Cerebral Air Embolism: a Case Report with an Emphasis of its Pathophysiology and MRI Findings
- Affiliations
-
- 1Department of Radiology, Wonkwang University Hospital, Jeonlabuk-do, Korea. sschoi@wonkwang.ac.kr
- KMID: 2442236
- DOI: http://doi.org/10.13104/imri.2019.23.1.70
Abstract
- Cerebral air embolism (CAE) is a rare complication of various medical procedures. It manifests with symptoms similar to those of typical acute cerebral infarction, however the treatment is quite different. We present a case of arterial CAE that was associated with a disconnected central venous catheter and appeared as punctate dark signal intensities with aliasing artifacts on the susceptibility-weighted filtered phase magnetic resonance image. The susceptibility-weighted filtered phase image can be helpful for diagnosing CAE and the magnetic resonance imaging reflects the pathophysiology of CAE.
MeSH Terms
Figure
-
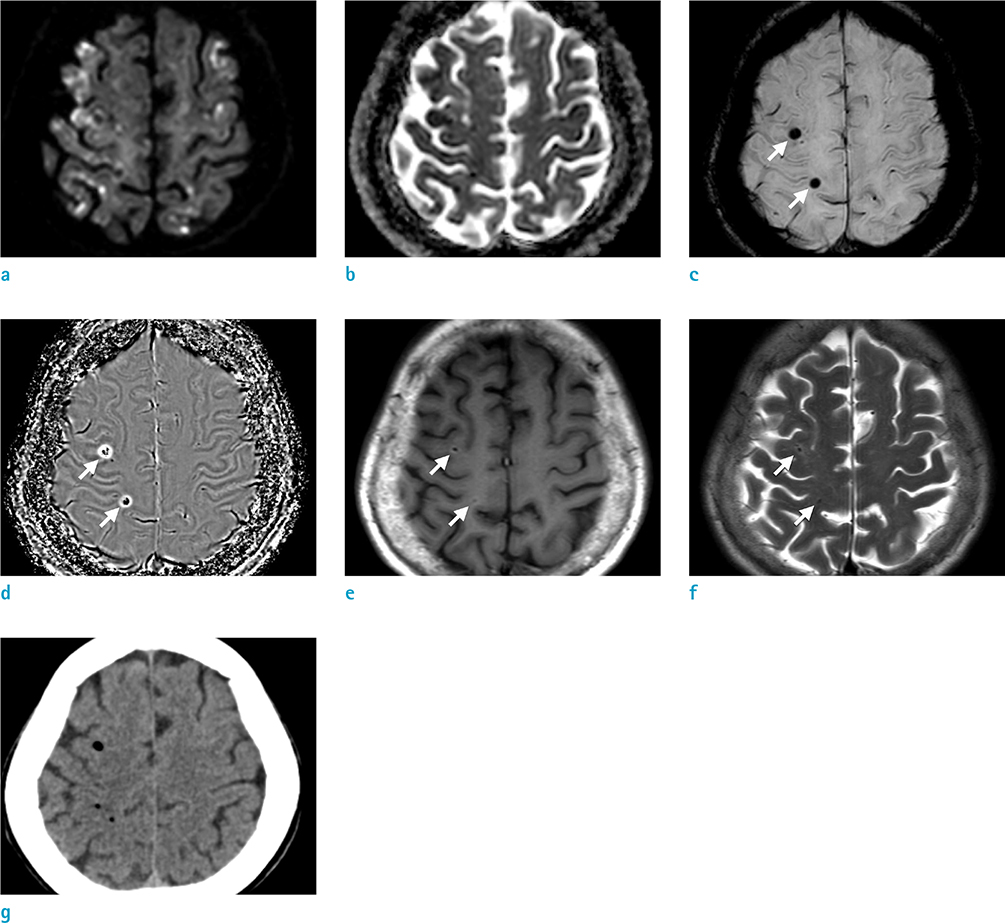
Fig. 1 Initial brain MRI and CT two hours after the onset of symptoms. DWI (a) demonstrates multifocal hyperintensities, seen as low signal foci on the ADC map (b), indicating acute cerebral infarction. SWI shows multifocal dark signal intensities (white arrows) on magnitude image (c) and aliasing artifacts on filtered phase image (d). They also present as dark signal intensities (white arrows) on T1-weighted image (e) and T2-weighted image (f). Immediate brain CT (g) shows multiple punctate air bubbles, indicating arterial CAE.

Fig. 2 Follow-up MRI 12 days later. DWI (a) and ADC map (b) show new diffuse progressing vasogenic edema in cerebral hemispheres. SW magnitude image (c) and filtered phase image (d) show new multifocal tiny dark signal intensities (black arrows) without blooming or aliasing artifacts, suggesting microhemorrhage. The preexisting air bubble (white arrow) shows aliasing artifacts.
Reference
-
1. Jain KK. Textbook of hyperbaric medicine. 6th ed. Switzerland: Springer;2017. p. 121–129.2. Mishra R, Reddy P, Khaja M. Fatal cerebral air embolism: a case series and literature review. Case Rep Crit Care. 2016; 2016:3425321.
Article3. Bauerle J, Fischer A, Hornig T, Egger K, Wengenmayer T, Bardutzky J. Therapeutic hypothermia in cerebral air embolism: a case report. Springerplus. 2013; 2:411.
Article4. Lin C, Barrio GA, Hurwitz LM, Kranz PG. Cerebral air embolism from angioinvasive cavitary aspergillosis. Case Rep Neurol Med. 2014; 2014:406106.
Article5. Suri V, Gupta R, Sharma G, Suri K. An unusual cause of ischemic stroke - Cerebral air embolism. Ann Indian Acad Neurol. 2014; 17:89–91.
Article6. Togo M, Hoshi T, Matsuoka R, Imai Y, Kohara N. Multiple small hemorrhagic infarcts in cerebral air embolism: a case report. BMC Res Notes. 2017; 10:599.
Article7. Caulfield AF, Lansberg MG, Marks MP, Albers GW, Wijman CA. MRI characteristics of cerebral air embolism from a venous source. Neurology. 2006; 66:945–946.
Article8. Kaichi Y, Kakeda S, Korogi Y, et al. Changes over time in intracranial air in patients with cerebral air embolism: radiological study in two cases. Case Rep Neurol Med. 2015; 2015:491017.
Article9. Hwang Y, Kim YJ. Retrograde cerebral venous air embolism on susceptibility-weighted imaging. Can J Neurol Sci. 2018; 45:464–465.
Article10. Han SS, Kim SS, Hong HP, Lee SY, Lee SJ, Lee BK. Massive paradoxical air embolism in brain occurring after central venous catheterization: a case report. J Korean Med Sci. 2010; 25:1536–1538.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Cerebral Air Embolism Following a Gastroscopy
- Gradient-Echo MRI in Defining the Severity of Cerebral Fat Embolism
- Cerebral Air Embolism in a Patient with a Tuberculous-Destroyed Lung during Commercial Air Travel: A Case Report
- Stroke Caused by Cerebral Air Embolism after Central Venous Catheter Removal: A Case Report
- Systemic Air Embolism after CT-guided Transthoracic Needle Biopsy
