Cancer Res Treat.
2016 Apr;48(2):583-595. 10.4143/crt.2015.091.
Surgery Alone Versus Surgery Followed by Chemotherapy and Radiotherapy in Resected Extrahepatic Bile Duct Cancer: Treatment Outcome Analysis of 336 Patients
- Affiliations
-
- 1Department of Radiation Oncology, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea.
- 2Department of Radiation Oncology, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Korea. ikjae412@yuhs.ac
- 3Department of Surgery, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Korea.
- 4Department of Surgery, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea.
- 5Department of Radiation Oncology, Ewha Womans University Medical Center, Seoul, Korea.
- KMID: 2454336
- DOI: http://doi.org/10.4143/crt.2015.091
Abstract
- PURPOSE
This study analyzed the outcomes of patients with resected extrahepatic bile duct cancer (EHBDC) in order to clarify the role of adjuvant treatments in these patients.
MATERIALS AND METHODS
A total of 336 patients with EHBDC who underwent curative resection between 2001 and 2010 were analyzed retrospectively. The treatment types were as follows: surgery alone (n=168), surgery with chemotherapy (CTx, n=90), surgery with radiotherapy (RT) alone (n=29), and surgery with chemoradiotherapy (CRT, n=49).
RESULTS
The median follow-up period was 63 months. The 5-year rates of locoregional failure-free survival (LRFFS), distant metastasis-free survival (DMFS), progression-free survival (PFS), and overall survival (OS) for all patients were 56.5%, 59.7%, 36.6%, and 42.0%, respectively. In multivariate analysis, surgery with RT and CRT was a significant prognostic factor for LRFFS, and surgery with CTx was a significant prognostic factor for DMFS, and surgery with CTx, RT, and CRT was a significant prognostic factor for PFS (p < 0.05). Surgery with CTx and CRT showed association with superior OS (p < 0.05), and surgery with RT had marginal significance (p=0.078). In multivariate analysis of the R1 resection patients, surgery with CRT showed significant association with OS (p < 0.05).
CONCLUSION
Adjuvant RT and CTx may be helpful in improving clinical outcomes of patients with resected EHBDC who have a high risk of disease recurrence, particularly R1 resection patients. Conduct of additional prospective, larger-scale studies will be required in order to confirm the benefit of adjuvant RT and CTx in these patients.
Keyword
MeSH Terms
Figure
-
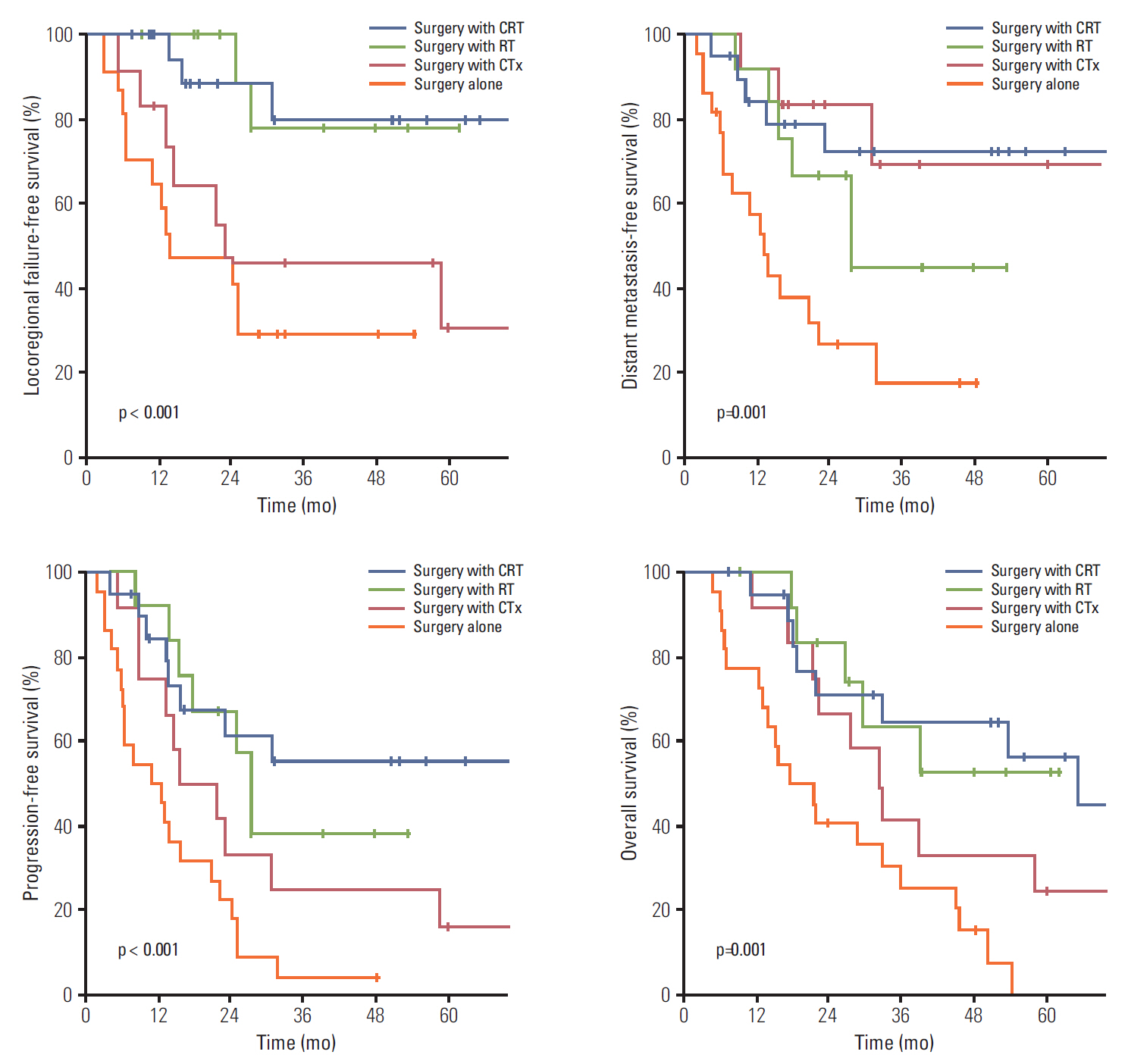
Fig. 1. Comparison of survival curves according to treatment type in patients with R1 resection. CRT, chemoradiotherapy; RT, radiotherapy; CTx, chemotherapy.
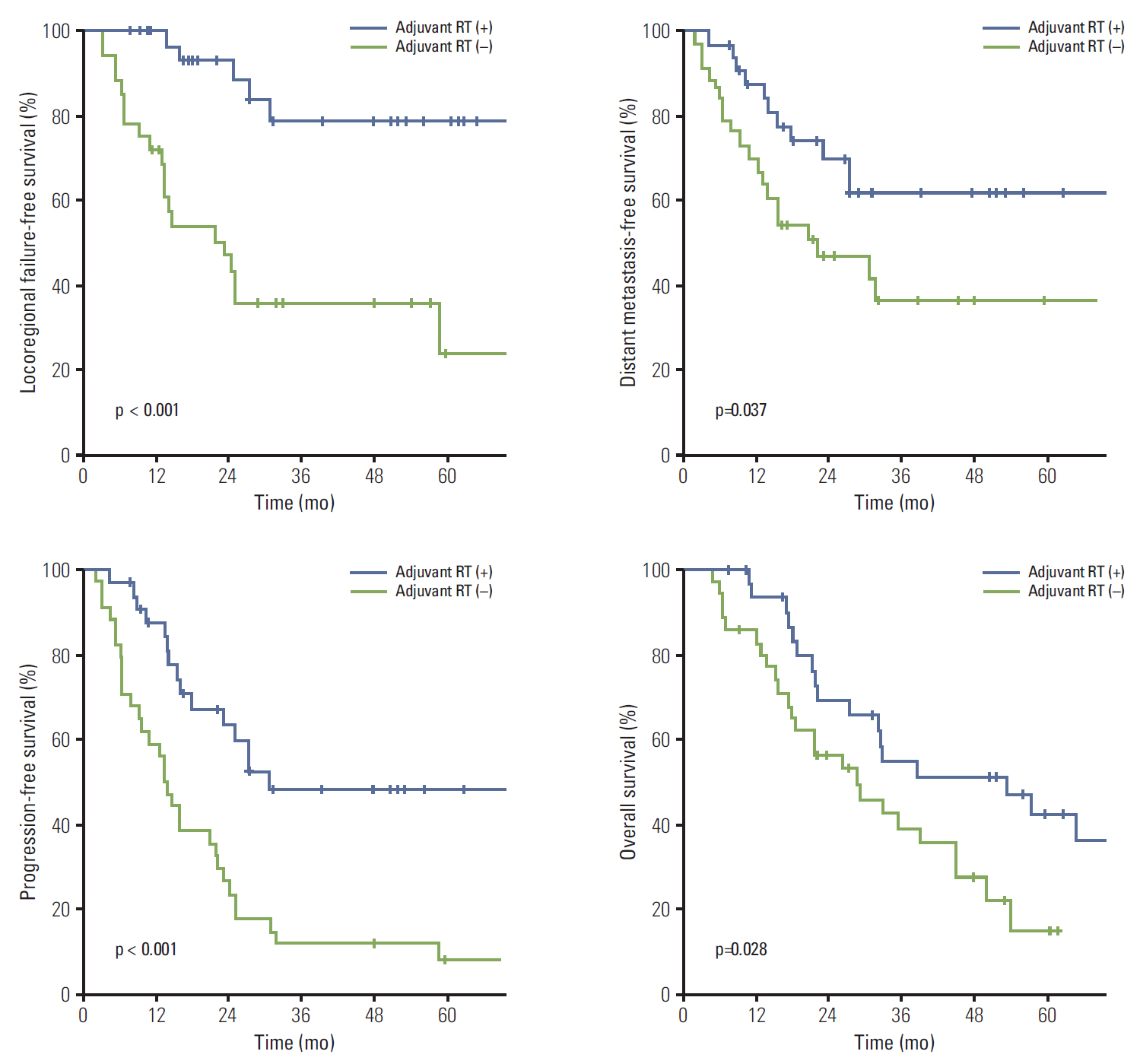
Fig. 2. Combined comparison of survival curves according to treatment type (surgery alone and surgery with chemotherapy vs. surgery with radiotherapy [RT] and surgery with chemoradiotherapy) in patients with R1 resection.
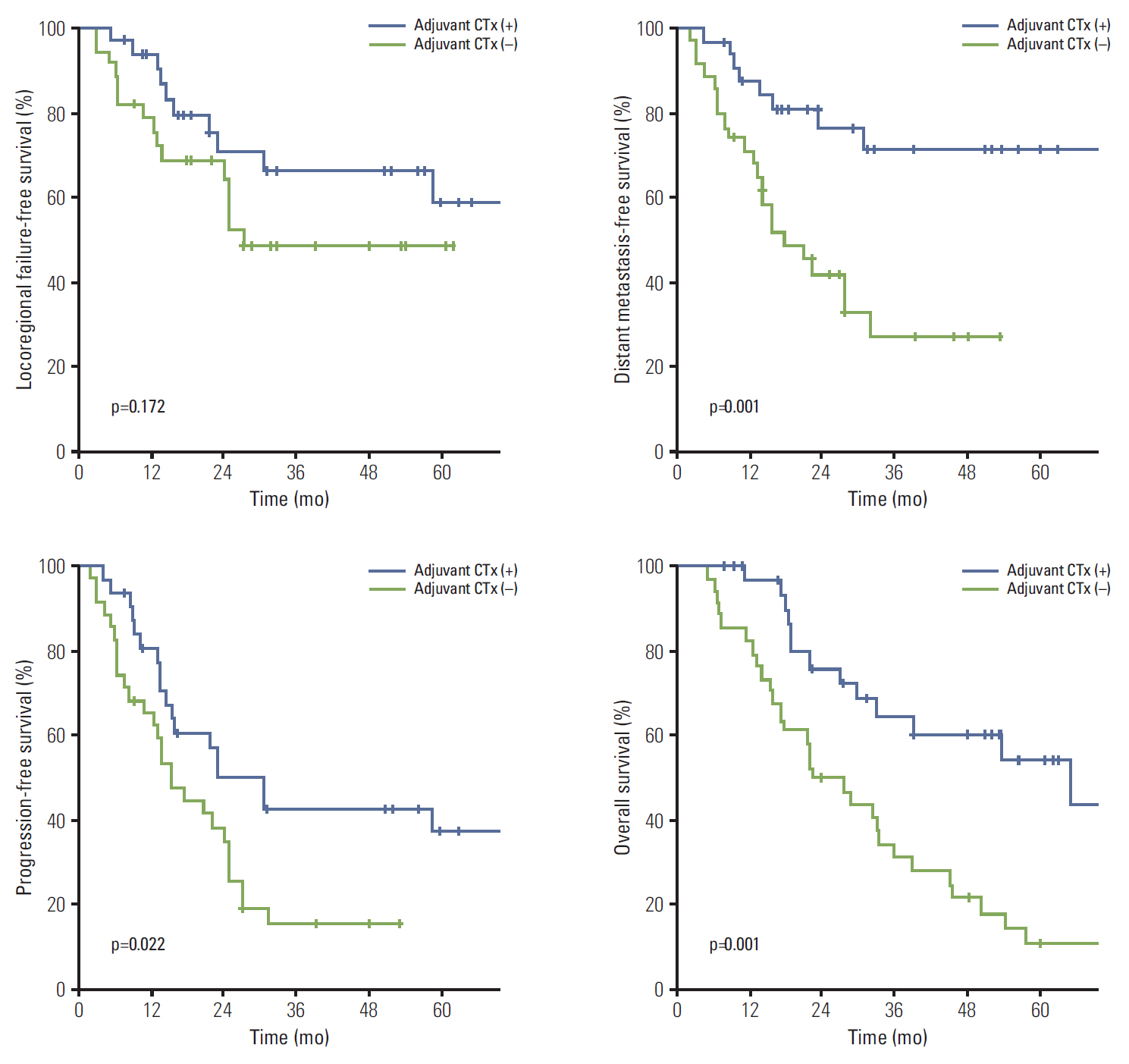
Fig. 3. Combined comparison of survival curves according to treatment type (surgery alone and surgery with radiotherapy vs. surgery with chemotherapy [CTx] and surgery with chemoradiotherapy) in patients with R1 resection.
Reference
-
References
1. Khan SA, Thomas HC, Davidson BR, Taylor-Robinson SD. Cholangiocarcinoma. Lancet. 2005; 366:1303–14.
Article2. Murakami Y, Uemura K, Sudo T, Hashimoto Y, Kondo N, Nakagawa N, et al. Perineural invasion in extrahepatic cholangiocarcinoma: prognostic impact and treatment strategies. J Gastrointest Surg. 2013; 17:1429–39.
Article3. Gwak HK, Kim WC, Kim HJ, Park JH. Extrahepatic bile duct cancers: surgery alone versus surgery plus postoperative radiation therapy. Int J Radiat Oncol Biol Phys. 2010; 78:194–8.
Article4. Jung KW, Won YJ, Kong HJ, Oh CM, Seo HG, Lee JS. Cancer statistics in Korea: incidence, mortality, survival and prevalence in 2010. Cancer Res Treat. 2013; 45:1–14.
Article5. Todoroki T, Ohara K, Kawamoto T, Koike N, Yoshida S, Kashiwagi H, et al. Benefits of adjuvant radiotherapy after radical resection of locally advanced main hepatic duct carcinoma. Int J Radiat Oncol Biol Phys. 2000; 46:581–7.
Article6. Todoroki T, Kawamoto T, Koike N, Fukao K, Shoda J, Takahashi H. Treatment strategy for patients with middle and lower third bile duct cancer. Br J Surg. 2001; 88:364–70.
Article7. Borghero Y, Crane CH, Szklaruk J, Oyarzo M, Curley S, Pisters PW, et al. Extrahepatic bile duct adenocarcinoma: patients at high-risk for local recurrence treated with surgery and adjuvant chemoradiation have an equivalent overall survival to patients with standard-risk treated with surgery alone. Ann Surg Oncol. 2008; 15:3147–56.
Article8. Kim TH, Han SS, Park SJ, Lee WJ, Woo SM, Moon SH, et al. Role of adjuvant chemoradiotherapy for resected extrahepatic biliary tract cancer. Int J Radiat Oncol Biol Phys. 2011; 81:e853–9.
Article9. Fuller CD, Wang SJ, Choi M, Czito BG, Cornell J, Welzel TM, et al. Multimodality therapy for locoregional extrahepatic cholangiocarcinoma: a population-based analysis. Cancer. 2009; 115:5175–83.10. Sagawa N, Kondo S, Morikawa T, Okushiba S, Katoh H. Effectiveness of radiation therapy after surgery for hilar cholangiocarcinoma. Surg Today. 2005; 35:548–52.
Article11. Vern-Gross TZ, Shivnani AT, Chen K, Lee CM, Tward JD, MacDonald OK, et al. Survival outcomes in resected extrahepatic cholangiocarcinoma: effect of adjuvant radiotherapy in a surveillance, epidemiology, and end results analysis. Int J Radiat Oncol Biol Phys. 2011; 81:189–98.
Article12. Im JH, Seong J, Lee J, Kim YB, Lee IJ, Park JS, et al. Postoperative radiotherapy dose correlates with locoregional control in patients with extra-hepatic bile duct cancer. Radiat Oncol J. 2014; 32:7–13.
Article13. Jarnagin WR, Ruo L, Little SA, Klimstra D, D'Angelica M, DeMatteo RP, et al. Patterns of initial disease recurrence after resection of gallbladder carcinoma and hilar cholangiocarcinoma: implications for adjuvant therapeutic strategies. Cancer. 2003; 98:1689–700.14. Choi SB, Park SW, Kim KS, Choi JS, Lee WJ. The survival outcome and prognostic factors for middle and distal bile duct cancer following surgical resection. J Surg Oncol. 2009; 99:335–42.
Article15. Koo TR, Eom KY, Kim IA, Cho JY, Yoon YS, Hwang DW, et al. Patterns of failure and prognostic factors in resected extrahepatic bile duct cancer: implication for adjuvant radiotherapy. Radiat Oncol J. 2014; 32:63–9.
Article16. Park JH, Choi EK, Ahn SD, Lee SW, Song SY, Yoon SM, et al. Postoperative chemoradiotherapy for extrahepatic bile duct cancer. Int J Radiat Oncol Biol Phys. 2011; 79:696–704.
Article17. Kim K, Chie EK, Jang JY, Kim SW, Han SW, Oh DY, et al. Adjuvant chemoradiotherapy after curative resection for extrahepatic bile duct cancer: a long-term single center experience. Am J Clin Oncol. 2012; 35:136–40.18. Takada T, Amano H, Yasuda H, Nimura Y, Matsushiro T, Kato H, et al. Is postoperative adjuvant chemotherapy useful for gallbladder carcinoma? A phase III multicenter prospective randomized controlled trial in patients with resected pancreaticobiliary carcinoma. Cancer. 2002; 95:1685–95.19. Lim KH, Oh DY, Chie EK, Jang JY, Im SA, Kim TY, et al. Adjuvant concurrent chemoradiation therapy (CCRT) alone versus CCRT followed by adjuvant chemotherapy: which is better in patients with radically resected extrahepatic biliary tract cancer?: a non-randomized, single center study. BMC Cancer. 2009; 9:345.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Effect of Adjuvant Therapy for Curatively Resected Extrahepatic Bile Duct Cancer
- Extrahepatic Bile Duct Duplication with Intraductal Papillary Neoplasm: A Case Report
- Recurrent pyogenic cholangitis: The pattern of thickening of the extrahepatic bile duct on CT
- Significance of EGFR and c-erbB-2 Expression in Extrahepatic Bile Duct Cancer
- Treatment Outcome of Postoperative Radiotherapy in Extrahepatic Bile Duct Cancer
