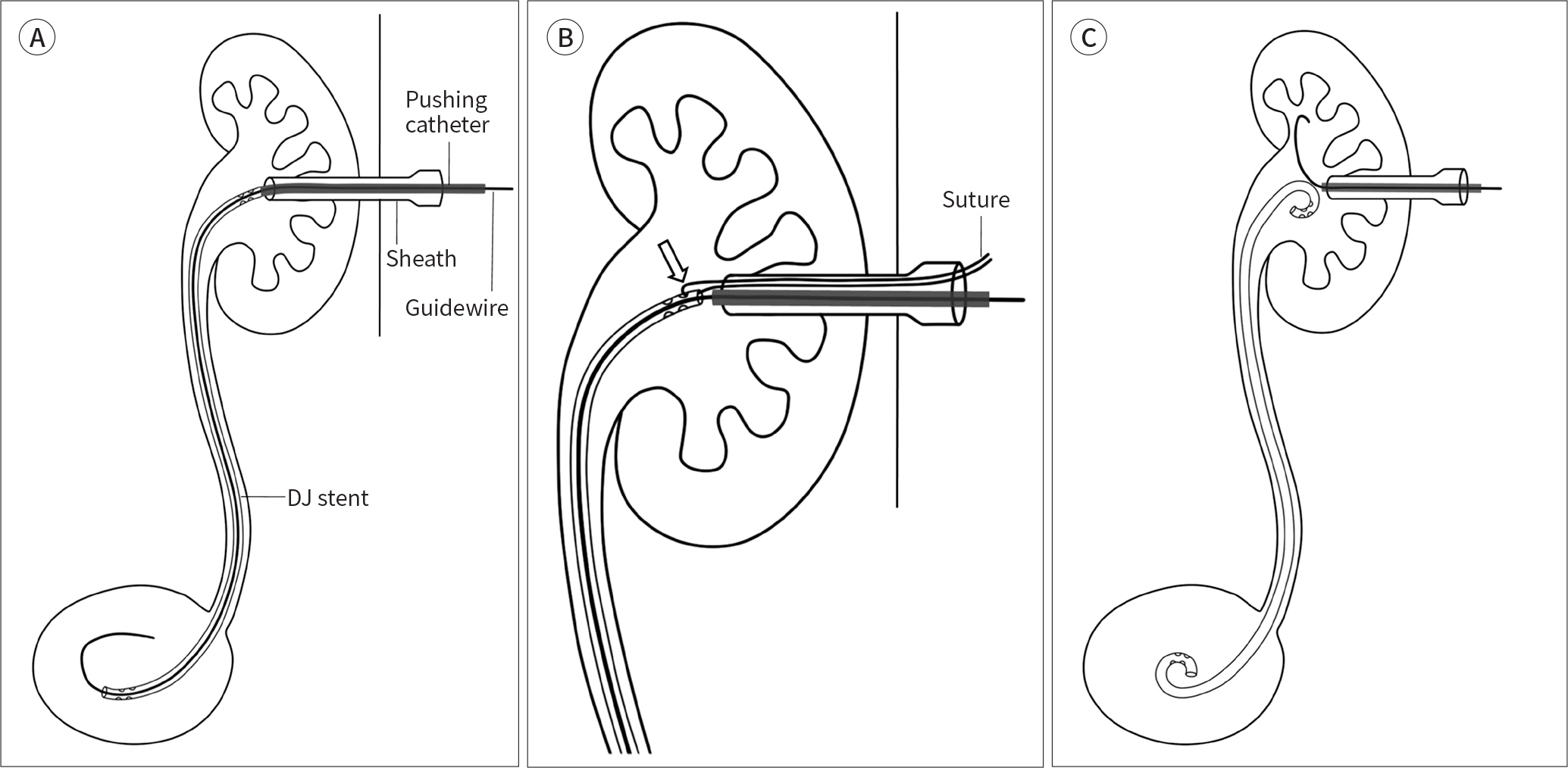
Fig. 2. Schema shows DJ stent insertion. A. The DJ stent is pushed into the urinary bladder using a pushing catheter. A 9 Fr sheath is usually used. B. On magnification, the suture loop (arrow) connected to the DJ stent is outside the body through the sheath. This loop is for repositioning and pigtail shaping. C. As a guidewire is out, the distal pigtail is positioned in the urinary bladder, and the proximal pigtail is positioned in the renal pelvis by manipulating the pushing catheter and suture loop. At the final position of the DJ stent, the suture loop is cut and removed. DJ = double J
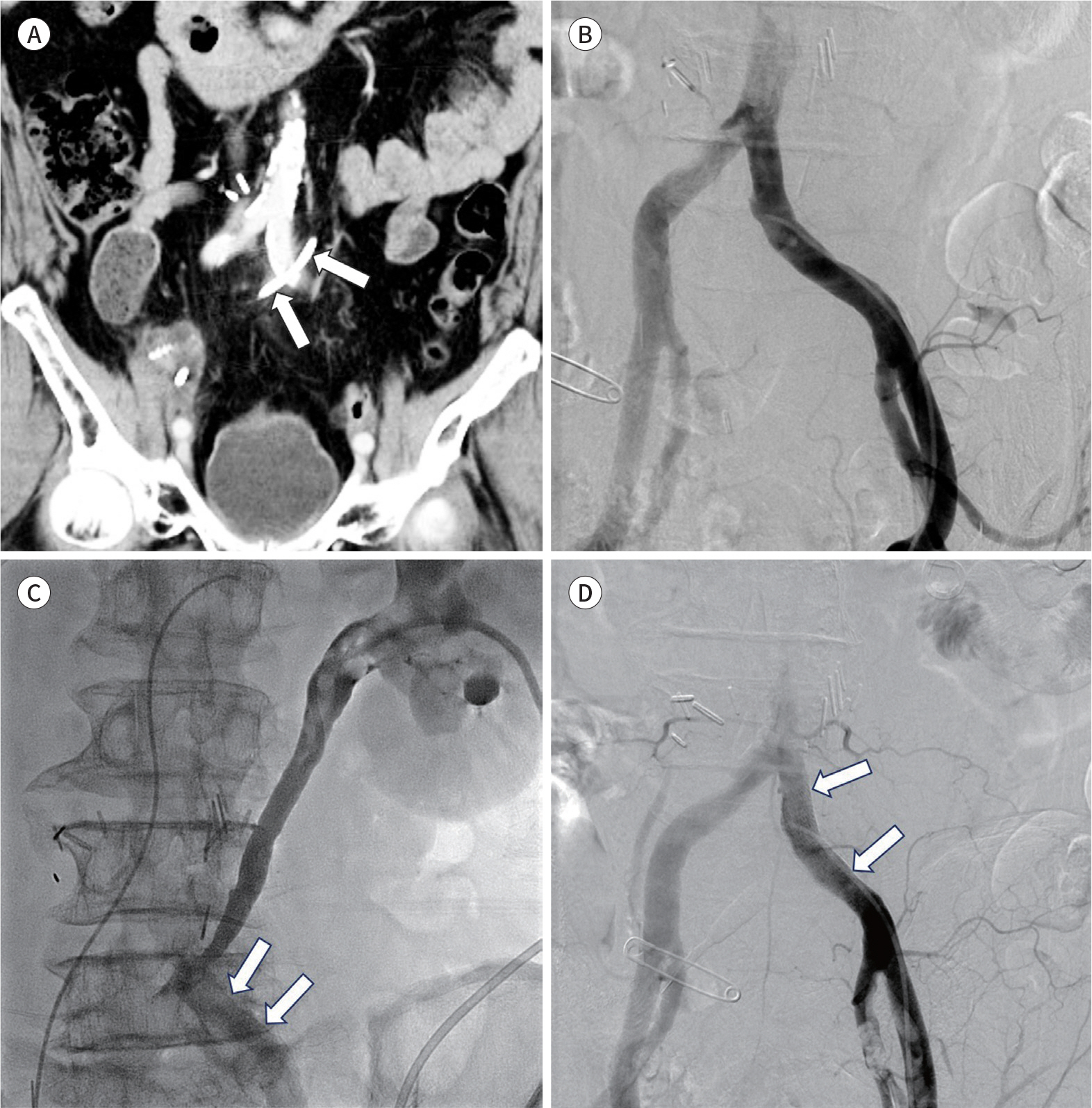
Fig. 3. A 70-year-old man who underwent radical cystectomy and neobladder formation for bladder cancer reports abrupt hematuria. A. On coronal CT, the left double J stent (arrows) inserted four months ago is noted adjacent to the left common iliac artery. B. The left common iliac angiogram shows no definite hematuria. The left renal angiogram shows no bleeding (not shown). C. The left renal pelvis irrigation through nephrostomy shows opacification of the left common iliac artery (arrows), revealing an arterioureteral fistula. The stent graft (13-mm diameter, 5-cm length) was inserted to seal off the fistula (not shown). D. The completion angiogram shows complete closure of the fistula after insertion of the stent graft (arrows). Hematuria has disappeared.
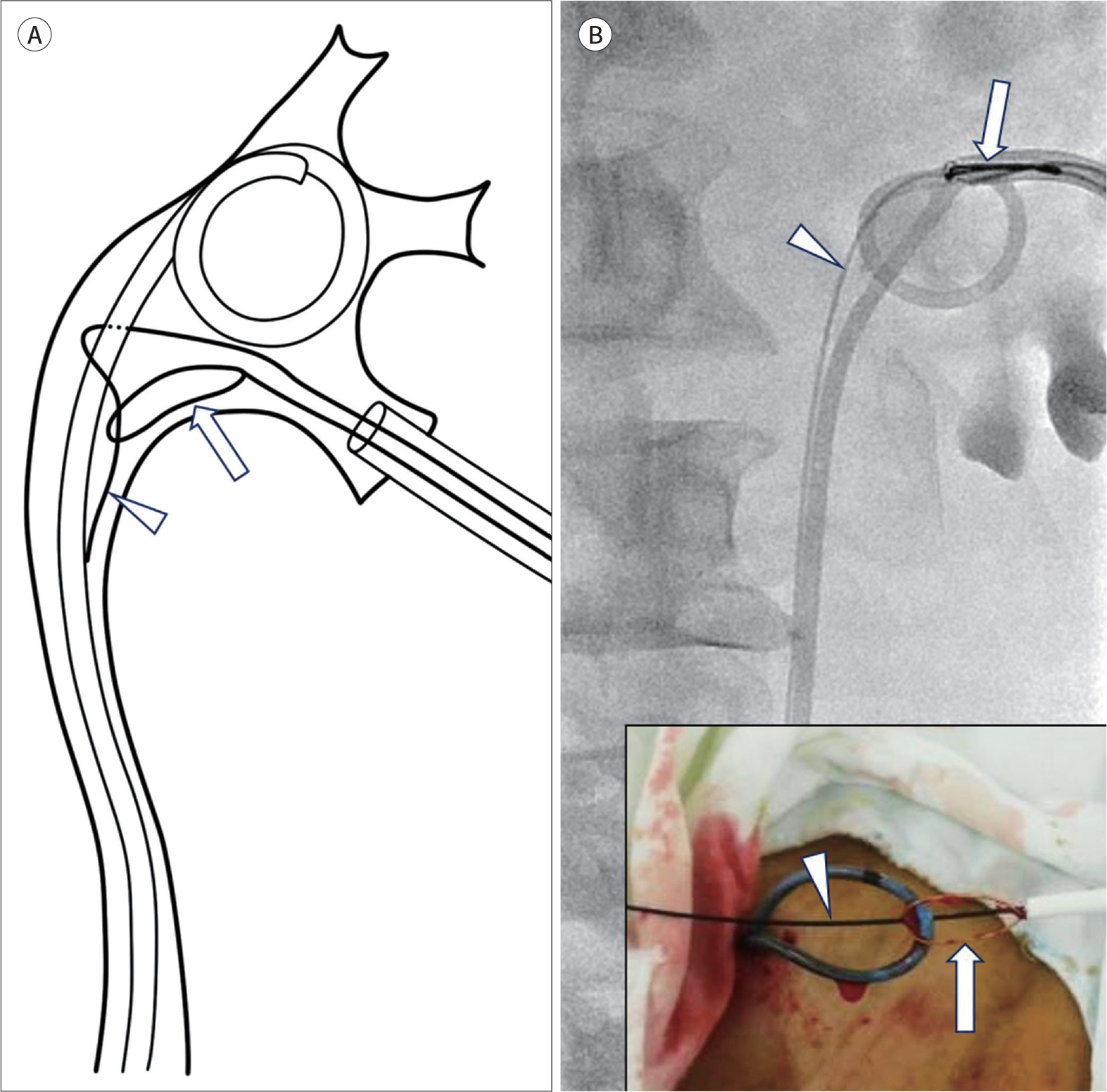
Fig. 4. The modified snare technique to remove the DJ stent is shown. Schematic illustration (A) and fluoroscopy (B) demonstrate a spatial relationship among the snare (arrows), guidewire (arrowheads), and DJ stent. After the guidewire winds around the DJ stent, it is snared to create a loop around the DJ stent. Subsequently, the entire assembly, including the DJ stent, guidewire, and snare-guiding sheath, is withdrawn through the sheath (inset in B). DJ = double J

Fig. 5. A 70-year-old man with advanced gastric cancer reports left hydronephrosis. A. Antegrade pyelogram via percutaneous nephrostomy tube shows multifocal, segmental ureteric strictures (arrows) from middle to distal ureter. B. The first stent (arrows) is inserted to cover the middle to distal ureter, following a 7-mm balloon dilation of the entire ureter. C. The second stent (arrows) is inserted to cover the proximal to middle ureter, followed by a repeated 7-mm balloon dilation (arrowheads). D. The antegrade pyelogram two days following metallic ureteral stent placements shows good flow of the contrast medium through metallic ureteral stents into the urinary bladder.
Reference
-
References
1. Mosayyebi A, Manes C, Carugo D, Somani BK. Advances in ureteral stent design and materials.Curr Urol Rep. 2018; 19:35.2. Zimskind PD, Fetter TR, Wilkerson JL. Clinical use of longterm indwelling silicone rubber ureteral splints inserted cystoscopically. J Urol. 1967; 97:840–844.
Article3. Finney RP. Experience with new double J ureteral catheter stent. J Urol. 1978; 120:678–681.
Article4. Kim JW, Hong B, Shin JH, Park J, Kim JH, Gwon DI, et al. A prospective randomized comparison of a covered metallic ureteral stent and a double-J stent for malignant ureteral obstruction. Korean J Radiol. 2018; 19:606–612.
Article5. Kim JH, Song K, Jo MK, Park JW. Palliative care of malignant ureteral obstruction with polytetrafluoroethylene membrane-covered self-expandable metallic stents: initial experience.Korean J Urol. 2012; 53:625–631.6. Chow PM, Chiang IN, Chen CY, Huang KH, Hsu JS, Wang SM, et al. Malignant ureteral obstruction: functional duration of metallic versus polymeric ureteral stents. PLoS One. 2015; 10:e0135566.
Article7. Asakawa J, Iguchi T, Tamada S, Ninomiya N, Kato M, Yamasaki T, et al. Treatment outcomes of ureteral stenting for malignant extrinsic ureteral obstruction: a comparison between polymeric and metallic stents. Cancer Manag Res. 2018; 10:2977–2982.
Article8. Dyer RB, Chen MY, Zagoria RJ, Regan JD, Hood CG, Kavanagh PV. Complications of ureteral stent placement. Radiographics. 2002; 22:1005–1022.
Article9. Al-Aown A, Kyriazis I, Kallidonis P, Kraniotis P, Rigopoulos C, Karnabatidis D, et al. Ureteral stents: new ideas, new designs. Ther Adv Urol. 2010; 2:85–92.
Article10. Youn SY, Oh JS, Lee HG, Choi BG, Chun HJ, Kim EH. Primary and secondary percutaneous ureteral stent placement: comparison of stent patency and clinical outcome. Cardiovasc Intervent Radiol. 2018; 41:130–136.
Article11. Patel U, Abubacker MZ. Ureteral stent placement without postprocedural nephrostomy tube: experience in 41 patients. Radiology. 2004; 230:435–442.
Article12. Watson GM, Patel U. Primary antegrade ureteric stenting: prospective experience and cost-effectiveness analysis in 50 ureters. Cl/iin Radiol. 2001; 56:568–574.
Article13. Van der Meer RW, Weltings S, Van Erkel AR, Roshani H, Elzevier HW, Van Dijk LC, et al. Antegrade ureteral stenting is a good alternative for the retrograde approach.Curr Urol. 2017; 10:87–91.14. Chung SY, Stein RJ, Landsittel D, Davies BJ, Cuellar DC, Hrebinko RL, et al. 15-year experience with the management of extrinsic ureteral obstruction with indwelling ureteral stents.J Urol. 2004; 172:592–595.15. Yossepowitch O, Lifshitz DA, Dekel Y, Gross M, Keidar DM, Neuman M, et al. Predicting the success of retrograde stenting for managing ureteral obstruction.J Urol. 2001; 166:1746–1749.16. Fine H, Gordon RL, Lebensart PD. Extracorporeal shock wave lithotripsy and stents: fluoroscopic observations and a hypothesis on the mechanisms of stent function. Urol Radiol. 1989; 11:37–41.
Article17. Watson G. Problems with double-J stents and nephrostomy tubes.J Endourol. 1997; 11:413–417.18. Saltzman B. Ureteral stents. Indications, variations, and complications.Urol Clin North Am. 1988; 15:481–491.
Article19. Matsuura H, Arase S, Hori Y. Ureteral stents for malignant extrinsic ureteral obstruction: outcomes and factors predicting stent failure.Int J Clin Oncol. 2019; 24:306–312.20. Chung HH, Kim MD, Won JY, Won JH, Cho SB, Seo TS, et al. Multicenter experience of the newly designed covered metallic ureteral stent for malignant ureteral occlusion: comparison with double J stent insertion. Cardiovasc Intervent Radiol. 2014; 37:463–470.
Article21. Lange D, Bidnur S, Hoag N, Chew BH. Ureteral stent-associated complications–where we are and where we are going.Nat Rev Urol. 2015; 12:17–25.22. Kawahara T, Ito H, Terao H, Yoshida M, Matsuzaki J. Ureteral stent encrustation, incrustation, and coloring: morbidity related to indwelling times.J Endourol. 2012; 26:178–182.23. Docimo SG, Dewolf WC. High failure rate of indwelling ureteral stents in patients with extrinsic obstruction: experience at 2 institutions. J Urol. 1989; 142:277–279.
Article24. Bergqvist D, Pärsson H, Sherif A. Arterio-ureteral fistula–a systematic review. Eur J Vasc Endovasc Surg. 2001; 22:191–196.25. Pillai AK, Anderson ME, Reddick MA, Sutphin PD, Kalva SP. Ureteroarterial fistula: diagnosis and management.A JR Am J Roentgenol. 2015; 204:W592–W598.26. Muraoka N, Sakai T, Kimura H, Kosaka N, Itoh H, Tanase K, et al. Endovascular treatment for an iliac artery-ureteral fistula with a covered stent. J Vasc Interv Radiol. 2006; 17:1681–1685.
Article27. Eisner BH, McGovern FJ. Management of ureteroiliac artery fistula.Semin Intervent Radiol. 2007; 24:117–118.28. Horikawa M, Saito H, Hokotate H, Mori T. Treatment of ureteroarterial fistula with an endoureteral stent graft. J Vasc Interv Radiol. 2012; 23:1241–1243.
Article29. LeRoy AJ, Williams HJ Jr, Segura JW, Patterson DE, Benson RC Jr. Indwelling ureteral stents: percutaneous management of complications. Radiology. 1986; 158:219–222.
Article30. Shin JH, Yoon HK, Ko GY, Sung KB, Song HY, Choi E, et al. Percutaneous antegrade removal of double J ureteral stents via a 9-F nephrostomy route. J Vasc Interv Radiol. 2007; 18:1156–1161.
Article31. Breen DJ, Cowan NC. Fluoroscopically-guided retrieval of ureteric stents.Clin Radiol. 1995; 50:860–863.32. Yeung EY, Carmody E, Thurston W, Ho CS. Percutaneous fluoroscopically guided removal of dysfunctioning ureteral stents.Radiology. 1994; 190:145–148.33. Liang HL, Yang TL, Huang JS, Lin YH, Chou CP, Chen MC, et al. Antegrade retrieval of ureteral stents through an 8-French percutaneous nephrostomy route. AJR Am J Roentgenol. 2008; 191:1530–1535.
Article34. Park SW, Cha IH, Hong SJ, Yi JG, Jeon HJ, Park JH, et al. Fluoroscopy-guided transurethral removal and exchange of ureteral stents in female patients: technical notes. J Vasc Interv Radiol. 2007; 18:251–256.
Article35. McCarthy E, Kavanagh J, McKernan S, O'Mahony N, McEniff N, Ryan JM, et al. Fluoroscopically guided transurethral removal and/or replacement of ureteric stents in women. Acta Radiol. 2015; 56:635–640.
Article36. Pedro RN, Hendlin K, Kriedberg C, Monga M. Wire-based ureteral stents: impact on tensile strength and compression. Urology. 2007; 70:1057–1059.
Article37. Lugmayr HF, Pauer W. Wallstents for the treatment of extrinsic malignant ureteral obstruction: midterm results. Radiology. 1996; 198:105–108.
Article38. Flueckiger F, Lammer J, Klein GE, Hausegger K, Lederer A, Szolar D, et al. Malignant ureteral obstruction: preliminary results of treatment with metallic self-expandable stents.Radiology. 1993; 186:169–173.39. Chung KJ, Park BH, Park B, Lee JH, Kim WJ, Baek M, et al. Efficacy and safety of a novel, double-layered, coated, self-expandable metallic mesh stent (UventaTM) in malignant ureteral obstructions.J Endourol. 2013; 27:930–935.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Percutaneous placement of ureteral stent
- Recent Advances in Gastrointestinal Stent Development
- Antegrade Ureteral Stenting in Ureteral Obstruction
- Adverse Effects of Ureteral Stent and Development of the Antireflux Ureteral Stent
- Removal of Migrated Thermo-Expandable Ureteral Stent (Memokath): Open Procedure 1 Case
