Acute Crit Care.
2018 Nov;33(4):252-259. 10.4266/acc.00248.
The Effect of Systematic Approach to Tracheostomy Care in Patients Transferred from the Surgical Intensive Care Unit to General Ward
- Affiliations
-
- 1Department of Nursing, Asan Medical Center, Seoul, Korea.
- 2Department of Surgery, National Medical Center, Seoul, Korea.
- 3Department of Surgery, Ulsan University Hospital, Ulsan, Korea.
- 4Department of Trauma Surgery, Gil Medical Center, Gachon University College of Medicine, Incheon, Korea.
- 5Division of Acute Care Surgery, Department of Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. skhong94@amc.seoul.kr
- KMID: 2441243
- DOI: http://doi.org/10.4266/acc.00248
Abstract
- BACKGROUND
The aim of this study was to investigate the effects of using a systematic approach to tracheostomy care by a clinical nurse specialist and surgical intensivists for patients with a tracheostomy who were transferred from the surgical intensive care unit (SICU) to the general ward.
METHODS
In this retrospective study, subjects were limited to SICU patients with a tracheostomy who were transferred to the general ward. The study period was divided into a preintervention period (January 1, 2007 to December 31, 2010) and a postintervention period (January 1, 2011 to December 31, 2014), and electronic medical records were used to analyze and compare patient characteristics, clinical outcomes, and readmission to the SICU.
RESULTS
The analysis included 44 patients in the preintervention group and 96 patients in the postintervention group. Decannulation time (26.7±25.1 vs. 12.1±16.0 days, P=0.003), length of stay in the general ward (70.6±89.1 vs. 40.5±42.2 days, P=0.008), length of total hospital stay (107.5±95.6 vs. 74.7±51.2 days, P=0.009), and readmission rate of SICU decreased due to T-cannula occlusion (58.8% vs. 5.9%, P=0.010).
CONCLUSIONS
Using a systematic approach to tracheostomy care in the general ward led to reduction in decannulation time through professional management, which resulted in a shorter hospital stay. It also lowered SICU readmission by solving problems related to direct T-cannula.
Keyword
MeSH Terms
Figure
-
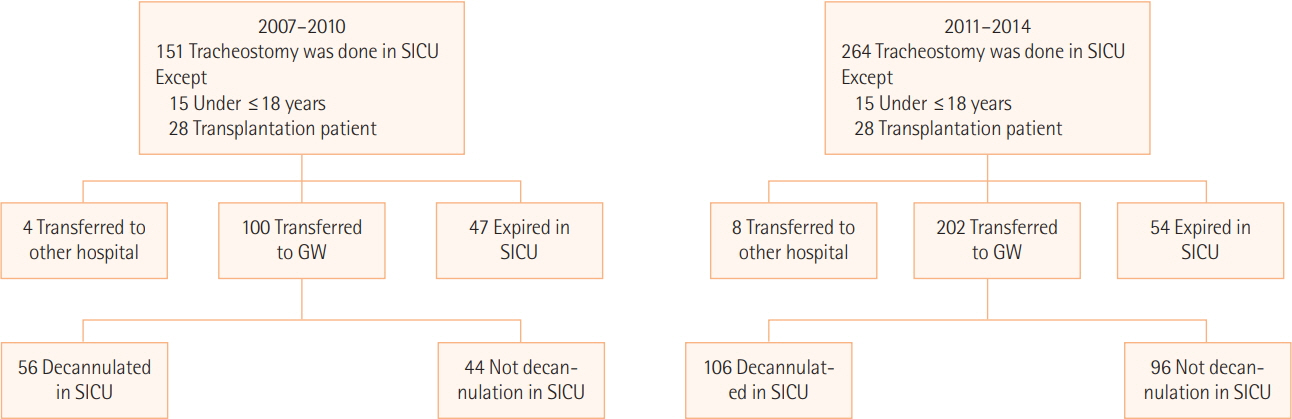
Figure 1. Flow diagram of preintervention and postintervention patient enrollment. SICU: surgical intensive care unit; GW: general ward.
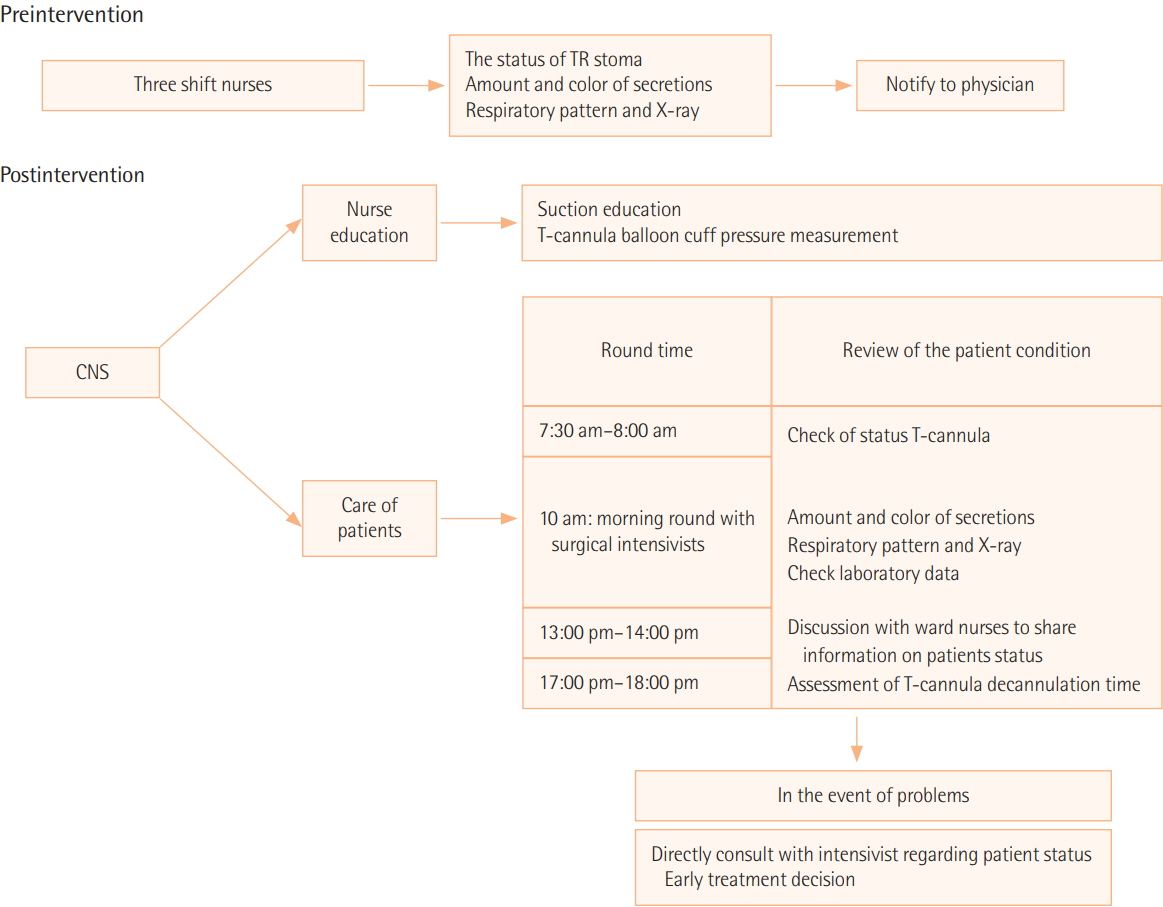
Figure 2. Comparison of pre- and postintervention tracheostomy care. TR: tracheostomy; CNS: clinical nurse specialist.
Reference
-
1. Casserly P, Lang E, Fenton JE, Walsh M. Assessment of healthcare professionals’ knowledge of managing emergency complications in patients with a tracheostomy. Br J Anaesth. 2007; 99:380–3.
Article2. Durbin CG Jr. Tracheostomy: why, when, and how? Respir Care. 2010; 55:1056–68.3. Cameron M, Corner A, Diba A, Hankins M. Development of a tracheostomy scoring system to guide airway management after major head and neck surgery. Int J Oral Maxillofac Surg. 2009; 38:846–9.
Article4. Stelfox HT, Crimi C, Berra L, Noto A, Schmidt U, Bigatello LM, et al. Determinants of tracheostomy decannulation: an international survey. Crit Care. 2008; 12:R26.
Article5. Engoren M, Arslanian-Engoren C, Fenn-Buderer N. Hospital and long-term outcome after tracheostomy for respiratory failure. Chest. 2004; 125:220–7.
Article6. Norwood MG, Spiers P, Bailiss J, Sayers RD. Evaluation of the role of a specialist tracheostomy service: from critical care to outreach and beyond. Postgrad Med J. 2004; 80:478–80.
Article7. Paul F. Tracheostomy care and management in general wards and community settings: literature review. Nurs Crit Care. 2010; 15:76–85.
Article8. Ball C. Ensuring a successful discharge from intensive care. Intensive Crit Care Nurs. 2005; 21:1–4.
Article9. Russell S. Continuity of care after discharge from ICU. Prof Nurse. 2000; 15:497–500.10. de Mestral C, Iqbal S, Fong N, LeBlanc J, Fata P, Razek T, et al. Impact of a specialized multidisciplinary tracheostomy team on tracheostomy care in critically ill patients. Can J Surg. 2011; 54:167–72.
Article11. Lewis T, Oliver G. Improving tracheostomy care for ward patients. Nurs Stand. 2005; 19:33–7.
Article12. Docherty B, Bench S. Tracheostomy management for patients in general ward settings. Prof Nurse. 2002; 18:100–4.13. Hooper M. Nursing care of the patient with a tracheostomy. Nurs Stand. 1996; 10:40–3.
Article14. Tamburri LM. Care of the patient with a tracheostomy. Orthop Nurs. 2000; 19:49–58.
Article15. Buglass E. Tracheostomy care: tracheal suctioning and humidification. Br J Nurs. 1999; 8:500–4.
Article16. Speed L, Harding KE. Tracheostomy teams reduce total tracheostomy time and increase speaking valve use: a systematic review and meta-analysis. J Crit Care. 2013; 28:216.e1-10.
Article17. Fernandez R, Bacelar N, Hernandez G, Tubau I, Baigorri F, Gili G, et al. Ward mortality in patients discharged from the ICU with tracheostomy may depend on patient’s vulnerability. Intensive Care Med. 2008; 34:1878–82.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Corrigendum: The Effect of Systematic Approach to Tracheostomy Care in Patients Transferred from the Surgical Intensive Care Unit to General Ward
- Concept Analysis of Relocation Stress: Focusing on Patients Transferred from Intensive Care Unit to General Ward
- Role Adaptation Processes of Family Caregivers with Patients Transferred from Intensive Care Unit to General Ward: Becoming almost a Nurse with Hope and Fear
- Is Percutaneous Dilatational Tracheostomy Safe to Perform in the Intensive Care Unit?
- Minimal Invasive Translaryngeal Tracheostomy after Open Heart Surgery
