Clinical Experience with the Bentall Procedure: 28 Years
- Affiliations
-
- 1Department of Thoracic and Cardiovascular Surgery, Yonsei Cardiovascular Center, Yonsei University College of Medicine, Seoul, Korea. sak911@yuhs.ac
Abstract
- PURPOSE
We retrospectively analyzed 28 years of experience with the Bentall procedure in patients with aortic valve, aortic root, and ascending aortic disease.
MATERIALS AND METHODS
Between March 1982 and December 2010, a total of 218 patients underwent the Bentall procedure using a composite valved conduit. The "inclusion technique" was used in 30 patients (13.8%), the "open-button technique" in 181 patients (83.0%), and the Cabrol technique in 7 patients (3.2%).
RESULTS
The early mortality rate was 5.5% (12/218). The mean follow-up duration was 108.0+/-81.0 months (range: 1-329 months). Seven patients required re-operation, and 1 patient required stent graft insertion at the descending thoracic aorta for progression of aortic arch or descending thoracic aortic dissection or aneurysm after the first operation, and 5 of them had Marfan syndrome. Kaplan-Meier estimated survival rates at 1, 5, 10, 20, and 25 years were 90.4%, 82.7%, 77.6%, 65.3%, and 60.3%, respectively. Freedom from reoperation rates at 1, 5, 10, 20, and 25 years were 99.0%, 98.3%, 95.5%, 90.8%, and 90.8%, respectively.
CONCLUSION
In our experience, the Bentall procedure provided optimal survival with improved functional status. The disease of the aorta may progress, especially in patients with Marfan syndrome. Therefore, careful follow-up with regular computed tomography angiograms should be performed in these patients.
MeSH Terms
Figure
-
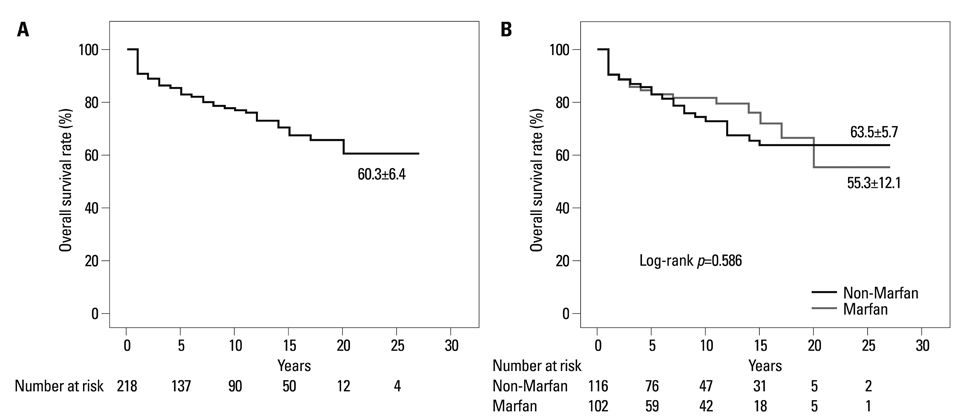
Fig. 1 Kaplan-Meier estimated survival curves. Actual survival of all patients, at a mean follow-up time of 108.0±81.0 months, following the Bentall procedure (A). Actual survival of Marfan and non-Marfan syndrome patients (B).
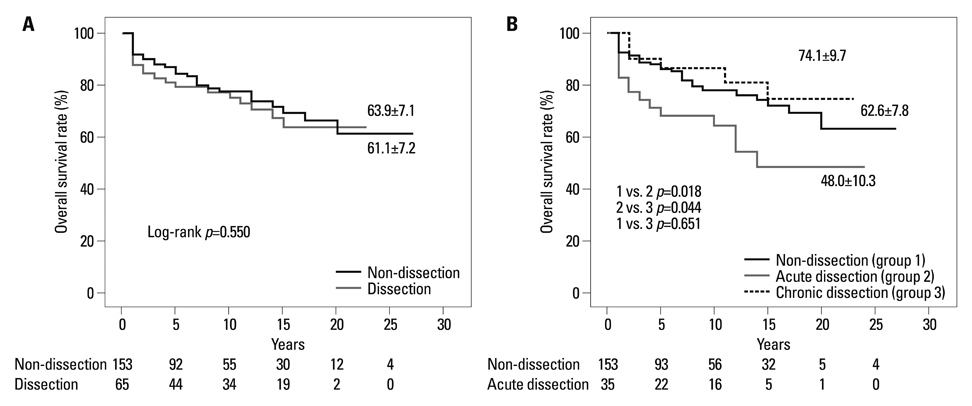
Fig. 2 Kaplan-Meier estimated survival curves. Actual survival rate for non-dissection and dissection patients (A). Actual survival of non-dissection (group 1), acute dissection (group 2) and chronic dissection (group 3) patients (B).

Fig. 3 Kaplan-Meier estimated survival curves. Actual survival rate according to coronary transfer technique. Inclusion (group 1), open-button (group 2), Cabrol (group 3).
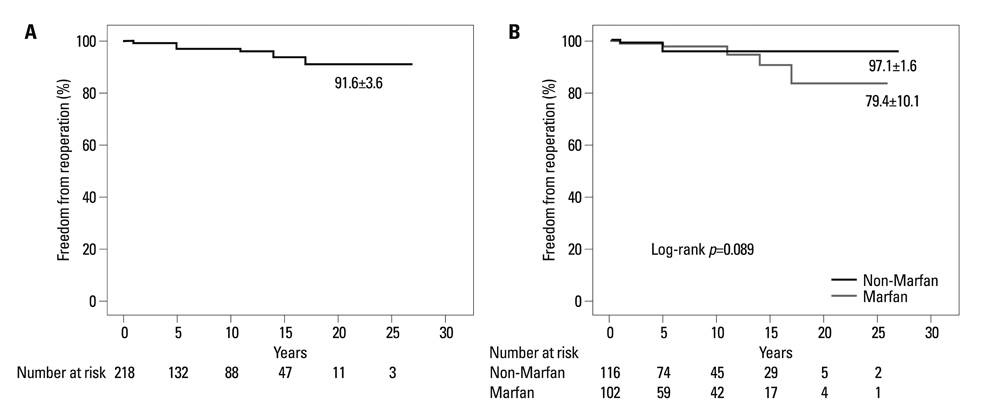
Fig. 4 Kaplan-Meier estimated freedom from reoperation. Freedom from reoperation for all patients, at a mean follow-up time of 100 months, following the Bentall procedure (A). Freedom from reoperation for Marfan versus non-Marfan syndrome patients (B).
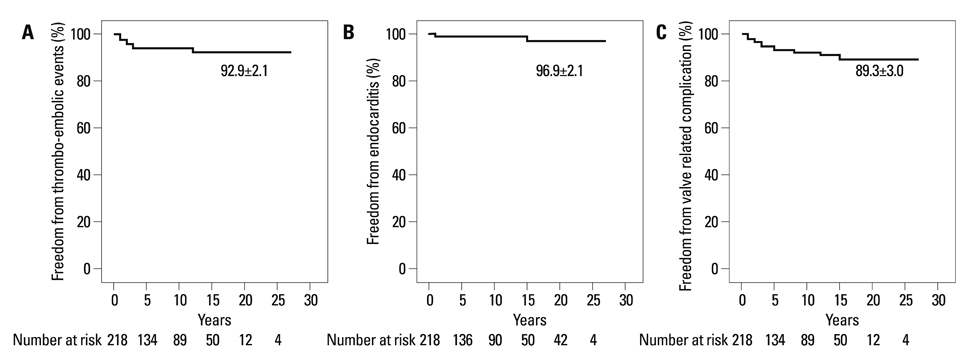
Fig. 5 Kaplan-Meier estimated freedom from prosthetic valve related complications. Kaplan-Meier estimated freedom from anti-coagulation-related complications (A), endocarditis-related complications (B), and valve-related complications (C).
Reference
-
1. Bentall H, De Bono A. A technique for complete replacement of the ascending aorta. Thorax. 1968. 23:338–339.
Article2. Kouchoukos NT, Wareing TH, Murphy SF, Perrillo JB. Sixteen-year experience with aortic root replacement. Results of 172 operations. Ann Surg. 1991. 214:308–318.3. Svensson LG, Crawford ES, Hess KR, Coselli JS, Safi HJ. Composite valve graft replacement of the proximal aorta: comparison of techniques in 348 patients. Ann Thorac Surg. 1992. 54:427–437.
Article4. Pacini D, Ranocchi F, Angeli E, Settepani F, Pagliaro M, Martin-Suarez S, et al. Aortic root replacement with composite valve graft. Ann Thorac Surg. 2003. 76:90–98.
Article5. Hagl C, Strauch JT, Spielvogel D, Galla JD, Lansman SL, Squitieri R, et al. Is the Bentall procedure for ascending aorta or aortic valve replacement the best approach for long-term event-free survival? Ann Thorac Surg. 2003. 76:698–703.
Article6. Sarsam MA, Yacoub M. Remodeling of the aortic valve anulus. J Thorac Cardiovasc Surg. 1993. 105:435–438.
Article7. David TE, Feindel CM, Bos J. Repair of the aortic valve in patients with aortic insufficiency and aortic root aneurysm. J Thorac Cardiovasc Surg. 1995. 109:345–351.
Article8. David TE, Armstrong S, Ivanov J, Feindel CM, Omran A, Webb G. Results of aortic valve-sparing operations. J Thorac Cardiovasc Surg. 2001. 122:39–46.
Article9. Kazui T, Tsuboi J, Izumoto H, Nakajima T, Ishihara K, Kawazoe K. Aortic root remodeling with aortic annuloplasty: mid-term results. Circ J. 2007. 71:207–210.
Article10. Kouchoukos NT, Marshall WG Jr, Wedige-Stecher TA. Eleven-year experience with composite graft replacement of the ascending aorta and aortic valve. J Thorac Cardiovasc Surg. 1986. 92:691–705.
Article11. Milano AD, Pratali S, Mecozzi G, Boraschi P, Braccini G, Magagnini E, et al. Fate of coronary ostial anastomoses after the modified Bentall procedure. Ann Thorac Surg. 2003. 75:1797–1801.
Article12. Mautner SL, Mautner GC, Curry CL, Roberts WC. Massive perigraft aortic aneurysm late after composite graft replacement of the ascending aorta and aortic valve in the Marfan syndrome. Am J Cardiol. 1993. 71:624–627.
Article13. Kazui T, Yamashita K, Terada H, Washiyama N, Suzuki T, Ohkura K, et al. Late reoperation for proximal aortic and arch complications after previous composite graft replacement in Marfan patients. Ann Thorac Surg. 2003. 76:1203–1207.
Article14. Shiono M, Hata M, Sezai A, Iida M, Negishi N, Sezai Y. Reoperation for ascending aortic aneurysm, coronary ostial aneurysm and patent Cabrol trick after bentall operation for aortitis syndrome. Circ J. 2005. 69:861–864.
Article15. Donaldson RM, Ross DN. Composite graft replacement for the treatment of aneurysms of the ascending aorta associated with aortic valvular disease. Circulation. 1982. 66(2 Pt 2):I116–I121.16. Mayer JE Jr, Lindsay WG, Wang Y, Jorgensen CR, Nicoloff DM. Composite replacement of the aortic valve and ascending aorta. J Thorac Cardiovasc Surg. 1978. 76:816–823.
Article17. McCready RA, Pluth JR. Surgical treatment of ascending aortic aneurysms associated with aortic valve insufficiency. Ann Thorac Surg. 1979. 28:307–316.
Article18. Sioris T, David TE, Ivanov J, Armstrong S, Feindel CM. Clinical outcomes after separate and composite replacement of the aortic valve and ascending aorta. J Thorac Cardiovasc Surg. 2004. 128:260–265.
Article19. Prifti E, Bonacchi M, Frati G, Proietti P, Giunti G, Babatasi G, et al. Early and long-term outcome in patients undergoing aortic root replacement with composite graft according to the Bentall's technique. Eur J Cardiothorac Surg. 2002. 21:15–21.
Article20. Sheick-Yousif B, Sheinfield A, Tager S, Ghosh P, Priesman S, Smolinsky AK, et al. Aortic root surgery in Marfan syndrome. Isr Med Assoc J. 2008. 10:189–193.21. Crawford ES. Marfan's syndrome. Broad spectral surgical treatment cardiovascular manifestations. Ann Surg. 1983. 198:487–505.22. Kindo M, Billaud P, Gerelli S, Levy F, Mazzucotelli JP, Eisenmann B. Twenty-seven-year experience with composite valve graft replacement of the aortic root. J Heart Valve Dis. 2007. 16:370–377.23. Bachet J, Termignon JL, Goudot B, Dreyfus G, Piquois A, Brodaty D, et al. Aortic root replacement with a composite graft. Factors influencing immediate and long-term results. Eur J Cardiothorac Surg. 1996. 10:207–213.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Erratum to “Clinical Experience with the Bentall Procedure: 28 Years†by Joo HC, et al. (Yonsei Med J 2012;53:915-23.)
- Surgical Management of Aortic Root Dilatation with Advanced Aortic Regurgitation: Bentall Operation versus Valve-sparing Procedure
- Surgical Repair of Left Coronary Artery Pseudoaneurysm 10 Years after a Bentall's Procudure
- Modified Bentall Operation and the Double Sewing Ring Technique: 2 case reports
- Reoperation of Bentall Procedure Using Remote Access Perfusion (RAP) Catheter: A case report
