Pulmonary and Physical Rehabilitation in Critically Ill Patients
- Affiliations
-
- 1Department of Rehabilitation Medicine, Biomedical Research Institute, Pusan National University Hospital, Busan, Korea. drshinmj@gmail.com
- 2Department of Rehabilitation Medicine, Pusan National University School of Medicine, Busan, Korea.
- KMID: 2449375
- DOI: http://doi.org/10.4266/acc.2019.00444
Abstract
- Some patients admitted to the intensive care unit (ICU) because of an acute illness, complicated surgery, or multiple traumas develop muscle weakness affecting the limbs and respiratory muscles during acute care in the ICU. This condition is referred to as ICU-acquired weakness (ICUAW), and can be evoked by critical illness polyneuropathy (CIP), critical illness myopathy (CIM), or critical illness polyneuromyopathy (CIPNM). ICUAW is diagnosed using the Medical Research Council (MRC) sum score based on bedside manual muscle testing in cooperative patients. The MRC sum score is the sum of the strengths of the 12 regions on both sides of the upper and lower limbs. ICUAW is diagnosed when the MRC score is less than 48 points. However, some patients require electrodiagnostic studies, such as a nerve conduction study, electromyography, and direct muscle stimulation, to differentiate between CIP and CIM. Pulmonary rehabilitation in the ICU can be divided into modalities intended to remove retained airway secretions and exercise therapies intended to improve respiratory function. Physical rehabilitation, including early mobilization, positioning, and limb exercises, attenuates the weakness that occurs during critical care. To perform mobilization in mechanically ventilated patients, pretreatment by removing secretions is necessary. It is also important to increase the strength of respiratory muscles and to perform lung recruitment to improve mobilization in patients who are weaned from the ventilator. For these reasons, pulmonary rehabilitation is important in addition to physical therapy. Early recognition of CIP, CIM, and CIPNM and early rehabilitation in the ICU might improve patients' functional recovery and outcomes.
Keyword
MeSH Terms
-
Critical Care
Critical Illness*
Early Ambulation
Electromyography
Exercise
Exercise Therapy
Extremities
Humans
Intensive Care Units
Lower Extremity
Lung
Multiple Trauma
Muscle Weakness
Muscular Diseases
Neural Conduction
Physical Therapy Modalities
Polyneuropathies
Rehabilitation*
Respiratory Muscles
Ventilators, Mechanical
Figure
-

Figure 1. Assessment of muscle strength with a handgrip dynamometer (A) and handheld dynamometry (B).
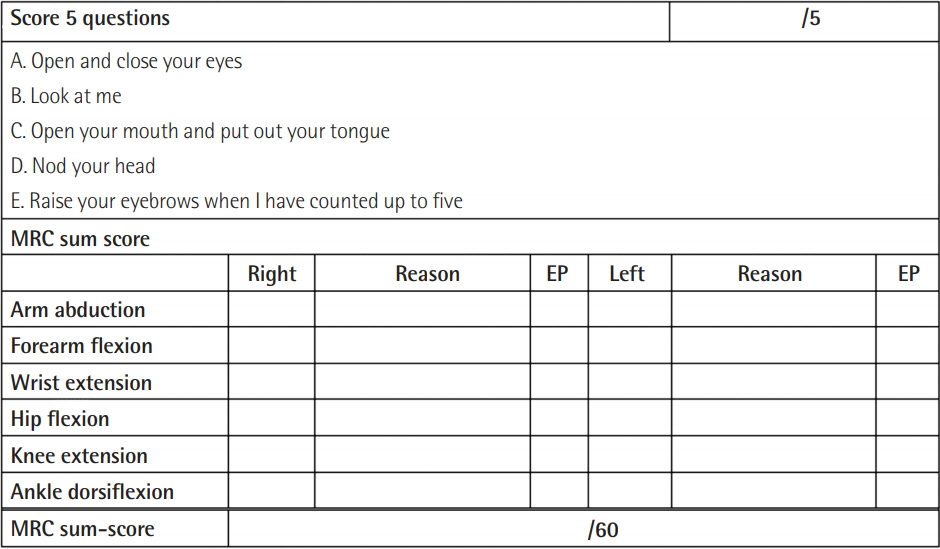
Figure 2. Sample sheet used for muscle strength testing through the Medical Research Council (MRC) sum score and the standardized 5 questions (S5Q) at Pusan National University Hospital. For values that are difficult to assess due to peripheral or central nervous lesions, amputation, or orthopedic reasons, the values of the same muscle group on the opposite side or in proximity on the ipsilateral side are extrapolated. EP: extrapolation.
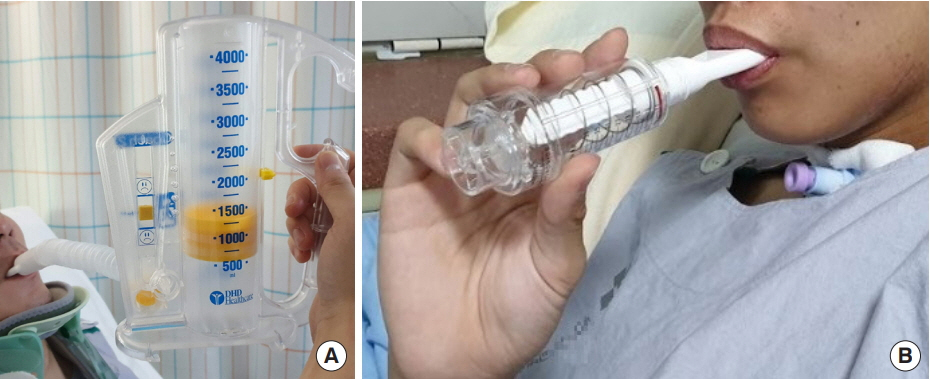
Figure 3. Incentive spirometry (A) and threshold inspiratory muscle training (B) for intensive care patients.

Figure 4. Treatment modalities for airway secretions. RFC: residual functional capacity; HFO: high frequency oscillation; IPV: intrapulmonary percussive ventilation; CPAP: continuous positive airway pressure; EPAP: expiratory positive airway pressure; PEP: positive expiratory pressure; NIV: noninvasive ventilation; MIE: mechanical insufflation-exsufflation.

Figure 5. Postural drainage with high-frequency oscillation (A) and the Acapella device (B) for secretion removal.
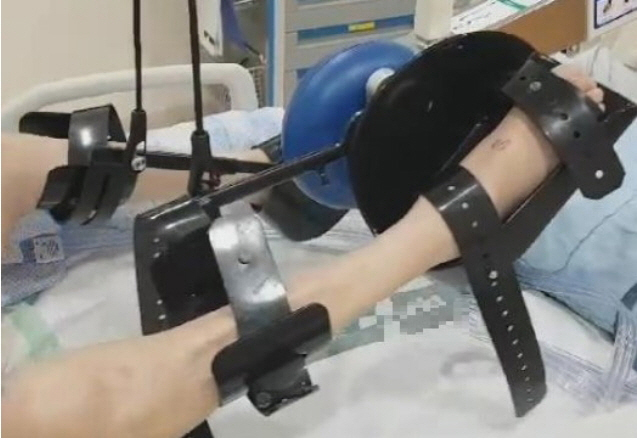
Figure 6. Cycle ergometer for active and passive cycling in the intensive care unit.

Figure 7. (A) Upper-body aerobic exercise with fitness equipment. (B, C) Resistive training of upper extremities and bridging exercise using elastic band.
Cited by 1 articles
-
Awakening in extracorporeal membrane oxygenation as a bridge to lung transplantation
Su Hwan Lee
Acute Crit Care. 2022;37(1):26-34. doi: 10.4266/acc.2022.00031.
Reference
-
1. Hashem MD, Parker AM, Needham DM. Early mobilization and rehabilitation of patients who are critically ill. Chest. 2016; 150:722–31.
Article2. Hermans G, Van den Berghe G. Clinical review: intensive care unit acquired weakness. Crit Care. 2015; 19:274.
Article3. Shepherd S, Batra A, Lerner DP. Review of critical illness myopathy and neuropathy. Neurohospitalist. 2017; 7:41–8.
Article4. De Jonghe B, Sharshar T, Lefaucheur JP, Authier FJ, Durand-Zaleski I, Boussarsar M, et al. Paresis acquired in the intensive care unit: a prospective multicenter study. JAMA. 2002; 288:2859–67.5. Linos K, Foot C, Ziegenfuss M, Freeman WD, Tan KM. Critical illness weakness: common questions. Curr Anaesth Crit Care. 2007; 18:252–60.
Article6. Latronico N, Bolton CF. Critical illness polyneuropathy and myopathy: a major cause of muscle weakness and paralysis. Lancet Neurol. 2011; 10:931–41.
Article7. Hermans G, De Jonghe B, Bruyninckx F, Van den Berghe G. Interventions for preventing critical illness polyneuropathy and critical illness myopathy. Cochrane Database Syst Rev. 2009; (1):CD006832.
Article8. Patel BK, Pohlman AS, Hall JB, Kress JP. Impact of early mobilization on glycemic control and ICU-acquired weakness in critically ill patients who are mechanically ventilated. Chest. 2014; 146:583–9.
Article9. Hermans G, Wilmer A, Meersseman W, Milants I, Wouters PJ, Bobbaers H, et al. Impact of intensive insulin therapy on neuromuscular complications and ventilator dependency in the medical intensive care unit. Am J Respir Crit Care Med. 2007; 175:480–9.
Article10. Shibahashi K, Sugiyama K, Kashiura M, Hamabe Y. Decreasing skeletal muscle as a risk factor for mortality in elderly patients with sepsis: a retrospective cohort study. J Intensive Care. 2017; 5:8.
Article11. Wallace JD, Calvo RY, Lewis PR, Brill JB, Shackford SR, Sise MJ, et al. Sarcopenia as a predictor of mortality in elderly blunt trauma patients: comparing the masseter to the psoas using computed tomography. J Trauma Acute Care Surg. 2017; 82:65–72.12. Looijaard WG, Dekker IM, Stapel SN, Girbes AR, Twisk JW, Oudemans-van Straaten HM, et al. Skeletal muscle quality as assessed by CT-derived skeletal muscle density is associated with 6-month mortality in mechanically ventilated critically ill patients. Crit Care. 2016; 20:386.
Article13. Paris M, Mourtzakis M. Assessment of skeletal muscle mass in critically ill patients: considerations for the utility of computed tomography imaging and ultrasonography. Curr Opin Clin Nutr Metab Care. 2016; 19:125–30.14. Vanpee G, Hermans G, Segers J, Gosselink R. Assessment of limb muscle strength in critically ill patients: a systematic review. Crit Care Med. 2014; 42:701–11.15. Vanpee G, Segers J, Van Mechelen H, Wouters P, Van den Berghe G, Hermans G, et al. The interobserver agreement of handheld dynamometry for muscle strength assessment in critically ill patients. Crit Care Med. 2011; 39:1929–34.
Article16. Tzanis G, Vasileiadis I, Zervakis D, Karatzanos E, Dimopoulos S, Pitsolis T, et al. Maximum inspiratory pressure, a surrogate parameter for the assessment of ICU-acquired weakness. BMC Anesthesiol. 2011; 11:14.
Article17. Gruther W, Benesch T, Zorn C, Paternostro-Sluga T, Quittan M, Fialka-Moser V, et al. Muscle wasting in intensive care patients: ultrasound observation of the M. quadriceps femoris muscle layer. J Rehabil Med. 2008; 40:185–9.
Article18. Witteveen E, Sommers J, Wieske L, Doorduin J, van Alfen N, Schultz MJ, et al. Diagnostic accuracy of quantitative neuromuscular ultrasound for the diagnosis of intensive care unitacquired weakness: a cross-sectional observational study. Ann Intensive Care. 2017; 7:40.
Article19. Parry SM, El-Ansary D, Cartwright MS, Sarwal A, Berney S, Koopman R, et al. Ultrasonography in the intensive care setting can be used to detect changes in the quality and quantity of muscle and is related to muscle strength and function. J Crit Care. 2015; 30:1151.
Article20. Looijaard WG, Molinger J, Weijs PJ. Measuring and monitoring lean body mass in critical illness. Curr Opin Crit Care. 2018; 24:241–7.
Article21. Kuchnia A, Earthman C, Teigen L, Cole A, Mourtzakis M, Paris M, et al. Evaluation of bioelectrical impedance analysis in critically ill patients: results of a multicenter prospective study. JPEN J Parenter Enteral Nutr. 2017; 41:1131–8.
Article22. Latronico N. Critical illness polyneuropathy and myopathy 20 years later. No man’s land? No, it is our land! Intensive Care Med. 2016; 42:1790–3.23. Moss M, Yang M, Macht M, Sottile P, Gray L, McNulty M, et al. Screening for critical illness polyneuromyopathy with single nerve conduction studies. Intensive Care Med. 2014; 40:683–90.
Article24. Latronico N, Nattino G, Guarneri B, Fagoni N, Amantini A, Bertolini G, et al. Validation of the peroneal nerve test to diagnose critical illness polyneuropathy and myopathy in the intensive care unit: the multicenter Italian CRIMYNE-2 diagnostic accuracy study. F1000Res. 2014; 3:127.25. Abrams D, Javidfar J, Farrand E, Mongero LB, Agerstrand CL, Ryan P, et al. Early mobilization of patients receiving extracorporeal membrane oxygenation: a retrospective cohort study. Crit Care. 2014; 18:R38.
Article26. Damluji A, Zanni JM, Mantheiy E, Colantuoni E, Kho ME, Needham DM. Safety and feasibility of femoral catheters during physical rehabilitation in the intensive care unit. J Crit Care. 2013; 28:535.
Article27. Brimioulle S, Moraine JJ, Norrenberg D, Kahn RJ. Effects of positioning and exercise on intracranial pressure in a neurosurgical intensive care unit. Phys Ther. 1997; 77:1682–9.
Article28. Nydahl P, Sricharoenchai T, Chandra S, Kundt FS, Huang M, Fischill M, et al. Safety of patient mobilization and rehabilitation in the intensive care unit: systematic review with metaanalysis. Ann Am Thorac Soc. 2017; 14:766–77.
Article29. Mendez-Tellez PA, Nusr R, Feldman D, Needham DM. Early physical rehabilitation in the ICU: a review for the neurohospitalist. Neurohospitalist. 2012; 2:96–105.
Article30. Devlin JW, Skrobik Y, Gélinas C, Needham DM, Slooter AJ, Pandharipande PP, et al. Clinical practice guidelines for the prevention and management of pain, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the ICU. Crit Care Med. 2018; 46:e825–73.31. Mendez-Tellez PA, Needham DM. Early physical rehabilitation in the ICU and ventilator liberation. Respir Care. 2012; 57:1663–9.
Article32. Burtin C, Clerckx B, Robbeets C, Ferdinande P, Langer D, Troosters T, et al. Early exercise in critically ill patients enhances short-term functional recovery. Crit Care Med. 2009; 37:2499–505.
Article33. Chiang LL, Wang LY, Wu CP, Wu HD, Wu YT. Effects of physical training on functional status in patients with prolonged mechanical ventilation. Phys Ther. 2006; 86:1271–81.
Article34. Tipping CJ, Harrold M, Holland A, Romero L, Nisbet T, Hodgson CL. The effects of active mobilisation and rehabilitation in ICU on mortality and function: a systematic review. Intensive Care Med. 2017; 43:171–83.
Article35. Cumming TB, Thrift AG, Collier JM, Churilov L, Dewey HM, Donnan GA, et al. Very early mobilization after stroke fast-tracks return to walking: further results from the phase II AVERT randomized controlled trial. Stroke. 2011; 42:153–8.
Article36. Gosselink R, Bott J, Johnson M, Dean E, Nava S, Norrenberg M, et al. Physiotherapy for adult patients with critical illness: recommendations of the European Respiratory Society and European Society of Intensive Care Medicine Task Force on physiotherapy for critically ill patients. Intensive Care Med. 2008; 34:1188–99.
Article37. Nyland BA, Spilman SK, Halub ME, Lamb KD, Jackson JA, Oetting TW, et al. A preventative respiratory protocol to identify trauma subjects at risk for respiratory compromise on a general in-patient ward. Respir Care. 2016; 61:1580–7.
Article38. Pathmanathan N, Beaumont N, Gratrix A. Respiratory physiotherapy in the critical care unit. BJA Educ. 2015; 15:20–5.
Article39. Bartlett RH, Gazzaniga AB, Geraghty TR. Respiratory maneuvers to prevent postoperative pulmonary complications: a critical review. JAMA. 1973; 224:1017–21.40. Moodie LH, Reeve JC, Vermeulen N, Elkins MR. Inspiratory muscle training to facilitate weaning from mechanical ventilation: protocol for a systematic review. BMC Res Notes. 2011; 4:283.
Article41. Levine S, Nguyen T, Taylor N, Friscia ME, Budak MT, Rothenberg P, et al. Rapid disuse atrophy of diaphragm fibers in mechanically ventilated humans. N Engl J Med. 2008; 358:1327–35.
Article42. Vorona S, Sabatini U, Al-Maqbali S, Bertoni M, Dres M, Bissett B, et al. Inspiratory muscle rehabilitation in critically ill adults: a systematic review and meta-analysis. Ann Am Thorac Soc. 2018; 15:735–44.
Article43. Bissett B, Leditschke IA, Green M, Marzano V, Collins S, Van Haren F. Inspiratory muscle training for intensive care patients: a multidisciplinary practical guide for clinicians. Aust Crit Care 2018 Jul 11 [Epub]. https://doi.org/10.1016/j.aucc.2018.06.001.
Article44. Gillespie DJ, Rehder K. Body position and ventilation-perfusion relationships in unilateral pulmonary disease. Chest. 1987; 91:75–9.45. Mezidi M, Guérin C. Effects of patient positioning on respiratory mechanics in mechanically ventilated ICU patients. Ann Transl Med. 2018; 6:384.
Article46. Lai CC, Chou W, Chan KS, Cheng KC, Yuan KS, Chao CM, et al. Early mobilization reduces duration of mechanical ventilation and intensive care unit stay in patients with acute respiratory failure. Arch Phys Med Rehabil. 2017; 98:931–9.
Article47. Wang TH, Wu CP, Wang LY. Chest physiotherapy with early mobilization may improve extubation outcome in critically ill patients in the intensive care units. Clin Respir J. 2018; 12:2613–21.
Article48. Ambrosino N, Venturelli E, Vagheggini G, Clini E. Rehabilitation, weaning and physical therapy strategies in chronic critically ill patients. Eur Respir J. 2012; 39:487–92.
Article49. Bach JR, Gonçalves MR, Hamdani I, Winck JC. Extubation of patients with neuromuscular weakness: a new management paradigm. Chest. 2010; 137:1033–9.50. Gonçalves MR, Honrado T, Winck JC, Paiva JA. Effects of mechanical insufflation-exsufflation in preventing respiratory failure after extubation: a randomized controlled trial. Crit Care. 2012; 16:R48.
Article51. Homnick DN. Mechanical insufflation-exsufflation for airway mucus clearance. Respir Care. 2007; 52:1296–305.52. McCarren B, Alison JA, Herbert RD. Manual vibration increases expiratory flow rate via increased intrapleural pressure in healthy adults: an experimental study. Aust J Physiother. 2006; 52:267–71.
Article53. Hristara-Papadopoulou A, Tsanakas J, Diomou G, Papadopoulou O. Current devices of respiratory physiotherapy. Hippokratia. 2008; 12:211–20.54. AARC clinical practice guideline. Use of positive airway pressure adjuncts to bronchial hygiene therapy: American Association for Respiratory Care. Respir Care. 1993; 38:516–21.55. Paneroni M, Clini E, Simonelli C, Bianchi L, Degli Antoni F, Vitacca M. Safety and efficacy of short-term intrapulmonary percussive ventilation in patients with bronchiectasis. Respir Care. 2011; 56:984–8.
Article56. Butts CA, Brady JJ 3rd, Wilhelm S, Castor L, Sherwood A, McCall A, et al. Do simple beside lung function tests predict morbidity after rib fractures? Am J Surg. 2017; 213:473–7.
Article57. Meynaerts A, Michels A, Leysen R, Heremans A, Sabbe M, Delooz H, et al. The effectiveness of incentive spirometry in hospitalised patients with blunt thoracic trauma. Acta Anaesthesiol Belg. 1999; 50:139.58. Grammatopoulou E, Belimpasaki V, Valalas A, Michos P, Skordilis E, Koutsouki D. Active cycle of breathing techniques contributes to pain reduction in patients with rib fractures. Hell Cheirourgike. 2010; 82:52–8.
Article59. Gosselink R, Clerckx B, Robbeets C, Vanhullebusch T, Vanpee G, Segers J. Physiotherapy in the Intensive Care Unit. Neth J Crit Care. 2011; 15:66–75.60. Morris PE, Goad A, Thompson C, Taylor K, Harry B, Passmore L, et al. Early intensive care unit mobility therapy in the treatment of acute respiratory failure. Crit Care Med. 2008; 36:2238–43.
Article61. Schieren M, Piekarski F, Dusse F, Marcus H, Poels M, Wappler F, et al. Continuous lateral rotational therapy in trauma: a systematic review and meta-analysis. J Trauma Acute Care Surg. 2017; 83:926–33.62. Griffiths RD, Palmer TE, Helliwell T, MacLennan P, MacMillan RR. Effect of passive stretching on the wasting of muscle in the critically ill. Nutrition. 1995; 11:428–32.
Article63. Edwards J, McWilliams D, Thomas M, Shah S. Electrical muscle stimulation in the intensive care unit: an integrative review. J Intensive Care Soc. 2014; 15:142–9.
Article64. Gerovasili V, Tripodaki E, Karatzanos E, Pitsolis T, Markaki V, Zervakis D, et al. Short-term systemic effect of electrical muscle stimulation in critically ill patients. Chest. 2009; 136:1249–56.
Article65. Fossat G, Baudin F, Courtes L, Bobet S, Dupont A, Bretagnol A, et al. Effect of in-bed leg cycling and electrical stimulation of the quadriceps on global muscle strength in critically ill adults: a randomized clinical trial. JAMA. 2018; 320:368–78.66. Chang AT, Boots R, Hodges PW, Paratz J. Standing with assistance of a tilt table in intensive care: a survey of Australian physiotherapy practice. Aust J Physiother. 2004; 50:51–4.
Article67. Bourdin G, Barbier J, Burle JF, Durante G, Passant S, Vincent B, et al. The feasibility of early physical activity in intensive care unit patients: a prospective observational one-center study. Respir Care. 2010; 55:400–7.68. Sommers J, Engelbert RH, Dettling-Ihnenfeldt D, Gosselink R, Spronk PE, Nollet F, et al. Physiotherapy in the intensive care unit: an evidence-based, expert driven, practical statement and rehabilitation recommendations. Clin Rehabil. 2015; 29:1051–63.
Article69. Fuest K, Schaller SJ. Recent evidence on early mobilization in critical-Ill patients. Curr Opin Anaesthesiol. 2018; 31:144–50.
Article70. Engels PT, Beckett AN, Rubenfeld GD, Kreder H, Finkelstein JA, da Costa L, et al. Physical rehabilitation of the critically ill trauma patient in the ICU. Crit Care Med. 2013; 41:1790–801.
Article71. Schaller SJ, Anstey M, Blobner M, Edrich T, Grabitz SD, Gradwohl-Matis I, et al. Early, goal-directed mobilisation in the surgical intensive care unit: a randomised controlled trial. Lancet. 2016; 388:1377–88.
Article
