Cancer Res Treat.
2016 Apr;48(2):561-566. 10.4143/crt.2015.114.
Multimodal Assessments Are Needed for Restaging after Neoadjunvant Chemoradiation Therapy in Rectal Cancer Patients
- Affiliations
-
- 1Department of Surgery, St. Vincent's Hospital, College of Medicine, The Catholic University of Korea, Suwon, Korea. hmcho@catholic.ac.kr
- 2Department of Surgery, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea.
- KMID: 2454333
- DOI: http://doi.org/10.4143/crt.2015.114
Abstract
- PURPOSE
Restaging after neoadjuvant treatment is done for planning the surgical approach and, increasingly, to determine whether additional therapy or resection can be avoided for selected patients.
MATERIALS AND METHODS
Local restaging after neoadjuvant chemoradiation therapy (nCRT) was performed in 270 patients with locally advanced (cT3or4 or N+) rectal cancer. Abdomen and pelvic computed tomography (APCT) was used in all 270 patients, transrectal ultrasound (TRUS) in 121 patients, and rectal magnetic resonance imaging (MRI) in 65 patients. Findings according to imaging modalities were correlated with pathologic stage using Cohen's kappa (κ) to test agreement and intra-class correlation coefficient α to test reliability.
RESULTS
Accuracy for prediction of ypT stage according to three imaging modalities was 45.2% (κ=0.136, α=0.380) in APCT, 49.2% (κ=0.259, α=0.514) in rectal MRI, and 57.9% (κ=0.266, α=0.520) in TRUS. Accuracy for prediction of ypN stage was 66.0% (κ=0.274, α=0.441) in APCT, 71.8% (κ=0.401, α=0.549) in rectal MRI, and 66.1% (κ=0.147, α=0.272) in TRUS. Of 270 patients, 37 (13.7%) were diagnosed as pathologic complete responder after nCRT. Rectal MRI for restaging did not predict complete response. On the other hand, TRUS did predict three complete responders (κ=0.238, α=0.401).
CONCLUSION
APCT, rectal MRI, and TRUS are unreliable in restaging rectal cancer after nCRT. We think that multimodal assessment with rectal MRI and TRUS may be the best option for local restaging of locally advanced rectal cancer after nCRT.
MeSH Terms
Figure
-
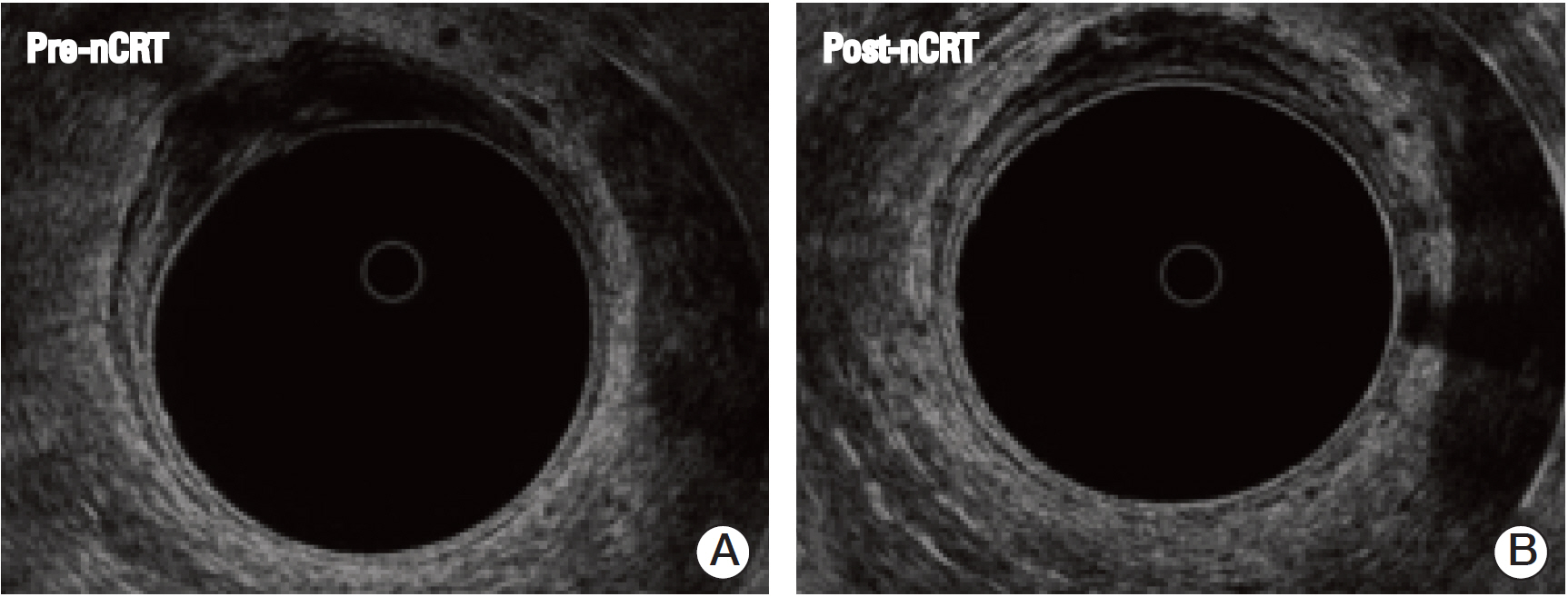
Fig. 1. A clinical complete response of the primary lesion after neoadjuvant chemoradiation therapy (nCRT) was defined when the primary lesion after nCRT was homogenous hypoechoic, reduced in size, had an intact whole rectal wall structure (B), especially hyper-echoic submucosal line, which was destructed before nCRT (A), and did not infiltrate to perirectal tissue.
Reference
-
References
1. Sauer R, Becker H, Hohenberger W, Rodel C, Wittekind C, Fietkau R, et al. Preoperative versus postoperative chemoradiotherapy for rectal cancer. N Engl J Med. 2004; 351:1731–40.
Article2. Kapiteijn E, Marijnen CA, Nagtegaal ID, Putter H, Steup WH, Wiggers T, et al. Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer. N Engl J Med. 2001; 345:638–46.
Article3. Theodoropoulos G, Wise WE, Padmanabhan A, Kerner BA, Taylor CW, Aguilar PS, et al. T-level downstaging and complete pathologic response after preoperative chemoradiation for advanced rectal cancer result in decreased recurrence and improved disease-free survival. Dis Colon Rectum. 2002; 45:895–903.
Article4. Van Cutsem E, Dicato M, Haustermans K, Arber N, Bosset JF, Cunningham D, et al. The diagnosis and management of rectal cancer: expert discussion and recommendations derived from the 9th World Congress on Gastrointestinal Cancer, Barcelona, 2007. Ann Oncol. 2008; 19 Suppl 6:vi1–8.
Article5. Kim CJ, Yeatman TJ, Coppola D, Trotti A, Williams B, Barthel JS, et al. Local excision of T2 and T3 rectal cancers after downstaging chemoradiation. Ann Surg. 2001; 234:352–8.
Article6. Kennelly RP, Heeney A, White A, Fennelly D, Sheahan K, Hyland JM, et al. A prospective analysis of patient outcome following treatment of T3 rectal cancer with neo-adjuvant chemoradiotherapy and transanal excision. Int J Colorectal Dis. 2012; 27:759–64.
Article7. Habr-Gama A, Perez RO, Nadalin W, Sabbaga J, Ribeiro U Jr, Silva e Sousa AH Jr, et al. Operative versus nonoperative treatment for stage 0 distal rectal cancer following chemoradiation therapy: long-term results. Ann Surg. 2004; 240:711–7.8. Martin ST, Heneghan HM, Winter DC. Systematic review and meta-analysis of outcomes following pathological complete response to neoadjuvant chemoradiotherapy for rectal cancer. Br J Surg. 2012; 99:918–28.
Article9. Smith FM, Waldron D, Winter DC. Rectum-conserving surgery in the era of chemoradiotherapy. Br J Surg. 2010; 97:1752–64.
Article10. Gannon CJ, Zager JS, Chang GJ, Feig BW, Wood CG, Skibber JM, et al. Pelvic exenteration affords safe and durable treatment for locally advanced rectal carcinoma. Ann Surg Oncol. 2007; 14:1870–7.
Article11. Dresen RC, Beets GL, Rutten HJ, Engelen SM, Lahaye MJ, Vliegen RF, et al. Locally advanced rectal cancer: MR imaging for restaging after neoadjuvant radiation therapy with concomitant chemotherapy. Part I. Are we able to predict tumor confined to the rectal wall? Radiology. 2009; 252:71–80.
Article12. Barbaro B, Vitale R, Leccisotti L, Vecchio FM, Santoro L, Valentini V, et al. Restaging locally advanced rectal cancer with MR imaging after chemoradiation therapy. Radiographics. 2010; 30:699–716.
Article13. Pomerri F, Pucciarelli S, Maretto I, Zandona M, Del Bianco P, Amadio L, et al. Prospective assessment of imaging after preoperative chemoradiotherapy for rectal cancer. Surgery. 2011; 149:56–64.
Article14. Hanly AM, Ryan EM, Rogers AC, McNamara DA, Madoff RD, Winter DC, et al. Multicenter Evaluation of Rectal cancer ReImaging pOst Neoadjuvant (MERRION) therapy. Ann Surg. 2014; 259:723–7.
Article15. Barbaro B, Schulsinger A, Valentini V, Marano P, Rotman M. The accuracy of transrectal ultrasound in predicting the pathological stage of low-lying rectal cancer after preoperative chemoradiation therapy. Int J Radiat Oncol Biol Phys. 1999; 43:1043–7.
Article16. Huh JW, Park YA, Jung EJ, Lee KY, Sohn SK. Accuracy of endorectal ultrasonography and computed tomography for restaging rectal cancer after preoperative chemoradiation. J Am Coll Surg. 2008; 207:7–12.
Article17. Herzog U, von Flue M, Tondelli P, Schuppisser JP. How accurate is endorectal ultrasound in the preoperative staging of rectal cancer? Dis Colon Rectum. 1993; 36:127–34.
Article18. Garcia-Aguilar J, Pollack J, Lee SH, Hernandez de Anda E, Mellgren A, Wong WD, et al. Accuracy of endorectal ultrasonography in preoperative staging of rectal tumors. Dis Colon Rectum. 2002; 45:10–5.
Article19. Lin S, Luo G, Gao X, Shan H, Li Y, Zhang R, et al. Application of endoscopic sonography in preoperative staging of rectal cancer: six-year experience. J Ultrasound Med. 2011; 30:1051–7.20. Kim TH, Jeong SY, Choi DH, Kim DY, Jung KH, Moon SH, et al. Lateral lymph node metastasis is a major cause of locoregional recurrence in rectal cancer treated with preoperative chemoradiotherapy and curative resection. Ann Surg Oncol. 2008; 15:729–37.
Article21. Kim JH, Beets GL, Kim MJ, Kessels AG, Beets-Tan RG. High-resolution MR imaging for nodal staging in rectal cancer: are there any criteria in addition to the size? Eur J Radiol. 2004; 52:78–83.
Article22. MERCURY Study Group. Extramural depth of tumor invasion at thin-section MR in patients with rectal cancer: results of the MERCURY study. Radiology. 2007; 243:132–9.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Interpretation of Rectal MRI after Neoadjuvant Treatment in Patients with Rectal Cancer
- The pattern of bowel dysfunction in patients with rectal cancer following the multimodal treatment: anorectal manometric measurements at before and after chemoradiation therapy, and postoperative 1 year
- How to Achieve a Higher Pathologic Complete Response in Patients With Locally Advanced Rectal Cancer Who Receive Preoperative Chemoradiation Therapy
- The Effects of Preoperative Chemoradiation Therapy in Pectal Cancer
- Unveiling the profound advantages of total neoadjuvant therapy in rectal cancer: a trailblazing exploration
