Korean J Gastroenterol.
2019 Jun;73(6):365-369. 10.4166/kjg.2019.73.6.365.
Feasibility of Adopting the “Step-up Approach†in Managing Necrotizing Pancreatitis-induced Pancreatic-colonic Fistula
- Affiliations
-
- 1Division of Gastroenterology, Department of Internal Medicine, Biomedical Research Institute, Chonbuk National University Hospital, Jeonju, Korea. solee@jbnu.ac.kr
- KMID: 2454099
- DOI: http://doi.org/10.4166/kjg.2019.73.6.365
Abstract
- Managing acute pancreatitis is clinically challenging because of the generally poor patient condition, the variety of treatment options depending on the severity and complications, and the uncertainty of outcomes. Recently, the step-up approach, which involves less invasive initial treatment and more invasive subsequent treatment, where necessary, has been proposed as the mainstay of managing pancreatitis. This paper presents a case of a 57-year-old man with severe acute pancreatitis, who developed an unexpected fistula in the rectum, which was treated successfully using the step-up approach. In managing this case, the authors faced clinical challenges in determining the infection of necrotic tissue in the early phase of the disease, the optimal timing and method of drainage, and the fistula closure or repair technique. Successful management of this case using the step-up approach validated current recommendations and suggests that it is a reasonable treatment strategy for pancreatic-colonic fistulas. This case also highlights the importance of an awareness that pancreatitis-associated complications can develop in an unexpected manner.
Keyword
MeSH Terms
Figure
-

Fig. 1 Computed tomography (CT) scans of the patient. Initial CT scan reveals edematous change of the pancreatic head with acute peripancreatic fluid collection (A) extending to the pelvic cavity (B). Follow-up scan at day 20 shows a massive increase in necrotic collection and wall formation at the same level (C).
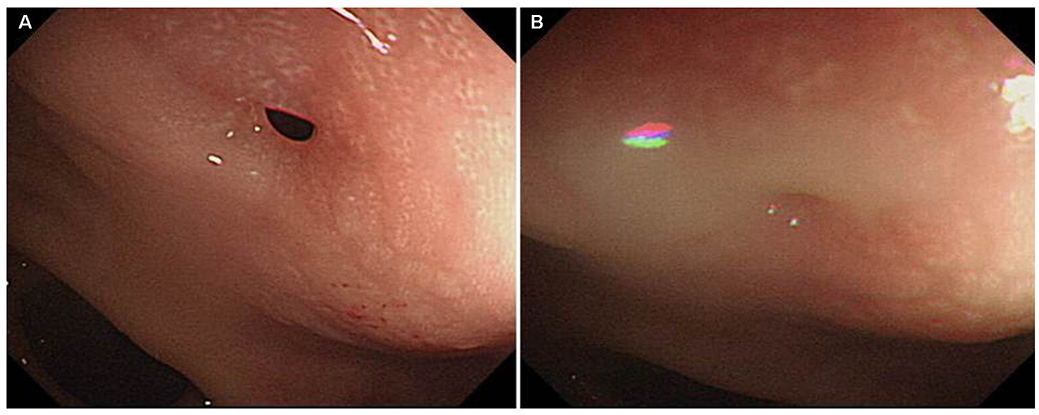
Fig. 2 Sigmoidoscopy image of the fistula opening. Sigmoidoscopy at day 25 reveals a fistula opening in the rectum (A) with pus discharge (B).
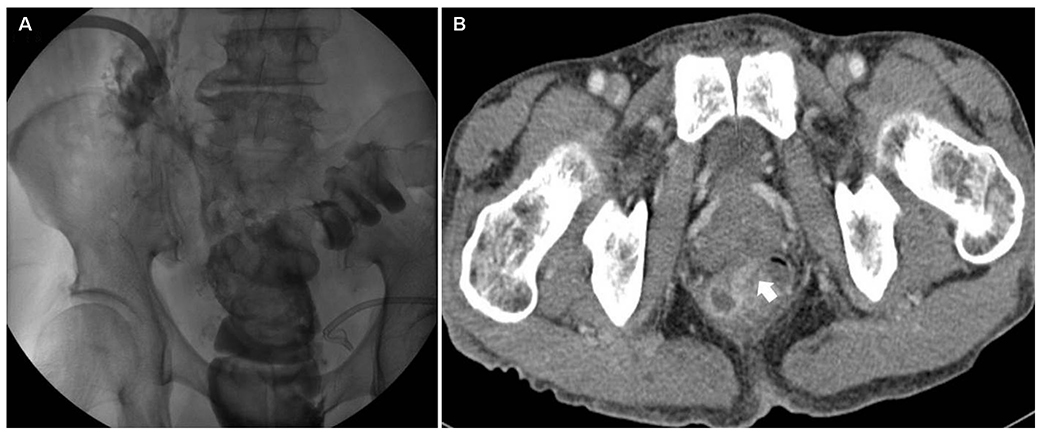
Fig. 3 Radiologic confirmation of the fistula tract. Contrast media filled rectum and sigmoid colon after contrast media injection to the percutaneous drainage tube (A) and computed tomography scan showing the fistula tract (B, white arrow).
Reference
-
1. Zerem E. Treatment of severe acute pancreatitis and its complications. World J Gastroenterol. 2014; 20:13879–13892.
Article2. Zerem E, Imamović G, Sušić A, Haračić B. Step-up approach to infected necrotising pancreatitis: a 20-year experience of percutaneous drainage in a single centre. Dig Liver Dis. 2011; 43:478–483.
Article3. van Santvoort HC, Besselink MG, Bakker OJ, et al. A step-up approach or open necrosectomy for necrotizing pancreatitis. N Engl J Med. 2010; 362:1491–1502.4. Working Group IAP/APA Acute Pancreatitis Guidelines. APA Acute Pancreatitis Guidelines. IAP/APA evidence-based guidelines for the management of acute pancreatitis. Pancreatology. 2013; 13:4 Suppl 2. e1–e15.5. Gerzof SG, Banks PA, Robbins AH, et al. Early diagnosis of pancreatic infection by computed tomography-guided aspiration. Gastroenterology. 1987; 93:1315–1320.
Article6. Banks PA, Bollen TL, Dervenis C, et al. Classification of acute pancreatitis--2012: revision of the Atlanta classification and definitions by international consensus. Gut. 2013; 62:102–111.
Article7. Oana S, Shibata S, Matsumoto T. Pancreatico-colonic fistula after endoscopic ultrasound-guided cyst drainage for pancreatic pseudocyst: report of three cases. JOP. 2016; 17:334–339.8. Will U, Meyer F, Hartmeier S, Schramm H, Bosseckert H. Endoscopic treatment of a pseudocystocolonic fistula by band ligation and endoloop application: case report. Gastrointest Endosc. 2004; 59:581–583.
Article9. Karvonen J, Gullichsen R, Salminen P, Grönroos JM. Endoscopic treatment of pseudocystocolonic fistula with fibrin glue. Gastrointest Endosc. 2010; 72:664–665.
Article10. Wille-Jørgensen P, Frederiksen HJ. Colonic necrosis or fistula following pancreatitis or gastric surgery. Eur J Surg. 1991; 157:137–139.11. Suzuki A, Suzuki S, Sakaguchi T, et al. Colonic fistula associated with severe acute pancreatitis: report of two cases. Surg Today. 2008; 38:178–183.
Article12. Shatney CH, Sosin H. Spontaneous perforation of a pancreatic pseudocyst into the colon and duodenum. Am J Surg. 1973; 126:433–438.
Article13. Clements JL Jr, Bradley EL 3rd, Eaton SB Jr. Spontaneous internal drainage of pancreatic pseudocysts. AJR Am J Roentgenol. 1976; 126:985–991.
Article14. Jiang W, Tong Z, Yang D, et al. Gastrointestinal fistulas in acute pancreatitis with infected pancreatic or peripancreatic necrosis: a 4-year single-center experience. Medicine (Baltimore). 2016; 95:e3318.15. Kwon JC, Kim BY, Kim AL, et al. Pancreatic pseudocystocolonic fistula treated without surgical or endoscopic intervention. World J Gastroenterol. 2014; 20:1882–1886.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of gastric and colonic fistulas with pancreatic and peripancreatic abscess after acute necrotizing pancreatitis
- A Case of a Pancreaticogastric Fistula Following Acute Pancreatitis
- Pancreatic Pseudocyst-Portal Vein Fistula: Serial Imaging and Clinical Follow-up from Pseudocyst to Fistula
- Two Cases of Colonic Obstruction after Acute Pancreatitis
- A Case of Colonic Perforation after Acute Necrotizing Pancreatitis
