Pharmacologic therapy for nonalcoholic steatohepatitis focusing on pathophysiology
- Affiliations
-
- 1Department of Internal Medicine, Myongji Hospital, Hanyang University College of Medicine, Goyang, Korea. dreundavis@gmail.com
- KMID: 2449317
- DOI: http://doi.org/10.12701/yujm.2019.00171
Abstract
- The paradigm of chronic liver diseases has been shifting. Although hepatitis B and C viral infections are still the main causes of liver cirrhosis and hepatocellular carcinoma (HCC), the introduction of effective antiviral drugs may control or cure them in the near future. In contrast, the burden of nonalcoholic fatty liver disease (NAFLD) has been increasing for decades, and 25 to 30% of the general population in Korea is estimated to have NAFLD. Over 10% of NAFLD patients may have nonalcoholic steatohepatitis (NASH), a severe form of NAFLD. NASH can progress to cirrhosis and HCC. NASH is currently the second leading cause to be placed on the liver transplantation list in the United States. NAFLD is associated with obesity, type 2 diabetes, dyslipidemia, and metabolic syndrome. The pathophysiology is complex and associated with lipotoxicity, inflammatory cytokines, apoptosis, and insulin resistance. The only proven effective treatment is weight reduction by diet and exercise. However, this may not be effective for advanced fibrosis or cirrhosis. Therefore, effective drugs are urgently needed for treating these conditions. Unfortunately, no drugs have been approved for the treatment of NASH. Many pharmaceutical companies are trying to develop new drugs for the treatment of NASH. Some of them are in phase 2 or 3 clinical trials. Here, pharmacologic therapies in clinical trials, as well as the basic principles of drug therapy, will be reviewed, focusing on pathophysiology.
MeSH Terms
Figure
-

Fig. 1. Lipotoxicity. Although the major form of lipids is TG, other lipid metabolites also accumulate: FFAs, FC, diacylglycerol, CE, and ceramide. “The quality” rather than “quantity” of lipids may contribute to lipotoxicity. Especially, FC and FFAs are important mediators of lipotoxicity. They up-regulate death receptors, then sensitizing them to TNF-α. They also trigger ER stress, causing mitochondrial dysfunction and apoptosis (adapted from Okazaki I. [Non-alcoholic steatohepatitis]. Cho YK, Eun JR, translators. Paju: Koonja Publishing Inc.; 2018. p. 152 [5], with permission of Koonja Publishing Inc.). TG, triglyceride; FFA, free fatty acid; FC, free cholesterol; CE, cholesterol ester; TNF-α, tumor necrosis factor-α; ER, endoplasmic reticulum; TNF-R1, tumor necrosis factor receptor 1; TRAIL-R, TNF-related apoptosis-inducing ligand receptor; ROS, reactive oxygen species.
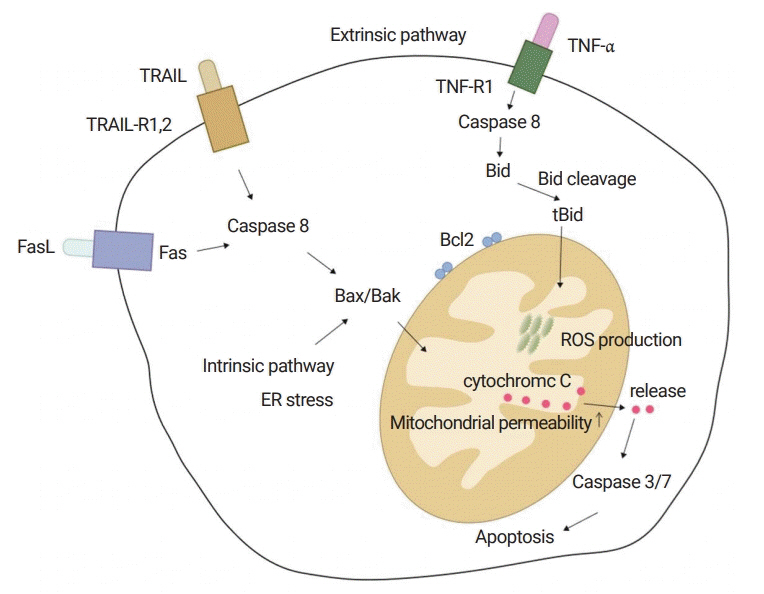
Fig. 2. Basic concept of apoptosis. Apoptosis is a key consequence of cell injury. There are two pathways: extrinsic pathway via death-receptors, such as the TNF-α receptor, Fas, and TRAIL; and the intrinsic pathway via ER stress. Both pathways go through the mitochondria. Mitochondrial dysfunction is a key event of apoptosis. Caspases are enzymes associated with the apoptotic process. Caspase 8 is an initiator caspase and caspase 3/7 is an effector caspase. The Bcl2 family is also involved with apoptosis. Bid, Bad, Bim, and Bax/Bak are pro-apoptotic and Bcl2 and Bcl-xL are anti-apoptotic. Caspase 8 occurs cleavage of Bid to tBid, leading to mitochondrial permeabilization and the release of cytochrome C. Released cytochrome C activates caspase 3/7, the effector caspase, resulting in the final apoptotic morphology (adapted from Okazaki I. [Non-alcoholic steatohepatitis]. Cho YK, Eun JR, translators. Paju: Koonja Publishing Inc.; 2018. p. 151 [5], with permission of Koonja Publishing Inc.). TNF-α, tumor necrosis factor-α; TRAIL, TNF-related apoptosis-inducing ligand; ER, endoplasmic reticulum; tBid, truncated Bid; ROS, reactive oxygen species.
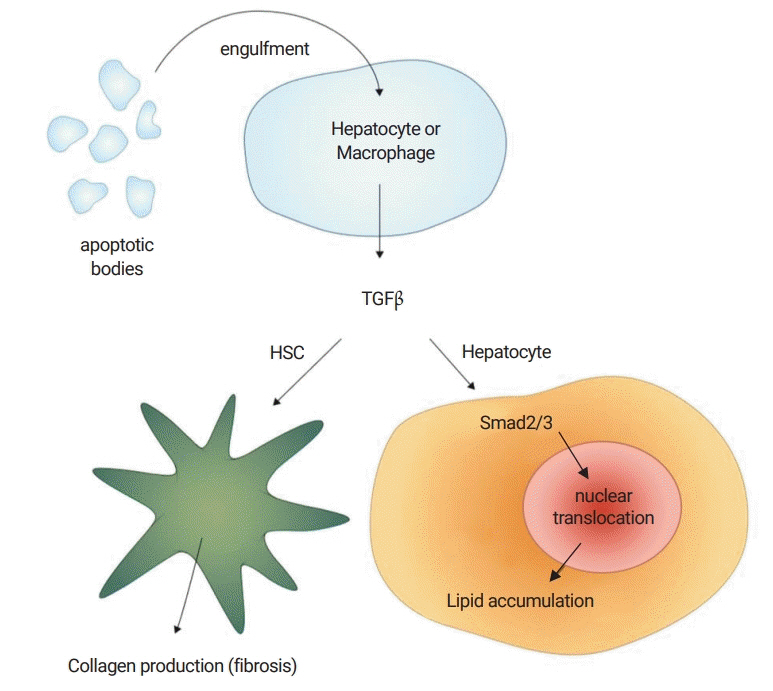
Fig. 3. TGF-β signaling in steatohepatitis. Even hepatocytes, as well as Kupffer cells, phagocytize apoptotic cell debris. They release TGF-β, the main cytokine in fibrosis, which causes the activation of HSCs and more accumulation of lipids in hepatocytes via Smad2/3 (adapted from Okazaki I. [Non-alcoholic steatohepatitis]. Cho YK, Eun JR, translators. Paju: Koonja Publishing Inc.; 2018. p. 154 [5], with permission of Koonja Publishing Inc.). TGF-β, transforming growth factor-β; HSC, hepatic stellate cell.
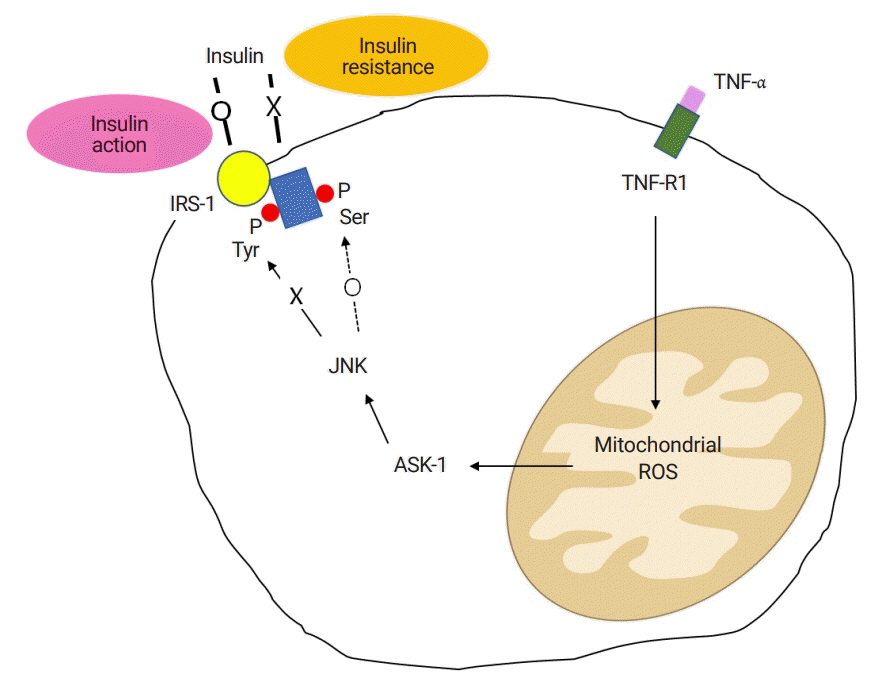
Fig. 4. ASK1 and insulin resistance. The inflammatory cytokine, TNF-α, produces mitochondrial ROS, which activates ASK1. ASK1 activates JNK, and subsequently causes serine phosphorylation of IRS-1. Normally, the tyrosine phosphorylation of IRS-1 is a key event in the action of insulin. Impaired tyrosine phosphorylation and increased serine phosphorylation of IRS-1 are associated with insulin resistance. ASK1, apoptosis signal-regulating kinase 1; TNF-α, tumor necrosis factor-α; ROS, reactive oxygen species; JNK, c-Jun-NH2-terminal kinases; IRS-1, insulin receptor substrate-1; ROS, reactive oxygen species.
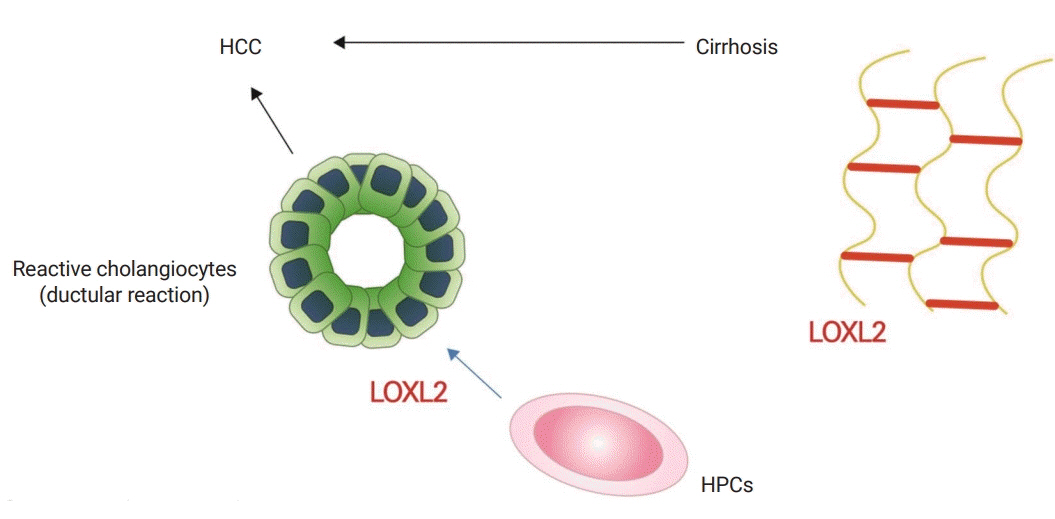
Fig. 5. Lysyl oxidase. The LOX family is composed of four isoforms, LOX and the LOXL1-4. Among them, LOXL2 is a stabilizer of collagen crosslinking. LOXL2 is also expressed in hepatic progenitor cells in fibrotic liver. LOXL2 promotes progenitor cells towards fibrogenic cholangiocytes, suppressing their differentiation into hepatocytes. The ductular reaction characterized by reactive cholangiocytes is associated with hepatocarcinogenesis (adapted from Okazaki I. [Non-alcoholic steatohepatitis]. Cho YK, Eun JR, translators. Paju: Koonja Publishing Inc.; 2018. p. 225 [5], with permission of Koonja Publishing Inc.). LOX, lysyl oxidase; LOXL1-4, LOX-like 1-4; HCC, hepatocellular carcinoma; HPC, hepatic progenitor cell.

Fig. 6. Farnesoid X receptor. The primary bile acids, CA, and CDCA, are synthesized in the liver and secreted into the bile duct. The CYP7A1 is key for this process. Approximately 95% of the primary bile acids are reabsorbed in the ileum. A small proportion (~5%) enters the colon. Here, secondary bile acids are metabolized by intestinal microbiota. The majority of the bile acids are re-used by the enterohepatic circulation and only some are newly-synthesized. The FXR is a key nuclear receptor for bile acid resorption in the ileum. FXR stimulates FGF-19 in the enterocytes, which inhibits CYP7A1, resulting in reduced new bile acid synthesis by negative feedback. The FXR nuclear receptors are also expressed in the liver, adrenal glands and kidneys. In the liver, FXR acts via a SHR. Intrahepatic FXR/SHP represses bile acid synthesis by inhibiting CYP7A1 and TG synthesis by inhibiting SREBP-1c. It also stimulates the β-oxidation of FFAs by PPAR-α activation, increases glycogenesis and suppresses glycolysis. Intestinal FXR induces FGF-19, which increases insulin sensitivity by GLP-1 activation (adapted from Okazaki I. [Non-alcoholic steatohepatitis]. Cho YK, Eun JR, translators. Paju: Koonja Publishing Inc.; 2018. p. 225 [5], with permission of Koonja Publishing Inc.). CA, cholic acid; CDCA, chenodeoxycholic acid; CYP7A1, cytochrome P450 7A1; FXR, farnesoid X receptor; FGF-19, fibroblast growth factor 19; SHR, short heterodimer partner; SHP, short heterodimer partner; TG, triglyceride; FFA, free fatty acid; PPAR-α, peroxisome proliferator-activated receptor-α; GLP-1, glucagon-like peptide-1; ACC, acetyl-CoA carboxylase; FAS, fatty acid synthase; SREBP-1, sterol-responsive element binding protein-1; SCD1, steroyl coenzyme A desaturase 1; DCA, deoxycholic acid; UCDA, ursodeoxycholic acid.
Reference
-
References
1. Oh H, Jun DW, Saeed WK, Nguyen MH. Non-alcoholic fatty liver diseases: update on the challenge of diagnosis and treatment. Clin Mol Hepatol. 2016; 22:327–35.
Article2. Alkhouri N, Dixon LJ, Feldstein AE. Lipotoxicity in nonalcoholic fatty liver disease: not all lipids are created equal. Expert Rev Gastroenterol Hepatol. 2009; 3:445–51.
Article3. Malhi H, Gores GJ. Cellular and molecular mechanisms of liver injury. Gastroenterology. 2008; 134:1641–54.
Article4. Yang L, Roh YS, Song J, Zhang B, Liu C, Loomba R, et al. Transforming growth factor beta signaling in hepatocytes participates in steatohepatitis through regulation of cell death and lipid metabolism in mice. Hepatology. 2014; 59:483–95.
Article5. Okazaki I. [Non-alcoholic steatohepatitis]. YK Cho JR Eun . Paju: Koonja Publishing Inc.;2018.6. Miura K, Yang L, van Rooijen N, Ohnishi H, Seki E. Hepatic recruitment of macrophages promotes nonalcoholic steatohepatitis through CCR2. Am J Physiol Gastrointest Liver Physiol. 2012; 302:G1310–21.
Article7. Tacke F. Cenicriviroc for the treatment of non-alcoholic steatohepatitis and liver fibrosis. Expert Opin Investig Drugs. 2018; 27:301–11.
Article8. Friedman S, Sanyal A, Goodman Z, Lefebvre E, Gottwald M, Fischer L, et al. Efficacy and safety study of cenicriviroc for the treatment of non-alcoholic steatohepatitis in adult subjects with liver fibrosis: CENTAUR Phase 2b study design. Contemp Clin Trials. 2016; 47:356–65.
Article9. Paradis V, Perlemuter G, Bonvoust F, Dargere D, Parfait B, Vidaud M, et al. High glucose and hyperinsulinemia stimulate connective tissue growth factor expression: a potential mechanism involved in progression to fibrosis in nonalcoholic steatohepatitis. Hepatology. 2001; 34:738–44.
Article10. Starley BQ, Calcagno CJ, Harrison SA. Nonalcoholic fatty liver disease and hepatocellular carcinoma: a weighty connection. Hepatology. 2010; 51:1820–32.
Article11. Derosa G. Efficacy and tolerability of pioglitazone in patients with type 2 diabetes mellitus: comparison with other oral antihyperglycaemic agents. Drugs. 2010; 70:1945–61.
Article12. Sanyal AJ, Chalasani N, Kowdley KV, McCullough A, Diehl AM, Bass NM, et al. Pioglitazone, vitamin E, or placebo for nonalcoholic steatohepatitis. N Engl J Med. 2010; 362:1675–85.
Article13. Schuster S, Feldstein AE. NASH: novel therapeutic strategies targeting ASK1 in NASH. Nat Rev Gastroenterol Hepatol. 2017; 14:329–30.
Article14. Loomba R, Lawitz E, Mantry PS, Jayakumar S, Caldwell SH, Arnold H, et al. The ASK1 inhibitor selonsertib in patients with nonalcoholic steatohepatitis: a randomized, phase 2 trial. Hepatology. 2018; 67:549–59.
Article15. Ikenaga N, Peng ZW, Vaid KA, Liu SB, Yoshida S, Sverdlov DY, et al. Selective targeting of lysyl oxidase-like 2 (LOXL2) suppresses hepatic fibrosis progression and accelerates its reversal. Gut. 2017; 66:1697–708.
Article16. Harrison SA, Abdelmalek MF, Caldwell S, Shiffman ML, Diehl AM, Ghalib R, et al. Simtuzumab is ineffective for patients with bridging fibrosis or compensated cirrhosis caused by nonalcoholic steatohepatitis. Gastroenterology. 2018; 155:1140–53.
Article17. Keely SJ, Walters JR. The farnesoid X receptor: good for BAD. Cell Mol Gastroenterol Hepatol. 2016; 2:725–32.
Article18. Mudaliar S, Henry RR, Sanyal AJ, Morrow L, Marschall HU, Kipnes M, et al. Efficacy and safety of the farnesoid X receptor agonist obeticholic acid in patients with type 2 diabetes and nonalcoholic fatty liver disease. Gastroenterology. 2013; 145:574–82.
Article19. Grygiel-Górniak B. Peroxisome proliferator-activated receptors and their ligands: nutritional and clinical implications--a review. Nutr J. 2014; 13:17.20. Miyahara T, Schrum L, Rippe R, Xiong S, Yee HF Jr, Motomura K, et al. Peroxisome proliferator-activated receptors and hepatic stellate cell activation. J Biol Chem. 2000; 275:35715–22.
Article21. van Wagner LB, Rinella ME. The role of insulin-sensitizing agents in the treatment of nonalcoholic steatohepatitis. Therap Adv Gastroenterol. 2011; 4:249–63.
Article22. Bugianesi E, Gentilcore E, Manini R, Natale S, Vanni E, Villanova N, et al. A randomized controlled trial of metformin versus vitamin E or prescriptive diet in nonalcoholic fatty liver disease. Am J Gastroenterol. 2005; 100:1082–90.
Article23. Chalasani N, Younossi Z, Lavine JE, Diehl AM, Brunt EM, Cusi K, et al. The diagnosis and management of non-alcoholic fatty liver disease: practice guideline by the American Association for the Study of Liver Diseases, American College of Gastroenterology, and the American Gastroenterological Association. Am J Gastroenterol. 2012; 107:811–26.
Article24. Armstrong MJ, Gaunt P, Aithal GP, Barton D, Hull D, Parker R, et al. Liraglutide safety and efficacy in patients with non-alcoholic steatohepatitis (LEAN): a multicentre, double-blind, randomised, placebo-controlled phase 2 study. Lancet. 2016; 387:679–90.
Article25. Wadden TA, Hollander P, Klein S, Niswender K, Woo V, Hale PM, et al. Weight maintenance and additional weight loss with liraglutide after low-calorie-diet-induced weight loss: the SCALE Maintenance randomized study. Int J Obes (Lond). 2013; 37:1443–51.
Article26. Milder TY, Stocker SL, Abdel Shaheed C, McGrath-Cadell L, Samocha-Bonet D, Greenfield JR, et al. Combination therapy with an SGLT2 inhibitor as initial treatment for type 2 diabetes: a systematic review and meta-analysis. J Clin Med. 2019; 8:pii: E45.
Article27. Sumida Y, Yoneda M. Current and future pharmacological therapies for NAFLD/NASH. J Gastroenterol. 2018; 53:362–76.
Article28. Shibuya T, Fushimi N, Kawai M, Yoshida Y, Hachiya H, Ito S, et al. Luseogliflozin improves liver fat deposition compared to metformin in type 2 diabetes patients with non-alcoholic fatty liver disease: a prospective randomized controlled pilot study. Diabetes Obes Metab. 2018; 20:438–42.
Article29. Ito D, Shimizu S, Inoue K, Saito D, Yanagisawa M, Inukai K, et al. Comparison of ipragliflozin and pioglitazone effects on nonalcoholic fatty liver disease in patients with type 2 diabetes: a randomized, 24-week, open-label, active-controlled trial. Diabetes Care. 2017; 40:1364–72.
Article30. Tomita K, Teratani T, Suzuki T, Shimizu M, Sato H, Narimatsu K, et al. Free cholesterol accumulation in hepatic stellate cells: mechanism of liver fibrosis aggravation in nonalcoholic steatohepatitis in mice. Hepatology. 2014; 59:154–69.
Article31. Muir K, Hazim A, He Y, Peyressatre M, Kim DY, Song X, et al. Proteomic and lipidomic signatures of lipid metabolism in NASH-associated hepatocellular carcinoma. Cancer Res. 2013; 73:4722–31.
Article32. Filozof C, Goldstein BJ, Williams RN, Sanyal A. Non-alcoholic steatohepatitis: limited available treatment options but promising drugs in development and recent progress towards a regulatory approval pathway. Drugs. 2015; 75:1373–92.
Article33. Sanyal AJ, Abdelmalek MF, Suzuki A, Cummings OW, Chojkier M; EPE-A Study Group. No significant effects of ethyl-eicosapentanoic acid on histologic features of nonalcoholic steatohepatitis in a phase 2 trial. Gastroenterology. 2014; 147:377–84.
Article34. Scorletti E, Bhatia L, McCormick KG, Clough GF, Nash K, Hodson L, et al. Effects of purified eicosapentaenoic and docosahexaenoic acids in nonalcoholic fatty liver disease: results from the Welcome* study. Hepatology. 2014; 60:1211–21.
Article35. Wang X, Ren Q, Wu T, Guo Y, Liang Y, Liu S. Ezetimibe prevents the development of non alcoholic fatty liver disease induced by high fat diet in C57BL/6J mice. Mol Med Rep. 2014; 10:2917–23.36. Loomba R, Sirlin CB, Ang B, Bettencourt R, Jain R, Salotti J, et al. Ezetimibe for the treatment of nonalcoholic steatohepatitis: assessment by novel magnetic resonance imaging and magnetic resonance elastography in a randomized trial (MOZART trial). Hepatology. 2015; 61:1239–50.
Article37. Hirose A, Ono M, Saibara T, Nozaki Y, Masuda K, Yoshioka A, et al. Angiotensin II type 1 receptor blocker inhibits fibrosis in rat nonalcoholic steatohepatitis. Hepatology. 2007; 45:1375–81.
Article38. Georgescu EF, Ionescu R, Niculescu M, Mogoanta L, Vancica L. Angiotensin-receptor blockers as therapy for mild-to-moderate hypertension-associated non-alcoholic steatohepatitis. World J Gastroenterol. 2009; 15:942–54.
Article39. McPherson S, Wilkinson N, Tiniakos D, Wilkinson J, Burt AD, McColl E, et al. A randomised controlled trial of losartan as an anti-fibrotic agent in non-alcoholic steatohepatitis. PLoS One. 2017; 12:e0175717.
Article40. Connolly JJ, Ooka K, Lim JK. Future pharmacotherapy for non-alcoholic steatohepatitis (NASH): review of phase 2 and 3 trials. J Clin Transl Hepatol. 2018; 6:264–75.
Article41. Abenavoli L, Falalyeyeva T, Boccuto L, Tsyryuk O, Kobyliak N. Obeticholic acid: a new era in the treatment of nonalcoholic fatty liver disease. Pharmaceuticals (Basel). 2018; 11:pii: E104.
Article42. Neuschwander-Tetri BA, Loomba R, Sanyal AJ, Lavine JE, Van Natta ML, Abdelmalek MF, et al. Farnesoid X nuclear receptor ligand obeticholic acid for non-cirrhotic, non-alcoholic steatohepatitis (FLINT): a multicentre, randomised, placebo-controlled trial. Lancet. 2015; 385:956–65.
Article43. Imoto K, Kukidome D, Nishikawa T, Matsuhisa T, Sonoda K, Fujisawa K, et al. Impact of mitochondrial reactive oxygen species and apoptosis signal-regulating kinase 1 on insulin signaling. Diabetes. 2006; 55:1197–204.
Article44. Ratziu V, Harrison SA, Francque S, Bedossa P, Lehert P, Serfaty L, et al. Elafibranor, an agonist of the peroxisome proliferator-activated receptor-α and -δ, induces resolution of nonalcoholic steatohepatitis without fibrosis worsening. Gastroenterology. 2016; 150:1147–59.
Article45. Shiffman M, Freilich B, Vuppalanchi R, Watt K, Chan JL, Spada A, et al. Randomised clinical trial: emricasan versus placebo significantly decreases ALT and caspase 3/7 activation in subjects with non-alcoholic fatty liver disease. Aliment Pharmacol Ther. 2019; 49:64–73.
Article46. Garcia-Tsao G, Fuchs M, Shiffman M, Borg BB, Pyrsopoulos N, Shetty K, et al. Emricasan (IDN-6556) Lowers portal pressure in patients with compensated cirrhosis and severe portal hypertension. Hepatology. 2019; 69:717–28.
Article47. Safadi R, Konikoff FM, Mahamid M, Zelber-Sagi S, Halpern M, Gilat T, et al. The fatty acid-bile acid conjugate Aramchol reduces liver fat content in patients with nonalcoholic fatty liver disease. Clin Gastroenterol Hepatol. 2014; 12:2085–91.
Article48. Harrison SA, Rinella ME, Abdelmalek MF, Trotter JF, Paredes AH, Arnold HL, et al. NGM282 for treatment of non-alcoholic steatohepatitis: a multicentre, randomised, double-blind, placebo-controlled, phase 2 trial. Lancet. 2018; 391:1174–85.
Article49. Sanyal A, Charles ED, Neuschwander-Tetri BA, Loomba R, Harrison SA, Abdelmalek MF, et al. Pegbelfermin (BMS-986036), a PEGylated fibroblast growth factor 21 analogue, in patients with non-alcoholic steatohepatitis: a randomised, double-blind, placebo-controlled, phase 2a trial. Lancet. 2019; 392:2705–17.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Nonalcoholic Steatohepatitis
- Pathology of nonalcoholic steatohepatitis
- Clinical Predictors Reflecting the Pathologic Severity of Nonalcoholic Steatohepatitis in Patients with Nonalcoholic Fatty Liver
- The Diagnosis of Nonalcoholic Fatty Liver Disease
- Nonalcoholic fatty liver disease and alcohol-related liver disease: From clinical aspects to pathophysiological insights
