Primary central nervous system lymphoma with intramedullary spinal cord involvement mimicking inflammatory demyelinating disease
- Affiliations
-
- 1Department of Neurology, Chonnam National University Hospital, Chonnam National University Medical School, Gwangju, Republic of Korea. nts0022@hanmail.net
- 2Department of Neurology, Massachusetts General Hospital, Harvard Medical School, Boston, MA, USA. mlevy11@mgh.harvard.edu
- 3Department of Pathology, Chonnam National University Medical School, Gwangju, Republic of Korea.
- 4Department of Nuclear Medicine, Chonnam National University Hospital, Chonnam National University Medical School, Gwangju, Republic of Korea.
- 5Department of Radiology, Chonnam National University Hospital, Chonnam National University Medical School, Gwangju, Republic of Korea.
- KMID: 2452828
- DOI: http://doi.org/10.18700/jnc.190083
Abstract
- BACKGROUND
Spinal cord involvement of primary central nervous system lymphoma (PCNSL) is rare in a young immunocompetent patient and can be misdiagnosed as an inflammatory demyelinating disease (IDD) of the central nervous system.
CASE REPORT
We report a case of PCNSL mimicking IDD in a previously healthy 46-year-old man with weakness in both hands for 1 week. Magnetic resonance imaging (MRI) of the cervical spinal cord revealed contrast-enhancing intraparenchymal and leptomeningeal lesions in the cervical spinal cord and medulla oblongata. Cerebrospinal fluid analysis revealed pleocytosis (37/mm³). The patient's symptoms and lesions improved with corticosteroid treatment. However, he developed semicomatose mentality 5 months later. Brain MRI, ventricular biopsy, and ¹â¸F -flurodeoxyglucose positron emission tomography/computed tomography confirmed PCNSL. The patient deceased 3 months later, despite high-dose methotrexate chemotherapy.
CONCLUSION
Persistent gadolinium-enhancing MRI lesions along the ventricular regions and spinal leptomeninges could differentiate PCNSL involving the spinal cord from IDD in the early stages of the disease.
Keyword
MeSH Terms
Figure
-
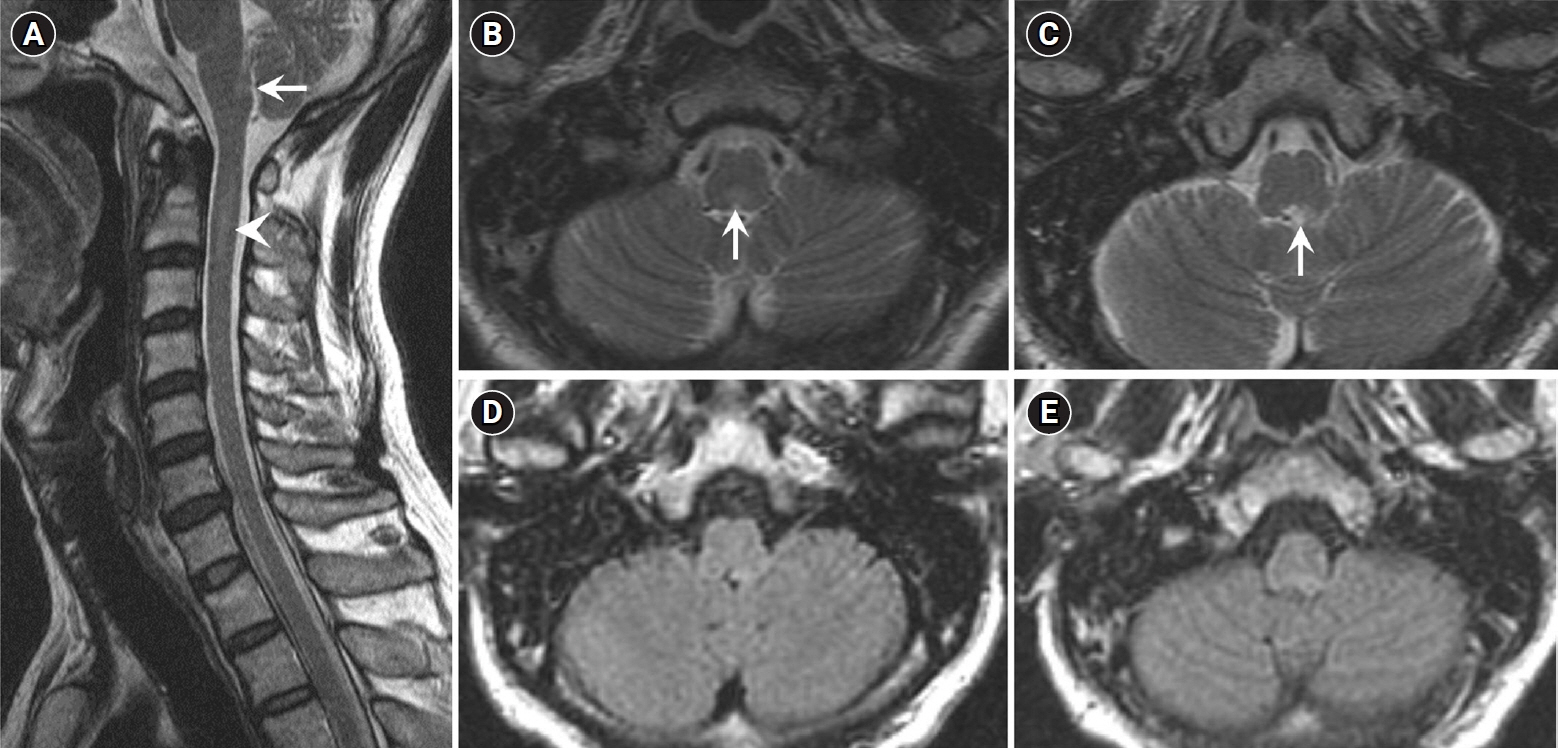
Fig. 1. Initial magnetic resonance imaging (MRI) of the brain and spinal cord 1 week after onset of symptoms. (A) Sagittal and (B, C) axial T2-weighted images show faint hyperintense multifocal lesions in the medulla oblongata (arrows) and cervical spinal cord (arrowhead). (D, E) High signal intensity in the medulla oblongata on T2-weighted images are not clearly detected on fluid-attenuated inversion recovery. No supratentorial or periventricular white matter lesion was seen on brain MRI (images not shown).

Fig. 2. Cervical spinal cord magnetic resonance imaging 3 weeks after the onset of symptoms. (A) Sagittal and (B, C) axial T2-weighted images show hyperintense lesions in the medulla oblongata and cervical spinal cord. (D) Gadolinium-enhanced T1-weighted images show leptomeningeal enhancement (arrowheads) and an intraparenchymal tadpole-like signal change (arrows) connected to the leptomeninges at the levels of (E) the medulla oblongata and (F) C2 vertebral body.

Fig. 3. Follow-up cervical spinal cord magnetic resonance imaging 6 months after the onset of symptoms. T2-weighted images (A, C) show marked decrease in multifocal lesions with no parenchymal enhancement (B, D). Gadolinium-enhanced T1-weighted sagittal images show persistent leptomeningeal enhancement (B, arrowheads).

Fig. 4. Brain computed tomography (CT) at the onset of the semicomatose status. Brain CT shows subependymal hyperdense lesions in all ventricles, including the right lateral ventricle, with hydrocephalus (A), and edema in the periventricular white matter and cerebral peduncle (B).

Fig. 5. Brain magnetic resonance imaging (MRI) after ventricular brain biopsy. (A, B) Axial T2-weighted images show hyperintensities in the hypothalamus and periventricular white matter. (C, D) Gadolinium-enhanced MRI shows multifocal subependymal nodular enhancing lesions.

Fig. 6. Pathologic findings. Hematoxylin and eosin staining (A) reveals large atypical lymphocytes mixed with small mature lymphocytes. Tumor cells were positive for CD20 (B, B-cell marker), with the Ki-67 labeling index approaching 80% (C), but negative for CD3 (D, T-cell marker) on immunohistochemical analysis (original magnification, ×200).

Fig. 7. 18F-fluorodeoxyglucose (FDG)-positron emission tomography (PET) of the brain. 18F-FDG-PET shows abnormal FDG uptake in the right lateral ventricle (A, white arrow) and inferior 4th ventricle (C, black arrow). PET and coregistered PET/magnetic resonance fusion imaging shows asymmetric, mild hypermetabolic lesions along the body, atrium, and posterior horn of the right lateral ventricle with a maximum standardized uptake volume (SUVmax) of 4.4 (A, B), and moderate hypermetabolic lesions along the inferior 4th ventricle with an SUVmax of 5.6 (C, D).

Fig. 8. Brain magnetic resonance imaging (MRI) after high-dose methotrexate chemotherapy. (A, B) Axial T2-weighted images show complete resolution of the multifocal subependymal nodular lesions in the hypothalamus and ventricular regions. (C, D) Gadolinium-enhanced MRI shows diffuse pachymeningeal thickening with no leptomeningeal enhancement.
Reference
-
1. Grommes C, DeAngelis LM. Primary CNS lymphoma. J Clin Oncol. 2017; 35:2410–8.
Article2. Hochberg FH, Baehring JM, Hochberg EP. Primary CNS lymphoma. Nat Clin Pract Neurol. 2007; 3:24–35.
Article3. Sierra del Rio M, Rousseau A, Soussain C, Ricard D, Hoang-Xuan K. Primary CNS lymphoma in immunocompetent patients. Oncologist. 2009; 14:526–39.
Article4. Herrlinger U, Weller M, Küker W. Primary CNS lymphoma in the spinal cord: clinical manifestations may precede MRI detectability. Neuroradiology. 2002; 44:239–44.5. Flanagan EP, O'Neill BP, Porter AB, Lanzino G, Haberman TM, Keegan BM. Primary intramedullary spinal cord lymphoma. Neurology. 2011; 77:784–91.
Article6. Elavarasi A, Dash D, Warrier AR, Bhatia R, Kumar L, Jain D, et al. Spinal cord involvement in primary CNS lymphoma. J Clin Neurosci. 2018; 47:145–8.
Article7. DeAngelis LM. Primary central nervous system lymphoma imitates multiple sclerosis. J Neurooncol. 1990; 9:177–81.
Article8. Kim SM, Kim SJ, Lee HJ, Kuroda H, Palace J, Fujihara K. Differential diagnosis of neuromyelitis optica spectrum disorders. Ther Adv Neurol Disord. 2017; 10:265–89.
Article9. Scott BJ, Douglas VC, Tihan T, Rubenstein JL, Josephson SA. A systematic approach to the diagnosis of suspected central nervous system lymphoma. JAMA Neurol. 2013; 70:311–9.
Article10. Han CH, Batchelor TT. Primary central nervous system lymphoma. Continuum (Minneap Minn). 2017; 23(6, Neuro-oncology):1601–18.
Article11. Mohile NA, Deangelis LM, Abrey LE. The utility of body FDG PET in staging primary central nervous system lymphoma. Neuro Oncol. 2008; 10:223–8.
Article12. Chiavazza C, Pellerino A, Ferrio F, Cistaro A, Soffietti R, Rudà R. Primary CNS lymphomas: challenges in diagnosis and monitoring. Biomed Res Int. 2018; 2018:3606970.
Article13. Bromberg JE, Breems DA, Kraan J, Bikker G, van der Holt B, Smitt PS, et al. CSF flow cytometry greatly improves diagnostic accuracy in CNS hematologic malignancies. Neurology. 2007; 68:1674–9.
Article14. Cordone I, Masi S, Carosi M, Vidiri A, Marchesi F, Marino M, et al. Brain stereotactic biopsy flow cytometry for central nervous system lymphoma characterization: advantages and pitfalls. J Exp Clin Cancer Res. 2016; 35:128.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Disseminated Tuberculosis of Central Nervous System : Spinal Intramedullary and Intracranial Tuberculomas
- Primary central nervous system lymphoma in the brainstem and cervical spinal cord: a case report and literature review
- A Case of Spinal Cord Glioblastoma Multiforme with Intracranial Metastasis
- Spinal Cord Neurosarcoidosis after Cervical Compressive Myelopathy
- Primary Peripheral Gamma Delta T-Cell Lymphoma of the Central Nervous System: Report of a Case Involving the Intramedullary Spinal Cord and Presenting with Myelopathy
