Spinal Hydatid Cyst Disease : Challenging Surgery - an Institutional Experience
- Affiliations
-
- 1Department of Neurosurgery, Ankara University School of Medicine, Ankara, Turkey. m.zaimoglu.neurosurgery@gmail.com
- KMID: 2441565
- DOI: http://doi.org/10.3340/jkns.2017.0245
Abstract
OBJECTIVE
Hydatid cyst disease is caused by the parasite Echinococcus granulosus. It is rarely seen in the vertebral system, occurring at a rate of 0.2-1%. The aim of this study is to present 12 spinal hydatid cyst cases, and propose a new type of drainage of the cyst.
METHODS
Twelve cases of spinal hydatid cysts, surgical operations, multiple operations, chronic recurrences, and spinal hydatic cyst excision methods are discussed in the context of the literature. Patients are operated between 2005 and 2016. All the patients are kept under routine follow up. Patient demographic data and clinicopathologic characteristics are examined.
RESULTS
Six male and six female patients with a median age of 38.6 at the time of surgery were included in the study. Spinal cyst hydatid infection sites were one odontoid, one cervical, five thoracic, two lumbar, and three sacral. In all cases, surgery was performed, with the aim of total excision of the cyst, decompression of the spinal cord, and if necessary, stabilization of the spinal column. Mean follow up was 61.3 months (10-156). All the patients were prescribed Albendazole. Three patients had secondary hydatid cyst infection (one lung and two hepatic).
CONCLUSION
The two-way drainage catheter placed inside a cyst provides post-operative chlorhexidine washing inside the cavity. Although a spinal hydatid cyst is a benign pathology and seen rarely, it is extremely difficult to achieve a real cure for patients with this disease. Treatment modalities should be aggressive and include total excision of cyst without rupture, decompression of spinal cord, flushing of the area with scolicidal drugs, and ensuring spinal stabilization. After the operation the patients should be kept under routine follow up. Radiological and clinical examinations are useful in spotting a recurrence.
Keyword
MeSH Terms
Figure
-
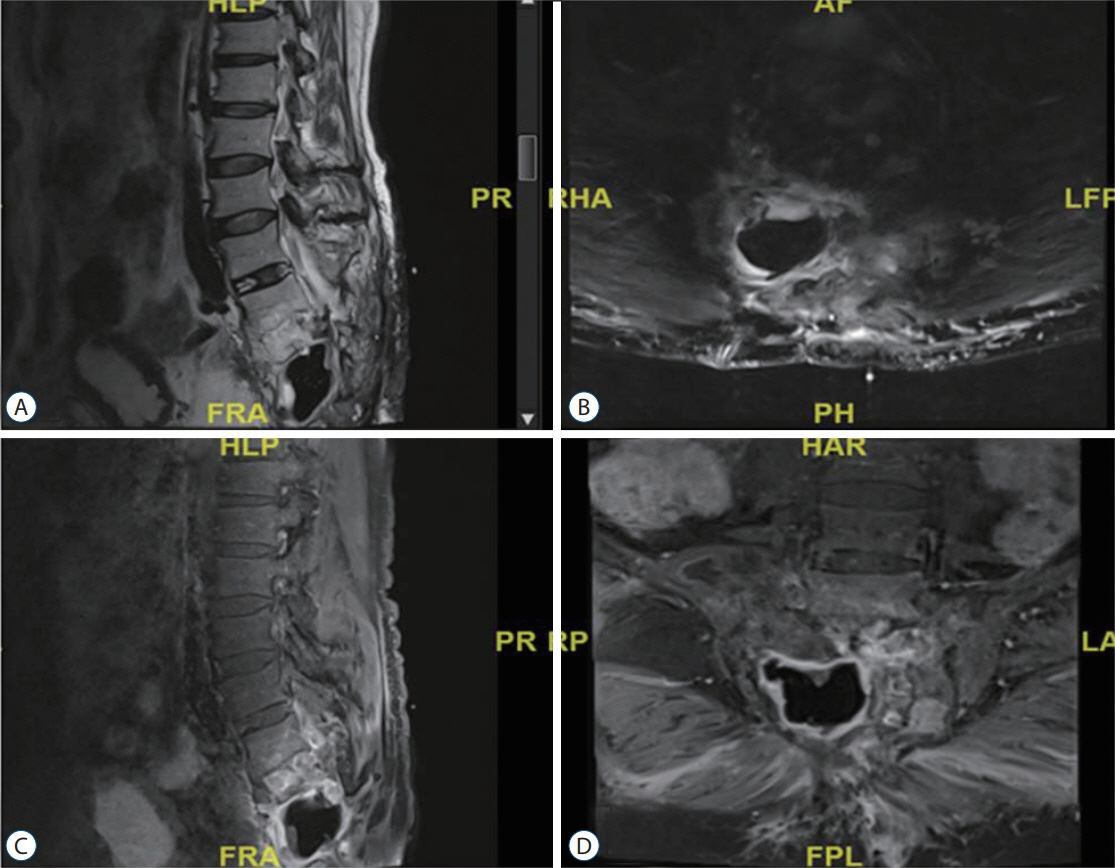
Fig. 1. Patient 11. A : Sagittal T2A weighted MRI showing sacral hydatid cyst infection. B : Sagittal T2A weighted MRI showing sacral hydatid cyst infection and paravertebral involvement. C : Contast enhanced sagittal T1A weighted MR. D : contast enhanced axial T1A weighted MR. MRI : magnetic resonance imaging, MR : magnetic resonance.

Fig. 2. Patient 7, thoracic hydatid cyst. Decompression and instrumentation surgery is performed. Recurrent disease can be seen in paravertebral area and subcutaneous tissue. A : T1A weighted sagittal MRI. B : Contrast enhanced T1A weighted sagittal MRI. C : Contrast enhanced T1A weighted sagittal MRI. D : T2A weighted axial MRI. R : right, L : left, MRI : magnetic resonance imaging.
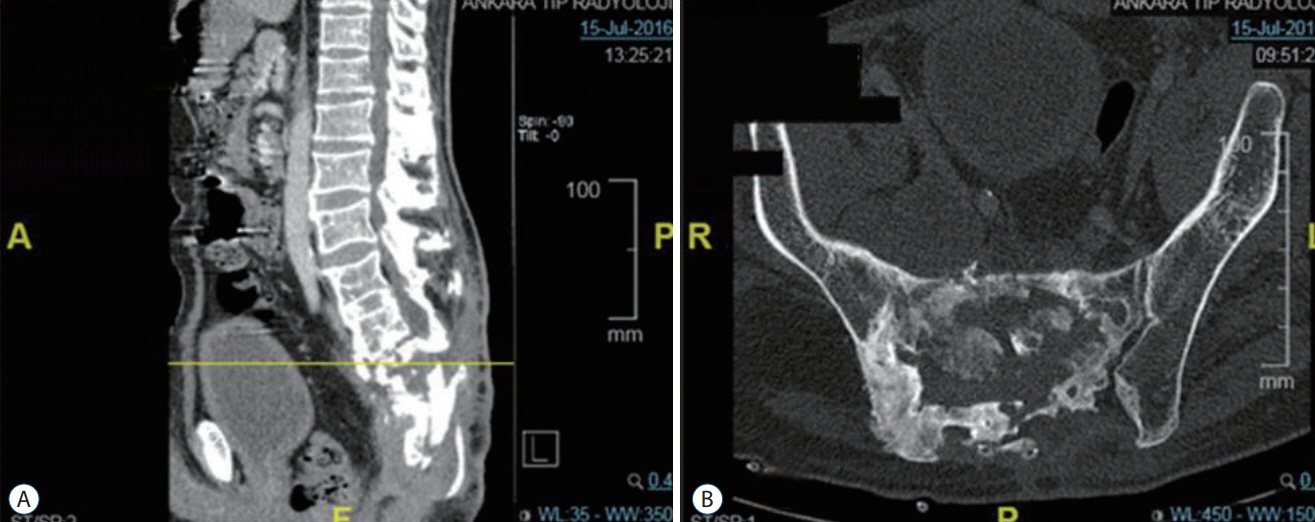
Fig. 3. Patient 1. Sagital (A) and axial computed tomography scan (B) of a sacral hydatid cyst patient, after 3rd operation.

Fig. 4. Patient 4, X-Ray scan of a thoracic hydatid cyst patient. Spinal stabilization and laminectomy were performed. Antero-posterior (A) and lateral X-ray scan (B).

Fig. 5. Continuous drainage of the hydatid cyst.
Reference
-
References
1. Abbassioun K, Amirjamshidi A. Diagnosis and management of hydatid cyst of the central nervous system: Part 2: Hydatid cysts of the skull, orbit, and spine. Neurosurg Q. 11:10–16. 2001.
Article2. Abdelhakim K, Khalil A, Haroune B, Oubaid M, Mondher M. A case of sacral hydatid cyst. Int J Surg Case Rep. 5:434–436. 2014.
Article3. Agnihotri M, Goel N, Shenoy A, Rai S, Goel A. Hydatid disease of the spine: a rare case. J Craniovertebr Junction Spine. 8:159–160. 2017.
Article4. Atalan G, Sivrioglu AK, Sönmez G, Celik M, Simsek B. A case of alveolar echinococcosis presenting as cerebral and spinal intradural metastases. Eurasian J Med. 48:149–152. 2016.
Article5. Bettaieb A, Khaldi M, Ben Rhouma T, Touibi S. Spinal echinococcosis; clinical study of 32 cases (author’s transl). Neurochirugie. 24:205–210. 1978.6. Caglar S, Bozkurt M, Kahilogullari G, Ozdemir M. Management of a rare and dangerous infectious lesion: hydatid cyst disease of the odontoid process. WScJ. 3:29–32. 2012.7. Celik C, Münevver FS, Ucan H. Spinal hydatid cyst: review. Türkiye Klinikleri J Med Sci. 30:1073–1077. 2010.
Article8. Cheng GY. Hydatid cysts of the spinal canal. Zhonghua Fang She Xue Za Zhi. 13:48–49. 1979.9. Claudon M, Bracard S, Plenat F, Regent D, Bernadac P, Picard L. Spinal involvement in alveolar echinococcosis: assessment of two cases. Radiology. 162:571–572. 1987.
Article10. Dogan I, Kahilogullari G, Guner E, Unlu A. A rare and unexpected clinical progress and location on a primary extradural spinal hydatid cyst in a pediatric patient: a case report. Childs Nerv Syst. 31:1407–1411. 2015.
Article11. Fares Y, Khazım R, El Zaatiri MM, Haddad GF, Barnes PR. Spinal hydatid disease and its neurological complications. Scand J Infect Dis. 35:394–396. 2003.
Article12. Faucher JF, Descotes-Genon C, Hoen B, Godard J, Félix S, Aubry S, et al. Hints for control of infection in unique extrahepatic vertebral alveolar echinococcosis. Infection. 45:365–368. 2017.
Article13. Gaucher A, Vinet E, Pere P, Plenat F, Ethgen D, Pourel J. Alveolar echinococcosis with spinal localization. Presse Med. 12:1366. 1983.14. Georges S, Villard O, Filisetti D, Mathis A, Marcellin L, Hansmann Y, et al. Usefulness of PCR analysis for diagnosis of alveolar echinococcosis with unusual localizations: two case studies. J Clin Microbiol. 42:5954–5956. 2004.
Article15. Gezercan Y, Ökten AI, Çavus¸ G¸ Açık V, Bilgin E. Spinal Hydatid Cyst Disease. World Neurosurg. 108:407–417. 2017.
Article16. Herrera A, Martínez AA, Rodríguez J. Spinal hydatidosis. Spine (Phila Pa 1976). 30:2439–2444. 2005.
Article17. Honma K, Basano N, Andoh N, Iwai K. Hepatic alveolar echinococcosis invading pancreas, vertebrae, and spinal cord. Hum Pathol. 13:944–946. 1982.
Article18. Iaroslavskii VE. Primary alveolar echinococcosis of spinal canal. Sov Med. 20:81–83. 1956.19. Is¸lekel S, Ers¸ahin Y, Zileli M, Oktar N, Oner K, Ovül I, et al. Spinal hydatid disease. Spinal Cord. 36:166–170. 1998.
Article20. Jain S, Jaiswal M, Gandhi A, Mittal RS. Primary spinal alveolar hydatid disease: a case series with review of literature. WScJ. 5:12–20. 2014.21. Jaiswal S, Jaiswal AK, Jain M, Behari S, Pandey R. Primary spinal extradural hydatid cyst causing paraplegia. Indian J Pathol Microbiol. 52:432–433. 2009.
Article22. Kadioglu HH, Malcok UA, Senguli G, Aydin IH. Alveolar hydatid disease of the spine causing paraplegia. Neurosciences (Riyadh). 10:180–182. 2005.23. Kahilogullari G, Tuna H, Aydin Z, Colpan E, Egemen N. Primary intradural extramedullary hydatid cyst. Am J Med Sci. 329:202–204. 2005.
Article24. Karray S, Zlitni M, Fowles JV, Zouari O, Slimane N, Kassab MT, et al. Vertebral hydatidosis and paraplegia. J Bone Joint Surg Br. 72:84–88. 1990.
Article25. Keutgens A, Simoni P, Detrembleur N, Frippiat F, Giot JB, Spirlet F, et al. Fatal alveolar echinococcosis of the lumbar spine. J Clin Microbiol. 51:688–691. 2013.
Article26. Kıls¸ç C, k M, Boyar B, Akalan N, Erdem H. Spinal kist hidatikler. Türk Nöros¸ irürji Dergisi Ek. 1:62–64. 1989.27. Kunze V, Layer G, Brüning R, Nägele M. “Metastasizing” echinococcus alveolar of the liver. Radiologe. 32:444–447. 1992.28. Merkle EM, Kramme E, Vogel J, Krämer S, Schulte M, Usadel S, et al. Bone and soft tissue manifestations of alveolar echinococcosis. Skeletal Radiol. 26:289–292. 1997.
Article29. Nell M, Burgkart RH, Gradl G, von Eisenhart-Rothe R, Schaeffeler C, Trappe D, et al. Primary extrahepatic alveolar echinococcosis of the lumbar spine and the psoas muscle. Ann Clin Microbiol Antimicrob. 10:13. 2011.
Article30. Neumayr A, Tamarozzi F, Goblirsch S, Blum J, Brunetti E. Spinal cystic echinococcosis--a systematic analysis and review of the literature: part 2. Treatment, follow-up and outcome. PLoS Negl Trop Dis. 7:e2458. 2013.31. Nourrisson C, Mathieu S, Beytout J, Cambon M, Poirier P. Osteolytic bone lesion: vertebral alveolar echinococcosis in a patient with splenectomy. Rev Med Interne. 35:399–402. 2014.32. Onal C, Canbolat A, Gokay H, Kaya U, Turker K, Turantan M, et al. Spinal hidatik kistler. Türk Nöros¸ irürji Dergisi Ek. 5:34. 1992.33. Ozdemir HM, Ogün TC, Tasbas B. A lasting solution is hard to achieve in primary hydatid disease of the spine: long-term results and an overview. Spine (Phila Pa 1976). 29:932–937. 2004.34. Pamir MN, Akalan N, Ozgen T, Erbengi A. Spinal hydatid cysts. Surg Neurol. 21:53–57. 1984.
Article35. Papanikolaou A. Osseous hydatid disease. Trans R Soc Trop Med Hyg. 102:233–238. 2008.
Article36. Patel D, Shukla D. Back bugged: A case of sacral hydatid cyst. J Neurosci Rural Pract. 1:43–45. 2010.
Article37. Piarroux M, Piarroux R, Giorgi R, Knapp J, Bardonnet K, Sudre B, et al. Clinical features and evolution of alveolar echinococcosis in France from 1982 to 2007: results of a survey in 387 patients. J Hepatol. 55:1025–1033. 2011.
Article38. Reuter S, Seitz HM, Kern P, Junghanss T. Extrahepatic alveolar echinococcosis without liver involvement: a rare manifestation. Infection. 28:187–192. 2000.
Article39. Savas R, Calli C, Alper H, Yunten N, Ustün EE, Ertugv vrul G, et al. Spinal cord compression due to costal Echinococcus multilocularis. Comput Med Imaging Graph. 23:85–88. 1999.
Article40. Scheuring UJ, Seitz HM, Wellmann A, Hartlapp JH, Tappe D, Brehm K, et al. Long-term benzimidazole treatment of alveolar echinococcosis with hematogenic subcutaneous and bone dissemination. Med Microbiol Immunol. 192:193–195. 2003.
Article41. Sengul G, Kadioglu HH, Kayaoglu CR, Aktas S, Akar A, Aydin IH. Treatment of spinal hydatid disease: a single center experience. J Clin Neurosci. 15:507–510. 2008.
Article42. Somay H, Ayan E, Turk CC, Emon ST, Berkman MZ. Long-term disseminated recurrence in spinal hydatid cyst: a case report. Turk Neurosurg. 24:78–81. 2014.43. Song X, Liu D, Wen H. Diagnostic pitfalls of spinal echinococcosis. J Spinal Disord Tech. 20:180–185. 2007.
Article44. Toussaint F, Pere P, Le Chaffotec L, Grandhaye P, Pourel J, Chary-Valckenaere I. Alveolar echinococcosis of the spine. J Clin Rheumatol. 7:248–251. 2001.
Article45. Turgut M. Hydatid disease of the spine: a survey study from Turkey. Infection. 25:221–226. 1997.
Article46. Unal VM, Ozdemir N, Karadag A, Oguzoglu S, Celik H. Primary sacral hydatid cyst causing cutaneous fistula. J Coll Physicians Surg Pak. 5:311–312. 2017.47. Vizcarra M, Mujica M, Sánchez V, Méndez P. An adolescent with lumbosacral instability due to the presence of a hydatid cyst: a case report. Rev Peru Med Exp Salud Publica. 34:126–131. 2017.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pulmonary Embolism Secondary to Hydatid Cyst of the Right Ventricle: A Case Report
- Renal Hydatid With Tuberculosis in a Child: A Rare Coexistence
- Incidentally Detected Cardiac Cyst Hydatid after Blunt Thoracic Trauma
- Rupture of Right Hepatic Duct into Hydatid Cyst
- US and CT Findings of Splenic Hydatid Cyst: A Case Report
