Clinical Characteristics of Intraocular Foreign Bodies According to Entrance Location: Corneal vs. Non-Corneal
- Affiliations
-
- 1Department of Ophthalmology, Pusan National University School of Medicine, Yangsan, Korea. oph97@naver.com
- 2Medical Research Institute, Pusan National University Hospital, Busan, Korea.
- KMID: 2443151
- DOI: http://doi.org/10.3341/jkos.2019.60.4.348
Abstract
- PURPOSE
To investigate differences in the clinical features of post-traumatic intraocular foreign bodies (IOFBs) according to their entrance locations, specifically, those penetrating the cornea and those not penetrating the cornea.
METHODS
A retrospective chart review was performed of patients with an IOFB from January 2011 to July 2016. The patients were divided into two groups: those in whom the IOFB entered through the cornea ("corneal entrance" group) and those in whom the IOFB did not penetrate the cornea ("non-corneal entrance" group), and compared. Damage to the anterior and posterior capsule, retinal tear, and retinal detachment were analyzed, and differences in surgical techniques including the IOFB extraction route and intraocular lens implantation were recorded.
RESULTS
A total of 43 eyes (43 patients) were included, with 33 (76.7%) in the corneal entrance group and 10 (23.3%) in the non-corneal group. The posterior capsule was preserved in 24.2% (eight) of eyes in the corneal group and 80% (eight) of eyes in the non-corneal group. The corneal group had significantly more posterior capsule ruptures but dramatically fewer retinal tears (39.4%) than the non-corneal group (80% retinal tears).
CONCLUSIONS
The location of IOFB entrance is a predictable factor of lens capsule and retinal injuries.
MeSH Terms
Figure
-

Figure 1 Case 1. (A) A preoperative photo of anterior segment shows 1.5 mm sized laceration at the center of cornea. (B) Computed tomography shows an intraocular foreign body in the left eye. (C) A postoperative photo of anterior segment shows an intraocular lens inserted in the ciliary sulcus. (D) There is no retinal injury in a postoperative fundus photo.
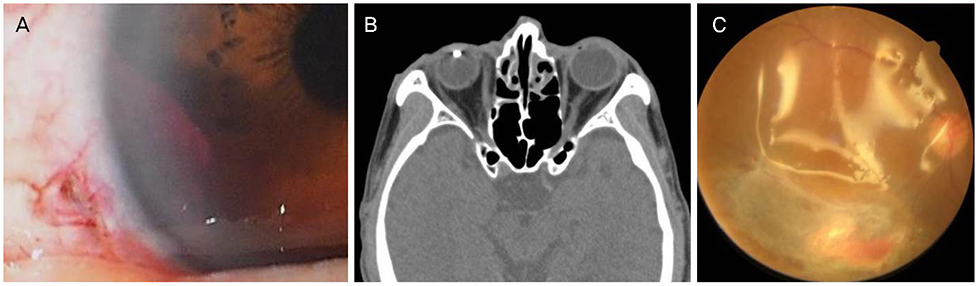
Figure 2 Case 2. (A) A preoperative photo of anterior segment shows 3 mm sized laceration in sclera which is 1 mm apart from limbus. (B) Computed tomography shows an intraocular foreign body in the right eye. (C) A postoperative fundus photo. Because of retinal tear and detachment, silicone oil was injected.

Figure 3 Schematic illustration of intraocular damage according to the entrance of intraocular foreign body (IOFB). (A) Corneal entrance; IOFB usually passed the cornea and lens. In such cases, posterior capsule of lens is ruptured commonly. However retinal tear happened less frequently due to bumpers of cornea and lens. (B) Limbal entrance, (C) Scleral entrance; because there was no bumpers of cornea and lens, incidence of retinal injury is higher.
Reference
-
1. Shock JP, Adams D. Long-term visual acuity results after penetrating and perforating ocular injuries. Am J Ophthalmol. 1985; 100:714–718.
Article2. Lam DS, Tham CC, Kwok AK, et al. Combined phacoemulsification, pars plana vitrectomy, removal of intraocular foreign body (IOFB), and primary intraocular lens implantation for patients with IO FB and traumatic cataract. Eye (Lond). 1998; 12:395–398.3. Tyagi AK, Kheterpal S, Callear AB, et al. Simultaneous posterior chamber intraocular lens implant combined with vitreoretinal surgery for intraocular foreign body injuries. Eye (Lond). 1998; 12(Pt 2):230–233.
Article4. Yeh S, Colyer MH, Weichel ED. Current trends in the management of intraocular foreign bodies. Curr Opin Ophthalmol. 2008; 19:225–233.
Article5. Singh R, Bhalekar S, Dogra MR, Gupta A. 23-gauge vitrectomy with intraocular foreign body removal via the limbus: an alternative approach for select cases. Indian J Ophthalmol. 2014; 62:707–710.
Article6. Cho HJ, Seo MS. Intraocular foreign bodies: clinical characteristics and visual prognosis. J Korean Ophthalmol Soc. 2002; 43:1968–1975.7. Lee EH, Moon CS, Lee SY, Lew HM. Factors influencing final visual outcome in intraocular foreign bodies. J Korean Ophthalmol Soc. 2001; 42:997–1002.8. Jonas JB, Knorr HL, Budde WM. Prognostic factors in ocular injuries caused by intraocular or retrobulbar foreign bodies. Ophthalmology. 2000; 107:823–828.
Article9. Choragiewicz T, Nowomiejska K, Wertejuk K, et al. Surgical treatment of open globe trauma complicated with the presence of an intraocular foreign body. Klin Oczna. 2015; 117:5–8.10. Lit ES, Young LH. Anterior and posterior segment intraocular foreign bodies. Int Ophthalmol Clin. 2002; 42:107–120.
Article11. Katz G, Moisseiev J. Posterior-segment intraocular foreign bodies: an update on management. Retin Physician. 2009; 6:32–34.12. Rathod R, Mieler WF. An update on the management of intraocular foreign bodies. Retin Physician. 2011; 8:52–55.13. Upshaw JE, Brenkert TE, Losek JD. Ocular foreign bodies in children. Pediatr Emerg Care. 2008; 24:409–414. quiz 415-7.
Article14. Zhang Y, Zhang M, Jiang C, Qiu HY. Intraocular foreign bodies in China: clinical characteristics, prognostic factors, and visual outcomes in 1,421 eyes. Am J Ophthalmol. 2011; 152:66–73.e1.
Article15. Jin YH, Kim YY, Kim SD. Simultaneous phacoemulsification, pars plana vitrectomy, intraocular foreign body extraction, and intraocular lens implantation. J Korean Ophthalmol Soc. 2002; 43:692–699.16. Dhoble P, Khodifad A. Combined cataract extraction with pars plana vitrectomy and metallic intraocular foreign body removal through sclerocorneal tunnel using a novel “Magnet Handshake” technique. Asia Pac J Ophthalmol (Phila). 2018; 7:114–118.
Article17. Yuksel K, Celik U, Alagoz C, et al. 23 Gauge pars plana vitrectomy for the removal of retained intraocular foreign bodies. BMC Ophthalmol. 2015; 15:75.
Article18. Ravani R, Chawla R, Azad SV, et al. Midline sclerotomy approach for intraocular foreign body removal in phakic eyes using endoilluminator: A novel technique. Indian J Ophthalmol. 2018; 66:687–690.
Article19. Park JH, Lee JH, Shin JP, et al. Intraocular foreign body removal by viscoelastic capture using DisCoVisc during 23-gauge microincision vitrectomy surgery. Retina. 2013; 33:1070–1072.
Article20. Gonzalez-Cortes JH, Bages-Rousselon Y, Gonzalez-Cantu JE, Mohamed-Hamsho J. Minimally invasive surgery for the removal of posterior intraocular foreign bodies. J Ophthalmic Vis Res. 2017; 12:236–240.21. Shim KY, Kim YJ, Kim JG, et al. Clinical characteristics of intraocular foreign body and analysis of prognostic factors. J Korean Ophthalmol Soc. 2013; 54:456–461.
Article22. Park CH, Oum BS. A clinical evaluation of intraocular foreign bodies. J Korean Ophthalmol Soc. 1991; 32:498–508.
