Ann Dermatol.
2019 Aug;31(4):378-386. 10.5021/ad.2019.31.4.378.
Association between Homocysteine Levels and Psoriasis: A Meta-Analysis
- Affiliations
-
- 1Department of Dermatology, Soonchunhyang University Cheonan Hospital, Cheonan, Korea. dermsung@schmc.ac.kr
- 2Department of Dermatology, Soonchunhyang University Seoul Hospital, Seoul, Korea.
- 3Department of Dermatology, Soonchunhyang University Bucheon Hospital, Bucheon, Korea.
- 4Department of Preventive Medicine, Korea University College of Medicine, Seoul, Korea. moole02@naver.com
- KMID: 2451474
- DOI: http://doi.org/10.5021/ad.2019.31.4.378
Abstract
- BACKGROUND
Psoriasis is a multifactorial disease associated with an increased risk for metabolic syndrome and cardiovascular diseases. Elevated levels of homocysteine (Hcy) are a marker of cardiovascular risk. Several studies have evaluated the associations between psoriasis and Hcy levels; however, the results remain inconclusive.
OBJECTIVE
We performed a systematic review of the literature and a meta-analysis to better understand the relationship between psoriasis and Hcy.
METHODS
Five scientific databases (MEDLINE, Embase, Cochrane Library, Scopus, and Web of Science) were searched to identify relevant studies. A review of 307 publications identified 16 studies that directly assessed plasma levels of Hcy in psoriasis patients.
RESULTS
A total of 16 studies including 2,091 subjects were included in the meta-analysis. Hcy levels were significantly higher in psoriasis patients relative to healthy controls (weighted mean difference [WMD], 3.30; 95% confidence interval [CI], 1.58∼5.02; I²=82.1%). Subgroup analyses revealed that patients with higher mean psoriasis area severity index (PASI) scores (PASI>10) had significantly higher Hcy levels compared to healthy controls (WMD, 4.17; 95% CI, 1.18∼7.16; I²=88.3%), whereas patients with lower mean PASI scores (PASI ≤10) had not (WMD, 0.76; 95% CI, −1.84∼3.35; I²=72.2%).
CONCLUSION
This meta-analysis found that psoriasis patients, in particular those with PASI >10, had significantly higher Hcy levels compared to healthy controls. Further research is needed to determine the association between Hcy levels and psoriasis severity.
Keyword
Figure
-
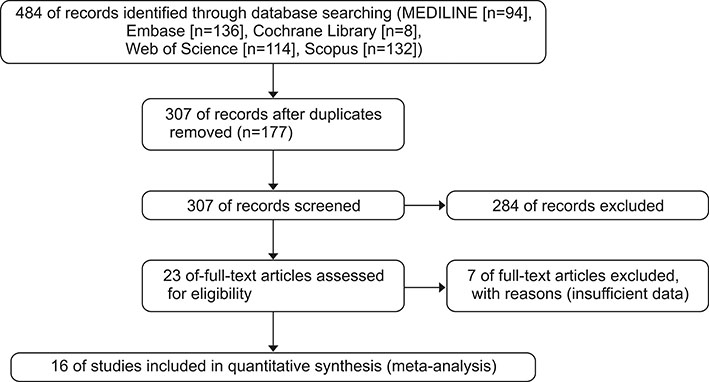
Fig. 1 Flow diagram of study identification, inclusion, and exclusion.
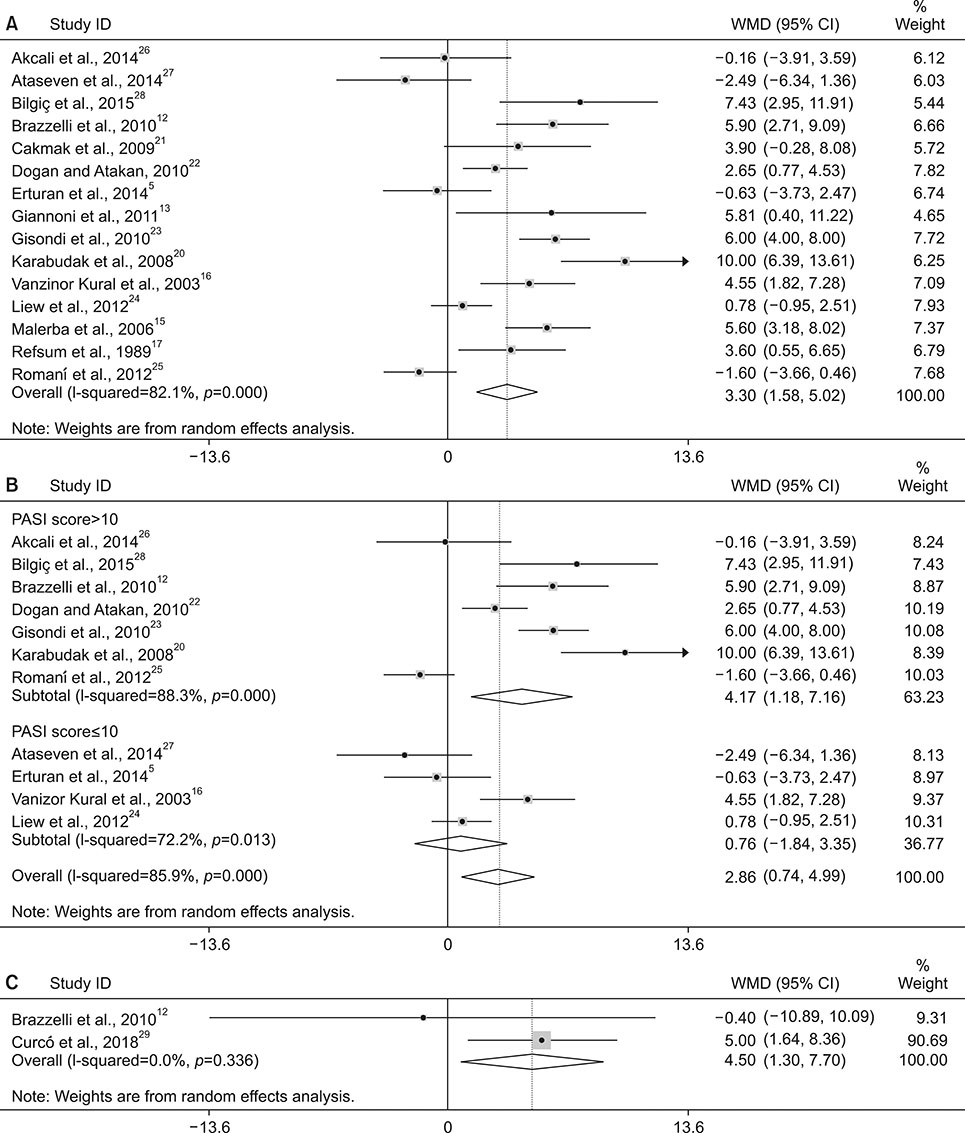
Fig. 2 Forest plot of the meta-analysis for homocysteine levels. (A) Homocysteine levels in psoriasis patients and controls. (B) Subgroup analysis according to mean psoriasis area severity index (PASI) scores. (C) Meta-analysis of two studies which directly compared homocysteine levels according to psoriasis severity within studies. WMD: weighted mean difference, CI: confidence interval.
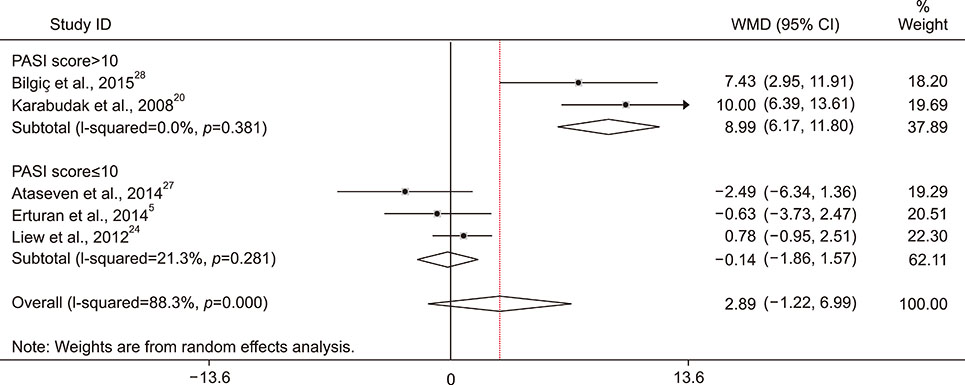
Fig. 3 Forest plot of the meta-analysis for sensitivity analysis. PASI: psoriasis area severity index, WMD: weighted mean difference, CI: confidence interval.
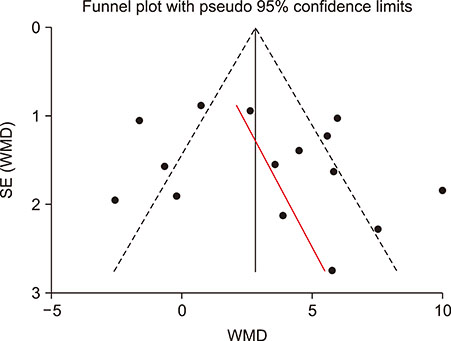
Fig. 4 Funnel plot of included studies. SE: standard error, WMD: weighted mean difference.
Reference
-
1. Neimann AL, Shin DB, Wang X, Margolis DJ, Troxel AB, Gelfand JM. Prevalence of cardiovascular risk factors in patients with psoriasis. J Am Acad Dermatol. 2006; 55:829–835.2. Arias-Santiago S, Orgaz-Molina J, Castellote-Caballero L, Arrabal-Polo MÁ, García-Rodriguez S, Perandrés-López R, et al. Atheroma plaque, metabolic syndrome and inflammation in patients with psoriasis. Eur J Dermatol. 2012; 22:337–344.
Article3. Vena GA, Altomare G, Ayala F, Berardesca E, Calzavara-Pinton P, Chimenti S, et al. Incidence of psoriasis and association with comorbidities in Italy: a 5-year observational study from a national primary care database. Eur J Dermatol. 2010; 20:593–598.4. Reich K. The concept of psoriasis as a systemic inflammation: implications for disease management. J Eur Acad Dermatol Venereol. 2012; 26:Suppl 2. 3–11.
Article5. Erturan I, Köroğlu BK, Adiloğlu A, Ceyhan AM, Akkaya VB, Tamer N, et al. Evaluation of serum sCD40L and homocysteine levels with subclinical atherosclerosis indicators in patients with psoriasis: a pilot study. Int J Dermatol. 2014; 53:503–509.
Article6. Ahlehoff O, Gislason GH, Charlot M, Jørgensen CH, Lindhardsen J, Olesen JB, et al. Psoriasis is associated with clinically significant cardiovascular risk: a Danish nationwide cohort study. J Intern Med. 2011; 270:147–157.
Article7. Hjuler KF, Gormsen LC, Vendelbo MH, Egeberg A, Nielsen J, Iversen L. Increased global arterial and subcutaneous adipose tissue inflammation in patients with moderate-to-severe psoriasis. Br J Dermatol. 2017; 176:732–740.
Article8. Dowlatshahi EA, van der Voort EA, Arends LR, Nijsten T. Markers of systemic inflammation in psoriasis: a systematic review and meta-analysis. Br J Dermatol. 2013; 169:266–282.
Article9. Davidovici BB, Sattar N, Prinz J, Puig L, Emery P, Barker JN, et al. Psoriasis and systemic inflammatory diseases: potential mechanistic links between skin disease and co-morbid conditions. J Invest Dermatol. 2010; 130:1785–1796.
Article10. Oussalah A, Guéant JL, Peyrin-Biroulet L. Meta-analysis: hyperhomocysteinaemia in inflammatory bowel diseases. Aliment Pharmacol Ther. 2011; 34:1173–1184.
Article11. Wang WM, Jin HZ. Homocysteine: a potential common route for cardiovascular risk and DNA methylation in psoriasis. Chin Med J (Engl). 2017; 130:1980–1986.12. Brazzelli V, Grasso V, Fornara L, Moggio E, Gamba G, Villani S, et al. Homocysteine, vitamin B12 and folic acid levels in psoriatic patients and correlation with disease severity. Int J Immunopathol Pharmacol. 2010; 23:911–916.
Article13. Giannoni M, Consales V, Campanati A, Ganzetti G, Giuliodori K, Postacchini V, et al. Homocysteine plasma levels in psoriasis patients: our experience and review of the literature. J Eur Acad Dermatol Venereol. 2015; 29:1781–1785.
Article14. Richetta AG, Mattozzi C, Macaluso L, Cantisani C, Giancristoforo S, D'epiro S, et al. Homocysteine plasmatic status in patients with psoriasis. Eur J Dermatol. 2011; 21:621–623.
Article15. Malerba M, Gisondi P, Radaeli A, Sala R, Calzavara Pinton PG, Girolomoni G. Plasma homocysteine and folate levels in patients with chronic plaque psoriasis. Br J Dermatol. 2006; 155:1165–1169.
Article16. Vanizor Kural B, Orem A, CimXMLLink_XYZit G, Uydu HA, Yandi YE, Alver A. Plasma homocysteine and its relationships with atherothrombotic markers in psoriatic patients. Clin Chim Acta. 2003; 332:23–30.
Article17. Refsum H, Helland S, Ueland PM. Fasting plasma homocysteine as a sensitive parameter of antifolate effect: a study of psoriasis patients receiving low-dose methotrexate treatment. Clin Pharmacol Ther. 1989; 46:510–520.
Article18. Tobin AM, Hughes R, Hand EB, Leong T, Graham IM, Kirby B. Homocysteine status and cardiovascular risk factors in patients with psoriasis: a case-control study. Clin Exp Dermatol. 2011; 36:19–23.
Article19. Moher D, Liberati A, Tetzlaff J, Altman DG. and the PRISMA Group. Preferred reporting items for systematic reviews and meta-analysis: the PRISMA Statment. Ann Intern Med. 2009; 151:264–269.
Article20. Karabudak O, Ulusoy RE, Erikci AA, Solmazgul E, Dogan B, Harmanyeri Y. Inflammation and hypercoagulable state in adult psoriatic men. Acta Derm Venereol. 2008; 88:337–340.21. Cakmak SK, Gül U, Kiliç C, Gönül M, Soylu S, Kiliç A. Homocysteine, vitamin B12 and folic acid levels in psoriasis patients. J Eur Acad Dermatol Venereol. 2009; 23:300–303.22. Dogan S, Atakan N. Is serum amyloid A protein a better indicator of inflammation in severe psoriasis? Br J Dermatol. 2010; 163:895–896.
Article23. Gisondi P, Malerba M, Malara G, Puglisi Guerra A, Sala R, Radaeli A, et al. C-reactive protein and markers for thrombophilia in patients with chronic plaque psoriasis. Int J Immunopathol Pharmacol. 2010; 23:1195–1202.
Article24. Liew SC, Das-Gupta E, Wong SF, Lee N, Safdar N, Jamil A. Association of methylentetraydrofolate reductase (MTHFR) 677 C > T gene polymorphism and homocysteine levels in psoriasis vulgaris patients from Malaysia: a case-control study. Nutr J. 2012; 11:1.
Article25. Romaní J, Caixàs A, Carrascosa JM, Ribera M, Rigla M, Luelmo J. Effect of narrowband ultraviolet B therapy on inflammatory markers and body fat composition in moderate to severe psoriasis. Br J Dermatol. 2012; 166:1237–1244.
Article26. Akcali C, Buyukcelik B, Kirtak N, Inaloz S. Clinical and laboratory parameters associated with metabolic syndrome in Turkish patients with psoriasis. J Int Med Res. 2014; 42:386–394.
Article27. Ataseven A, Kesli R, Kurtipek GS, Ozturk P. Assessment of lipocalin 2, clusterin, soluble tumor necrosis factor receptor-1, interleukin-6, homocysteine, and uric acid levels in patients with psoriasis. Dis Markers. 2014; 2014:541709.
Article28. Bilgiç Ö, Altınyazar HC, Baran H, Ünlü A. Serum homocysteine, asymmetric dimethyl arginine (ADMA) and other arginine-NO pathway metabolite levels in patients with psoriasis. Arch Dermatol Res. 2015; 307:439–444.
Article29. Curcó N, Barriendos N, Barahona MJ, Arteaga C, García M, Yordanov S, et al. Factors influencing cardiometabolic risk profile in patients with psoriasis. Australas J Dermatol. 2018; 59:e93–e98.
Article30. Hayden JA, van der Windt DA, Cartwright JL, Côté P, Bombardier C. Assessing bias in studies of prognostic factors. Ann Intern Med. 2013; 158:280–286.
Article31. Lin X, Huang T. Oxidative stress in psoriasis and potential therapeutic use of antioxidants. Free Radic Res. 2016; 50:585–595.
Article32. Mansoor MA, Bergmark C, Svardal AM, Lønning PE, Ueland PM. Redox status and protein binding of plasma homocysteine and other aminothiols in patients with early-onset peripheral vascular disease. Homocysteine and peripheral vascular disease. Arterioscler Thromb Vasc Biol. 1995; 15:232–240.
Article33. Koutroubakis IE, Malliaraki N, Dimoulios PD, Karmiris K, Castanas E, Kouroumalis EA. Decreased total and corrected antioxidant capacity in patients with inflammatory bowel disease. Dig Dis Sci. 2004; 49:1433–1437.
Article34. Pearce DJ, Morrison AE, Higgins KB, Crane MM, Balkrishnan R, Fleischer AB Jr, et al. The comorbid state of psoriasis patients in a university dermatology practice. J Dermatolog Treat. 2005; 16:319–323.
Article35. McDonald CJ, Calabresi P. Thromboembolic disorders associated with psoriasis. Arch Dermatol. 1973; 107:918.
Article36. Lindegård B. Diseases associated with psoriasis in a general population of 159,200 middle-aged, urban, native Swedes. Dermatologica. 1986; 172:298–304.
Article37. Henseler T, Christophers E. Disease concomitance in psoriasis. J Am Acad Dermatol. 1995; 32:982–986.
Article38. Gelfand JM, Neimann AL, Shin DB, Wang X, Margolis DJ, Troxel AB. Risk of myocardial infarction in patients with psoriasis. JAMA. 2006; 296:1735–1741.
Article39. Ludwig RJ, Herzog C, Rostock A, Ochsendorf FR, Zollner TM, Thaci D, et al. Psoriasis: a possible risk factor for development of coronary artery calcification. Br J Dermatol. 2007; 156:271–276.
Article40. Kremers HM, McEvoy MT, Dann FJ, Gabriel SE. Heart disease in psoriasis. J Am Acad Dermatol. 2007; 57:347–354.
Article41. Graham IM, Daly LE, Refsum HM, Robinson K, Brattström LE, Ueland PM, et al. Plasma homocysteine as a risk factor for vascular disease. The European Concerted Action Project. JAMA. 1997; 277:1775–1781.
Article42. Mayer O, Filipovský J, Dolejsová M, Cífková R, Simon J, Bolek L. Mild hyperhomocysteinaemia is associated with increased aortic stiffness in general population. J Hum Hypertens. 2006; 20:267–271.
Article43. Hild DH. Folate losses from the skin in exfoliative dermatitis. Arch Intern Med. 1969; 123:51–57.
Article44. Fry L, Macdonald A, Almeyda J, Griffin CJ, Hoffbrand AV. The mechanism of folate deficiency in psoriasis. Br J Dermatol. 1971; 84:539–544.
Article45. Touraine R, Revuz J, Zittoun J, Jarret J, Tulliez M. Study of folate in psoriasis: blood levels, intestinal absorption and cutaneous loss. Br J Dermatol. 1973; 89:335–341.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Association of Metabolic Comorbidities with Pediatric Psoriasis: A Systematic Review and Meta-Analysis
- Association of Blood Homocysteine levels with Subclinical Atherosclerosis in Impaired Fasting Glucose
- Association of Homocysteine Levels With Blood Lead Levels and Micronutrients in the US General Population
- Association of Psoriasis with Serum Vitamin D and Lipid Levels: A Clinical Review of Korean Patients in a Single Tertiary Referral Center
- Serum Homocysteine and Folate Levels in Korean Schizophrenic Patients
