Constrictive Pericarditis: A Medical or Surgical Disease?
- Affiliations
-
- 1Division of Cardiology, Department of Medicine, Heart Vascular Stroke Institute, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. elisabet.chang@gmail.com
- 2Department of Cardiovascular Medicine, Mayo Clinic College of Medicine, Rochester, MN, USA.
- KMID: 2456853
- DOI: http://doi.org/10.4250/jcvi.2019.27.e28
Abstract
- Constrictive pericarditis is a disease of the pericardium resulting from chronic inflammation and/or scar responsible for a clinical feature of left and right ventricular failure. Although constrictive pericarditis has long been considered a surgical disease, a subset of patients experience reversibility of pericardial inflammation, a condition referred to as "transient constriction." Thus, after establishing the diagnosis of constrictive pericarditis, it is essential to evaluate the duration and potential for reversal to determine an appropriate treatment plan. Evidence of chronic disease can be acquired from the patient's clinical features and cardiac imaging, especially calcifications seen on computed tomography and chest X-ray. Transient constrictive pericarditis should be considered in cases without evidence of chronic disease, as active inflammation of the pericardium can be treated medically. Resolution of constrictive physiology can be evaluated using serial transthoracic 2-D Doppler echocardiography along with clinical examination. The potential for reversibility may also be assessed with multi-modality cardiac imaging to look for evidence of late enhancement on cardiac magnetic resonance and ¹â¸F-FDG PET/CT imaging.
Keyword
MeSH Terms
Figure
-
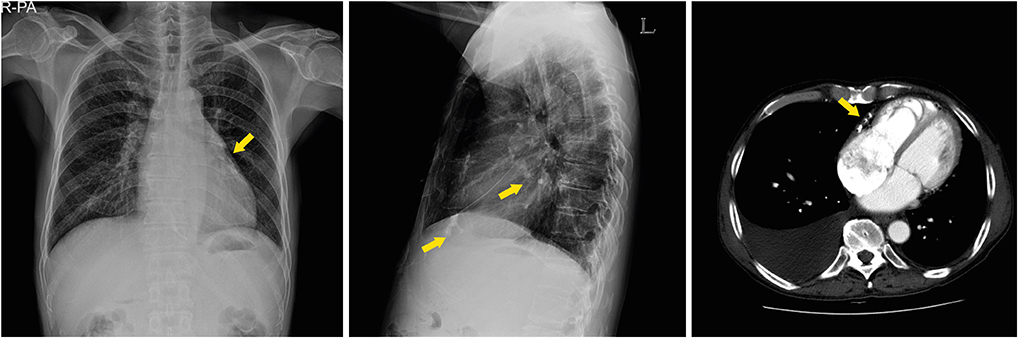
Figure 1 Calcification (yellow arrows) of the pericardium in simple chest X-ray (A, B) and CT (C).
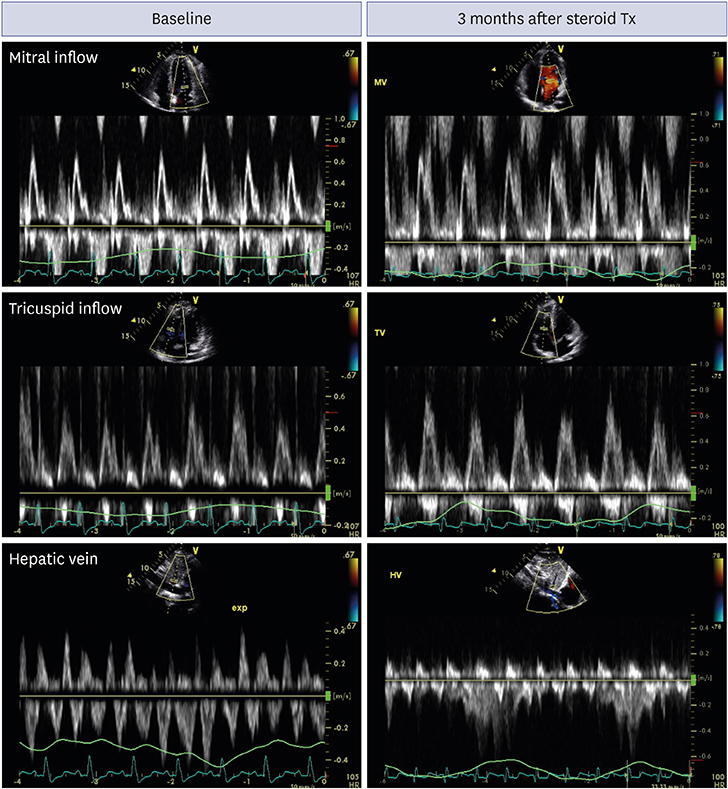
Figure 2 Doppler examination using transthoracic echocardiography is helpful to assess constrictive physiology during treatment. At baseline, respiratory variation of mitral and tricuspid inflow was exaggerated, and diastolic flow reversal during expiration was prominent. After 3 months of steroid therapy, there was no evidence of constrictive physiology.

Figure 3 Use of cardiac magnetic resonance imaging to diagnose transient constrictive pericarditis. A 32-year-old man was diagnosed with tuberculous pericarditis. Prior to treatment, the pericardium was thickened (left upper panel) and exhibited signs of late enhancement (left lower panel). After steroid therapy and anti-tuberculous medication, the pericardial thickness normalized and late enhancement of the pericardium resolved.

Figure 4 FDG-PET. Maximum-intensity projection (upper row) and fused transaxial PET/CT (lower row) images of a 32-year-old male patient showing significant and diffuse high 18F-FDG uptake in the pericardium (left panel, SUVmax = 16.0). After steroid therapy, the patient was free of symptoms, and 18F-FDG uptake in the pericardium was markedly decreased (right panel, SUVmax = 3.5). CT: computed tomography, FDG: fluorodeoxyglucose, PET: positron emission tomography.
Cited by 2 articles
-
Early Testing and Prompt Initiation of Proper Treatment: a Clever Strategy to Fight with Tuberculosis Pericarditis
Iksung Cho, William Dowon Kim
Korean Circ J. 2020;50(7):610-612. doi: 10.4070/kcj.2020.0179.Septal Bounce or Ventricle Interdependence in Constrictive Pericarditis: Same or Different
Sourabh Agstam
Korean Circ J. 2020;50(7):628-629. doi: 10.4070/kcj.2020.0178.
Reference
-
1. Bertog SC, Thambidorai SK, Parakh K, et al. Constrictive pericarditis: etiology and cause-specific survival after pericardiectomy. J Am Coll Cardiol. 2004; 43:1445–1452.
Article2. Chowdhury UK, Subramaniam GK, Kumar AS, et al. Pericardiectomy for constrictive pericarditis: a clinical, echocardiographic, and hemodynamic evaluation of two surgical techniques. Ann Thorac Surg. 2006; 81:522–529.
Article3. Copeland JG, Stinson EB, Griepp RB, Shumway NE. Surgical treatment of chronic constrictive pericarditis using cardiopulmonary bypass. J Thorac Cardiovasc Surg. 1975; 69:236–238.
Article4. DeValeria PA, Baumgartner WA, Casale AS, et al. Current indications, risks, and outcome after pericardiectomy. Ann Thorac Surg. 1991; 52:219–224.
Article5. Harrington SW. Chronic constrictive pericarditis: partial pericardiectomy and epicardiolysis in twenty-four cases. Ann Surg. 1944; 120:468–485.6. Ling LH, Oh JK, Schaff HV, et al. Constrictive pericarditis in the modern era: evolving clinical spectrum and impact on outcome after pericardiectomy. Circulation. 1999; 100:1380–1386.7. Kang SH, Song JM, Kim M, et al. Prognostic predictors in pericardiectomy for chronic constrictive pericarditis. J Thorac Cardiovasc Surg. 2014; 147:598–605.
Article8. Møller S, Bernardi M. Interactions of the heart and the liver. Eur Heart J. 2013; 34:2804–2811.
Article9. Bogaert J, Meyns B, Dymarkowski S, Sinnaeve P, Meuris B. Calcified constrictive pericarditis: prevalence, distribution patterns, and relationship to the myocardium. JACC Cardiovasc Imaging. 2016; 9:1013–1014.
Article10. Aagaard MT, Haraldsted VY. Chronic constrictive pericarditis treated with total pericardiectomy. Thorac Cardiovasc Surg. 1984; 32:311–314.
Article11. Permanyer-Miralda G, Sagristá-Sauleda J, Soler-Soler J. Primary acute pericardial disease: a prospective series of 231 consecutive patients. Am J Cardiol. 1985; 56:623–630.
Article12. Oh JK, Hatle LK, Mulvagh SL, Tajik AJ. Transient constrictive pericarditis: diagnosis by two-dimensional Doppler echocardiography. Mayo Clin Proc. 1993; 68:1158–1164.
Article13. Oh JY, Chang SA, Choe YH, Kim DK. Transient constrictive pericarditis in systemic lupus erythematous. Eur Heart J Cardiovasc Imaging. 2012; 13:793.
Article14. Woods T, Vidarsson B, Mosher D, Stein JH. Transient effusive-constrictive pericarditis due to chemotherapy. Clin Cardiol. 1999; 22:316–318.
Article15. Sagristà-Sauleda J, Permanyer-Miralda G, Candell-Riera J, Angel J, Soler-Soler J. Transient cardiac constriction: an unrecognized pattern of evolution in effusive acute idiopathic pericarditis. Am J Cardiol. 1987; 59:961–966.16. Haley JH, Tajik AJ, Danielson GK, Schaff HV, Mulvagh SL, Oh JK. Transient constrictive pericarditis: causes and natural history. J Am Coll Cardiol. 2004; 43:271–275.
Article17. Raviglione MC, Snider DE Jr, Kochi A. Global epidemiology of tuberculosis. Morbidity and mortality of a worldwide epidemic. JAMA. 1995; 273:220–226.18. Yang HS, Song JK, Song JM, et al. Clinical characteristics of constrictive pericarditis diagnosed by echo-Doppler technique in Korea. J Korean Med Sci. 2001; 16:558–566.
Article19. Chang SA, Choi JY, Kim EK, et al. [(18)F]Fluorodeoxyglucose PET/CT predicts response to steroid therapy in constrictive pericarditis. J Am Coll Cardiol. 2017; 69:750–752.
Article20. Feng D, Glockner J, Kim K, et al. Cardiac magnetic resonance imaging pericardial late gadolinium enhancement and elevated inflammatory markers can predict the reversibility of constrictive pericarditis after anti-inflammatory medical therapy: a pilot study. Circulation. 2011; 124:1830–1837.21. Oh JK, Hatle LK, Seward JB, et al. Diagnostic role of Doppler echocardiography in constrictive pericarditis. J Am Coll Cardiol. 1994; 23:154–162.
Article22. Taylor AM, Dymarkowski S, Verbeken EK, Bogaert J. Detection of pericardial inflammation with late-enhancement cardiac magnetic resonance imaging: initial results. Eur Radiol. 2006; 16:569–574.
Article23. Vaidyanathan S, Patel CN, Scarsbrook AF, Chowdhury FU. FDG PET/CT in infection and inflammation--current and emerging clinical applications. Clin Radiol. 2015; 70:787–800.
Article24. Huet P, Burg S, Le Guludec D, Hyafil F, Buvat I. Variability and uncertainty of 18F-FDG PET imaging protocols for assessing inflammation in atherosclerosis: suggestions for improvement. J Nucl Med. 2015; 56:552–559.
Article25. Dong A, Dong H, Wang Y, Cheng C, Zuo C, Lu J. (18)F-FDG PET/CT in differentiating acute tuberculous from idiopathic pericarditis: preliminary study. Clin Nucl Med. 2013; 38:e160–5.26. Nakao K, Noguchi T, Kim J, et al. Transient constrictive pericarditis diagnosed by cardiac magnetic resonance, 67Ga scintigraphy, and positron emission tomography. Int J Cardiol. 2009; 137:e70–2.
Article27. Strang JI, Kakaza HH, Gibson DG, Girling DJ, Nunn AJ, Fox W. Controlled trial of prednisolone as adjuvant in treatment of tuberculous constrictive pericarditis in Transkei. Lancet. 1987; 2:1418–1422.
Article28. Chang SA. Tuberculous and infectious pericarditis. Cardiol Clin. 2017; 35:615–622.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Constrictive Pericarditis Following Acute Idiopathic Pericarditis
- Tuberculous Constrictive Pericarditis: A Classical Case and Review
- Constrictive Pericarditis as a Never Ending Story: What's New?
- Echocardiographic Evaluation of Constrictive Pericarditis
- A Case of Constrictive Pericarditis with Localized Pericardial Effusion Simulating a Cystic Mass
