Technical Feasibility of a Guidetube for Various Endoscopic Procedures in Human Gastrointestinal Simulators
- Affiliations
-
- 1Department of Gastroenterology, SMG-SNU Boramae Medical Center, Seoul National University of College of Medicine, Seoul, Korea. kjwjor@snu.ac.kr
- 2Department of Internal Medicine, Seoul National University of College of Medicine, Seoul, Korea.
- KMID: 2449764
- DOI: http://doi.org/10.5946/ce.2018.147
Abstract
- BACKGROUND/AIMS
Many gastrointestinal (GI) endoscopic procedures are difficult and cumbersome owing to the limitation of currently available endoscopic devices. This study aimed to develop an endoscopic guidetube for multipurpose endoscopic procedures and assess its use in a realistic GI endoscopic simulator.
METHODS
The guidetube used is a soft overtube composed of neoprene and is designed to assist various endoscopic procedures on demand. In total, 15 types of procedures were performed in GI simulators. Four procedures were performed in the stomach model and 11 in the colon model. The procedures include repeated endoscopic insertion and foreign body removal in various positions. The mean insertion and procedure time were assessed in each session. All procedures were performed by 5 expert endoscopists.
RESULTS
Endoscopic procedures with the new guidetube were faster and more effective than the conventional endoscopic techniques. The mean insertion time of the endoscope with the guidetube was significantly shorter than that without the guidetube. The guidetube was safely inserted without scratch using low pushing force. Objects of various sizes larger than the endoscopic channel were easily removed by the guidetube-assisted endoscopic procedures.
CONCLUSIONS
This preliminary study shows that guidetube-assisted endoscopic procedures are faster, easier, safer and cheaper than conventional endoscopic procedures.
Figure
-
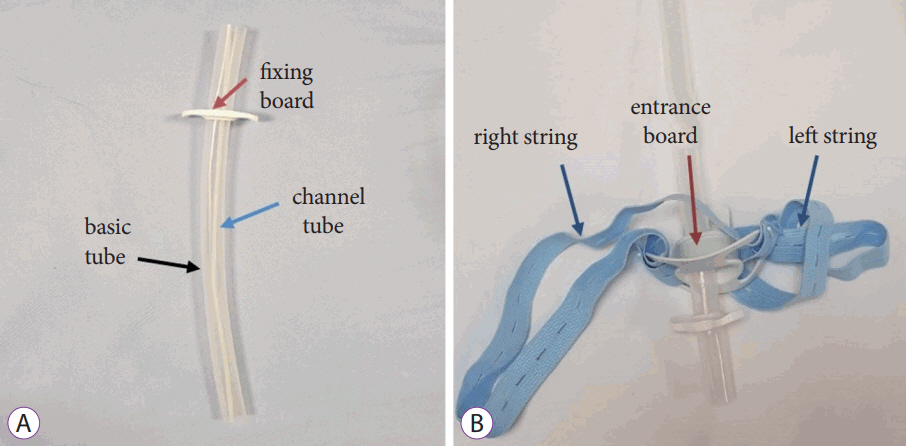
Fig. 1. This photo shows the guidetube for various endoscopic procedures. The guidetube system has 2 components, the guidetube and locking portion. (A) The guidetube is composed of a basic tube, channel tube, and fixing board. (B) The locking portion is composed of 2 strings and an entrance board. The guidetube is fixed through the entrance board. The 2 strings fasten the guidetube to the body.
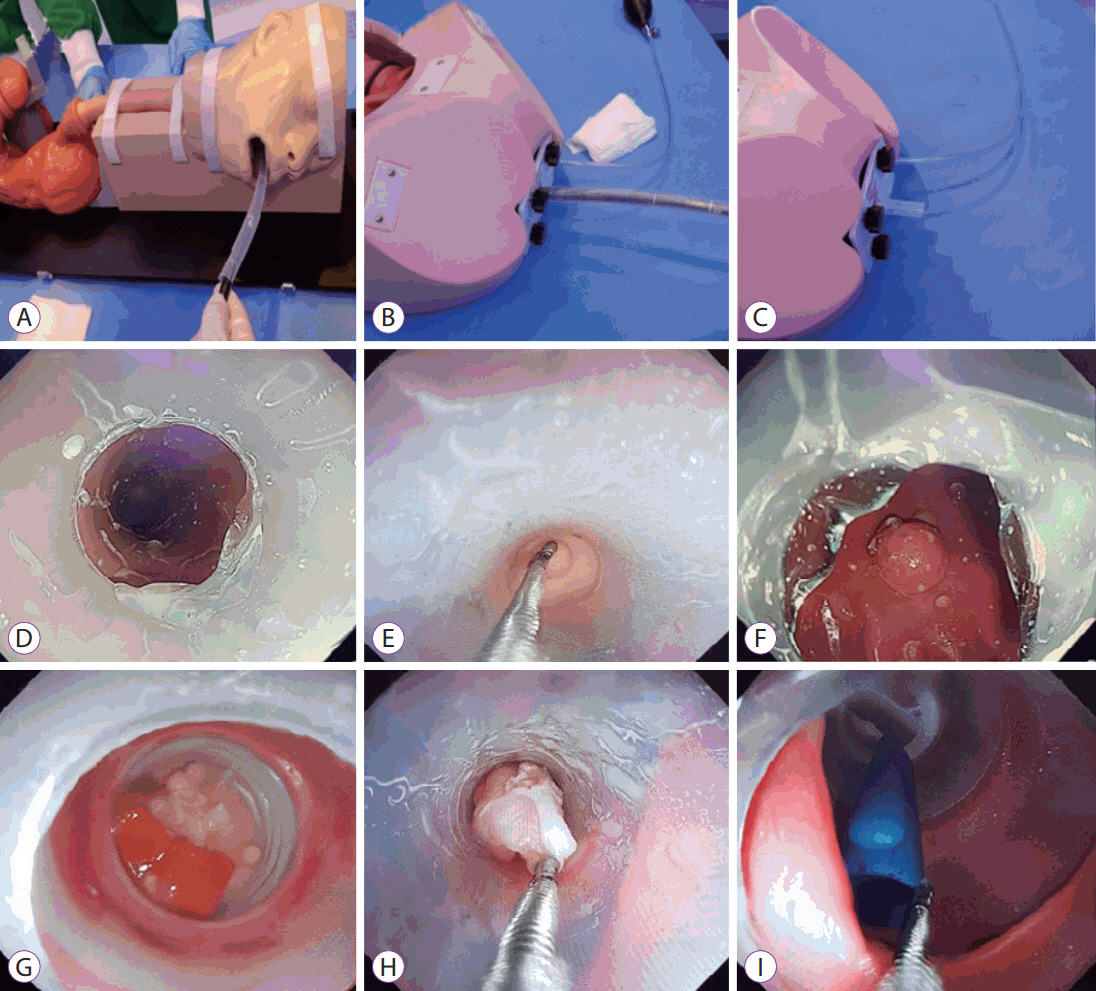
Fig. 2. Various endoscopic procedures using the guidetube. The guidetube is mounted on the conventional endoscope and inserted into the gastrointestinal lumen. After fixing the guidetube into the simulator entrance, the endoscope is removed. Examples of various materials removed using the new guidetube from the gastrointestinal tract. (A) An endoscope equipped with a guidetube is inserted into the stomach simulator. (B) An endoscope equipped with a guidetube is inserted into the colon simulator. (C) Only the guidetube is fixed in the colon. (D) The guidetube is mounted on the sigmoid colon. (E) Small polyps, (F) 1-cm polyps, (G) food material, (H) 2-cm polyp, and (I) foreign body (cap of pen).
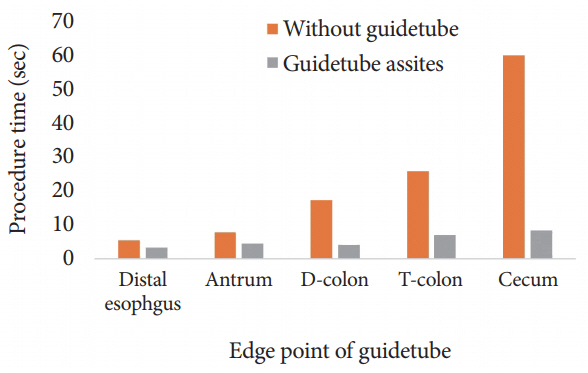
Fig. 3. Summarized results of the efficacy of repetitive endoscopic insertion. Endoscopic insertion using the guidetube was significantly efficient than conventional endoscopic insertion.
Cited by 1 articles
-
Usefulness of an Overtube Device in Gastrointestinal Endoscopy
Seung Han Kim
Clin Endosc. 2019;52(3):203-204. doi: 10.5946/ce.2019.085.
Reference
-
1. Birk M, Bauerfeind P, Deprez PH, et al. Removal of foreign bodies in the upper gastrointestinal tract in adults: European Society of Gastrointestinal Endoscopy (ESGE) clinical guideline. Endoscopy. 2016; 48:489–496.
Article2. Hong S, Suh M, Choi KS, et al. Guideline adherence to colonoscopic surveillance intervals after polypectomy in Korea: results from a nationwide survey. Gut Liver. 2018; 12:426–432.
Article3. Uraoka T, Saito Y, Matsuda T, et al. Endoscopic indications for endoscopic mucosal resection of laterally spreading tumours in the colorectum. Gut. 2006; 55:1592–1597.
Article4. Wedi E, Orlandini B, Gromski M, et al. Full-thickness resection device for complex colorectal lesions in high-risk patients as a last-resort endoscopic treatment: initial clinical experience and review of the current literature. Clin Endosc. 2018; 51:103–108.
Article5. Winawer SJ, Zauber AG, Ho MN, et al. Prevention of colorectal cancer by colonoscopic polypectomy. The National Polyp Study Workgroup. N Engl J Med. 1993; 329:1977–1981.6. Klein A, Bourke MJ. Advanced polypectomy and resection techniques. Gastrointest Endosc Clin N Am. 2015; 25:303–333.
Article7. Lee SP, Sung IK, Kim JH, Lee SY, Park HS, Shim CS. Risk factors for incomplete polyp resection during colonoscopic polypectomy. Gut Liver. 2015; 9:66–72.
Article8. Goldschmiedt M, Haber G, Kandel G, Kortan P, Marcon N. A safety maneuver for placing overtubes during endoscopic variceal ligation. Gastrointest Endosc. 1992; 38:399–400.
Article9. Hawari R, Pasricha PJ. Going for the loop: a unique overtube for the difficult colonoscopy. J Clin Gastroenterol. 2007; 41:138–140.10. Raju GS, Pasricha PJ. ShapeLock: a rapid access port for redeployment of a colonoscope into the proximal colon to facilitate multiple polypectomies in a single session. Gastrointest Endosc. 2005; 61:768–770.
Article11. Shin JS, Sheu BS, Lin XZ, Chen CY, Leow TC. Longitudinal linear-incised overtube for endoscopic removal of larger ingested foreign bodies. Gastrointest Endosc. 1995; 41:618.
Article12. ASGE Technology Committee, Tierney WM, Adler DG, et al. Overtube use in gastrointestinal endoscopy. Gastrointest Endosc. 2009; 70:828–834.13. Berkelhammer C, Madhav G, Lyon S, Roberts J. “Pinch” injury during overtube placement in upper endoscopy. Gastrointest Endosc. 1993; 39:186–188.
Article14. Dinning JP, Jaffe PE. Delayed presentation of esophageal perforation as a result of overtube placement. J Clin Gastroenterol. 1997; 24:250–252.
Article15. el-Newihi HM, Mihas AA. Esophageal perforation as a complication of endoscopic overtube insertion. Am J Gastroenterol. 1994; 89:953–954.16. Groenen MJ, Moreels TG, Orlent H, Haringsma J, Kuipers EJ. Acute pancreatitis after double-balloon enteroscopy: an old pathogenetic theory revisited as a result of using a new endoscopic tool. Endoscopy. 2006; 38:82–85.
Article17. Holderman WH, Etzkorn KP, Patel SA, Harig JM, Watkins JL. Endoscopic findings and overtube-related complications associated with esophageal variceal ligation. J Clin Gastroenterol. 1995; 21:91–94.
Article18. Jeffries MA, Scheiman JM. Overtube separation. Gastrointest Endosc. 1998; 47:435–436.19. Levy R, Kaur S, Uzer M. Separation of an overtube from the bite block during band ligation of esophageal varices. Gastrointest Endosc. 1997; 46:66–68.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Management of gastrointestinal tract perforations
- Endovascular hemostasis for endoscopic procedure-related gastrointestinal bleeding
- Endoscopic Treatment of Subepithelial Tumors
- Simulator-based training method in gastrointestinal endoscopy training and currently available simulators
- Pyloric Obstruction with Advanced Gastric Cancer: Stent vs. Bypass
