Long-term Results of Mini Asymmetric Radial Keratotomy and Corneal Cross-linking for the Treatment of Keratoconus
- Affiliations
-
- 1Abbondanza Eye Centers, Rome and Milan, Italy. info@abbondanza.org
- 2Centre for International Security Studies, The University of Sydney, Sydney, Australia.
- 3Graduate School of Public Health, St. Luke's International University, Tokyo, Japan.
- KMID: 2442624
- DOI: http://doi.org/10.3341/kjo.2018.0028
Abstract
- PURPOSE
To investigate the long-term results (at least 5 years of follow-up) of the mini asymmetric radial keratotomy (MARK) and corneal cross-linking (CXL) combined intervention, also known as the "˜Rome protocol,' for patients with progressive stage I and II keratoconus and contact lens intolerance.
METHODS
This was a retrospective observational case series. Fifteen eyes of 12 patients were evaluated, with a mean follow-up of 6.9 years. To assess the efficacy and stability of the MARK + CXL combined protocol, best spectacle-corrected visual acuity, mean pachymetry, and mean keratometry were recorded preoperatively and at least 1, 3, and 5 years postoperatively. Statistical analysis was performed using the R platform and involved the Wilcoxon signed-rank and Kruskal-Wallis non-parametric tests.
RESULTS
Best spectacle-corrected visual acuity improved for all patients, from 0.46 ± 0.69 logarithm of the minimum angle of resolution (20 / 60) to 0.15 ± 0.69 logarithm of the minimum angle of resolution (20 / 30, p = 0.0006), while mean pachymetry increased in 93% of patients, from 442.80 ± 61.02 to 464.50 ± 62.72 µm (p = 0.003). Lastly, mean keratometry improved in 87% of patients after 6.9 years of observation from 48.82 ± 5.00 to 43.25 ± 3.58 diopters (p = 0.008). No intraoperative or postoperative complications were observed.
CONCLUSIONS
The MARK + CXL combined protocol was effective in treating keratoconus by halting corneal thinning and bulging. In addition, this procedure significantly improved visual acuity based on long-term follow-up data. Analysis of data from a larger cohort of patients would be useful to support these findings.
MeSH Terms
Figure
-

Fig. 1 Diagram of mini asymmetric radial keratotomy mini-incisions.

Fig. 2 The Abbondanza markers.
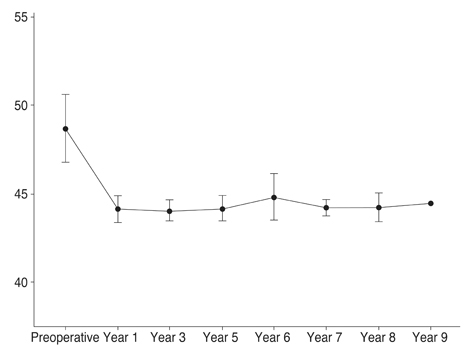
Fig. 3 Mean keratometry changes (with confidence intervals) before and after surgery. A Kruskal-Wallis non-parametric test showed that mean keratometry values do not have identical data distributions in the follow-up period (p = 0.175). A Wilcoxon signed-rank test indicates that postoperative Kavg values after 7 years are significantly lower than preoperative values (p < 0.05).
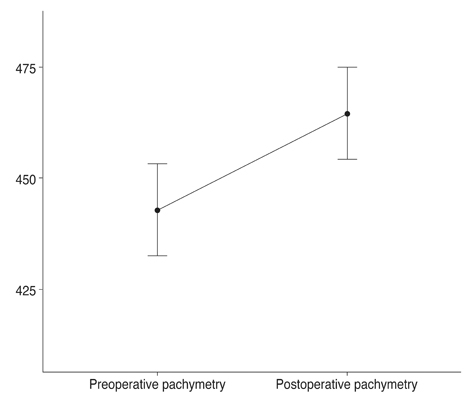
Fig. 4 Mean pachymetry (with 95% confidence intervals) before and after surgery. A Wilcoxon signed-rank test showed that postoperative pachymetry is significantly higher than preoperative pachymetry (p < 0.005).

Fig. 5 Pachymetric map (A) before and (B) after surgery, showing a general improvement in corneal thickness.
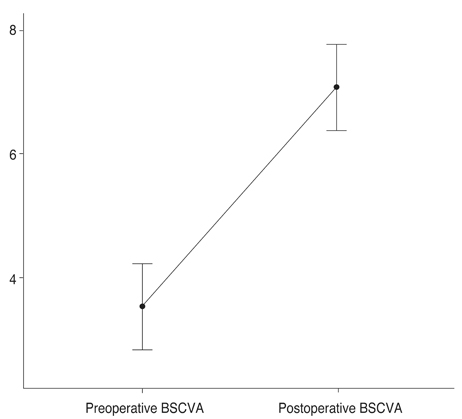
Fig. 6 Mean best spectacle-corrected visual acuity (BSCVA) (on a decimal scale with 95% confidence intervals) before and after surgery. A Wilcoxon signed-rank test shows that postoperative BSCVA is significantly higher than preoperative BSCVA (p < 0.005).
Reference
-
1. Grzybowski A. Mauchart did not give the first description of keratoconus. Acta Ophthalmol. 2014; 92:e84–e85.
Article2. Rabinowitz YS. Keratoconus. Surv Ophthalmol. 1998; 42:297–319.
Article3. Oh BL, Kim MK, Wee WR. Comparison of clinical outcomes of same-size grafting between deep anterior lamellar keratoplasty and penetrating keratoplasty for keratoconus. Korean J Ophthalmol. 2013; 27:322–330.
Article4. Kelly TL, Williams KA, Coster DJ. Australian Corneal Graft Registry. Corneal transplantation for keratoconus: a registry study. Arch Ophthalmol. 2011; 129:691–697.5. Wollensak G, Spoerl E, Seiler T. Ribof lavin/ultraviolet-a-induced collagen crosslinking for the treatment of keratoconus. Am J Ophthalmol. 2003; 135:620–627.6. Colin J, Cochener B, Savary G, Malet F. Correcting keratoconus with intracorneal rings. J Cataract Refract Surg. 2000; 26:1117–1122.
Article7. Lombardi M, Abbondanza M. Asymmetric radial keratotomy for the correction of keratoconus. J Refract Surg. 1997; 13:302–307.
Article8. Abbondanza M. Mini Asymmetric R adial K eratotomy (Mini ARK) for the surgical correction of early-stage keratoconus, hyperopia, and mild myopia. Esperienze. 1997; 12:21–24.9. Krumeich JH, Kezirian GM. Circular keratotomy to reduce astigmatism and improve vision in stage I and II keratoconus. J Refract Surg. 2009; 25:357–365.
Article10. Alio JL, Claramonte PJ, Caliz A, Ramzy MI. Corneal modeling of keratoconus by conductive keratoplasty. J Cataract Refract Surg. 2005; 31:190–197.11. Utine CA, Bayraktar S, Kaya V, et al. Radial keratotomy for the optical rehabilitation of mild to moderate keratoconus: more than 5 years' experience. Eur J Ophthalmol. 2006; 16:376–384.
Article12. Kocak I, Aydin A, Kaya F, et al. Efficacy of radial keratotomy in the optical rehabilitation of mild to moderate keratoconus cases. Int Eye Sci. 2015; 15:572–576.13. Fujimoto K, Osawa H, Moriyama T, et al. Long-term stability of minimally invasive radial keratotomy for mild to moderate keratoconus. Asia Pac J Ophthalmol (Phila). 2017; 6:407–411.
Article14. Abbondanza M, Abdolrahimzadeh B, Zuppardo M. Refractive changes following CXL. Cataract Refract Surg Today Eur. 2009; 4:33–38.15. Kanellopoulos AJ, Asimellis G. Keratoconus management: long-term stability of topography-guided normalization combined with high-fluence CXL stabilization (the Athens Protocol). J Refract Surg. 2014; 30:88–93.
Article16. Kanellopoulos AJ, Pamel GJ. Review of current indications for combined very high fluence collagen cross-linking and laser in situ keratomileusis surgery. Indian J Ophthalmol. 2013; 61:430–432.
Article17. El-Raggal TM. Sequential versus concurrent KERARINGS insertion and corneal collagen cross-linking for keratoconus. Br J Ophthalmol. 2011; 95:37–41.
Article18. Fadlallah A, Dirani A, El Rami H, et al. Safety and visual outcome of Visian toric ICL implantation after corneal collagen cross-linking in keratoconus. J Refract Surg. 2013; 29:84–89.
Article19. Kymionis GD, Kontadakis GA, Naoumidi TL, et al. Conductive keratoplasty followed by collagen cross-linking with riboflavin-UV-A in patients with keratoconus. Cornea. 2010; 29:239–243.
Article20. Abbondanza M, Abbondanza G, De Felice V. Mini asymmetric radial keratotomy and corneal cross-linking for the treatment of a bilateral stage IV keratoconus in a 14-year-old child. Med Arch. 2017; 71:69–71.
Article21. Lindstrom RL. Minimally invasive radial keratotomy: mini-RK. J Cataract Refract Surg. 1995; 21:27–34.
Article22. Snibson GR. Collagen cross-linking: a new treatment paradigm in corneal disease: a review. Clin Exp Ophthalmol. 2010; 38:141–153.23. Mastropasqua L. Collagen cross-linking: when and how? A review of the state of the art of the technique and new perspectives. Eye Vis (Lond). 2015; 2:19.
Article24. Lovisolo CF, Mularoni A, Calossi A, et al. Complications of refractive keratotomy. In : Alio JL, Azar DT, editors. Management of complications in refractive surgery. Berlin: Springer;2008. p. 197–224.25. Wilson SL, El Haj AJ, Yang Y. Control of scar tissue formation in the cornea: strategies in clinical and corneal tissue engineering. J Funct Biomater. 2012; 3:642–687.
Article26. Raiskup F, Theuring A, Pillunat LE, Spoerl E. Corneal collagen crosslinking with riboflavin and ultraviolet-A light in progressive keratoconus: ten-year results. J Cataract Refract Surg. 2015; 41:41–46.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Acute Hydrops after Radial Keratotomy on Keratoconus
- Long-Term Results of Three Cases of Radial Keratotomy
- Clinical Results of Riboflavin and Ultraviolet-A-induced Corneal Cross-linking for Progressive Keratoconus in Korean Patients
- Ten-year Results after Conventional Corneal Cross-linking in Korean Patients with Progressive Keratoconus
- The Long-term Clinical Outcome after Corneal Collagen Cross-linking in Korean Patients with Progressive Keratoconus
