Obstet Gynecol Sci.
2018 Jul;61(4):497-504. 10.5468/ogs.2018.61.4.497.
Clinical outcomes of frozen embryo transfer cycles after freeze-all policy to prevent ovarian hyperstimulation syndrome
- Affiliations
-
- 1Department of Obstetrics and Gynecology, Seoul National University College of Medicine, Seoul, Korea. blasto@snubh.org
- 2Department of Obstetrics and Gynecology, Kyung Hee University Hospital at Gangdong, Seoul, Korea.
- 3Department of Obstetrics and Gynecology, Seoul National University Hospital, Seoul, Korea.
- 4Department of Obstetrics and Gynecology, Seoul National University Bundang Hospital, Seongnam, Korea.
- KMID: 2439723
- DOI: http://doi.org/10.5468/ogs.2018.61.4.497
Abstract
OBJECTIVE
To compare the clinical pregnancy rate (CPR) and ongoing pregnancy rate (OPR) in frozen embryo transfers (FETs) following either freeze-all policy to prevent ovarian hyperstimulation syndrome (OHSS; freeze-all group) or excess embryo cryopreservation after fresh embryo transfer (surplus group).
METHODS
The freeze-all group comprised 44 FET cycles performed in 25 women between 2010 and 2016. The surplus group comprised 53 FET cycles performed in 47 women during the same period. The cumulative CPR and OPR according to duration of cryopreservation (interval between cryopreservation and FET) was estimated using Kaplan-Meier plots. Cox regression analysis was used for identifying factor to affect to cryopreservation duration in cycles with pregnancy.
RESULTS
In day 2-4 transfer cycles, the crude CPR (40% vs. 18.2%) and OPR (20% vs. 4.5%) were similar between the 2 groups. In day 5 transfer, the crude CPR (33.3% vs. 38.7%) and OPR (33.3% vs. 29%) were also similar between the 2 groups. The cumulative CPR (100% vs. 47.5%) and OPR (100% vs. 33.3%) in day 2-4 transfer as well as the cumulative CPR (46.7% vs. 100%) and OPR (46.7% and 74.8%) in day 5 transfer were also similar between the 2 groups. The median duration of cryopreservation was significantly shorter in the freeze-all group than in the surplus group (19.8 vs. 36.9 weeks, P=0.04). Previous history of delivery was the only factor associated with a shorter cryopreservation duration in cycles with pregnancy (hazard ratio, 0.18; 95% confidence interval, 0.05-0.65; P=0.01).
CONCLUSION
Freezing embryos to prevent OHSS and transferring the frozen embryos later may guarantee an acceptable reproductive outcome.
MeSH Terms
Figure
-
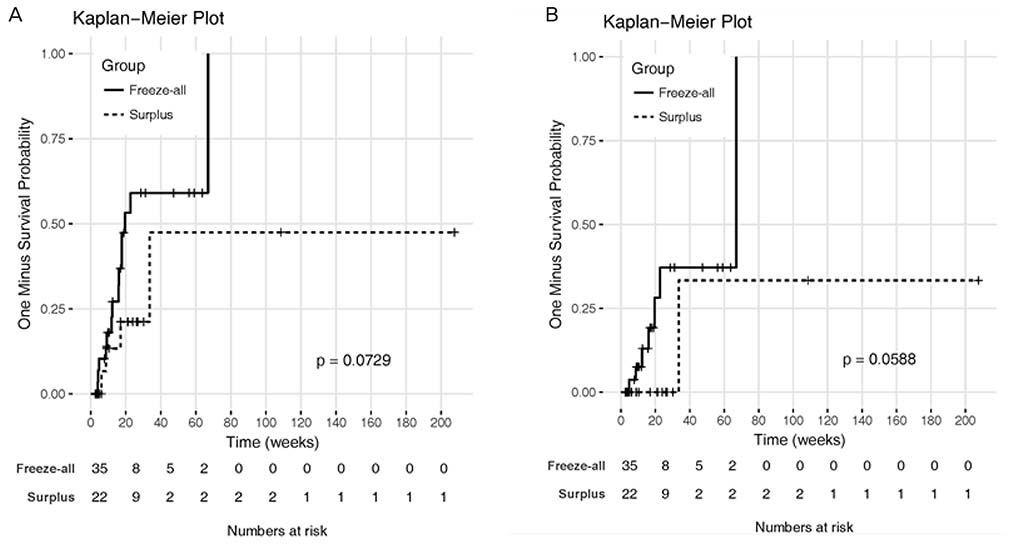
Fig. 1 Kaplan-Meier estimates of (A) cumulative clinical pregnancy rate and (B) cumulative ongoing pregnancy rate based on the interval between embryo freezing at day 2–4 and frozen embryo transfer.

Fig. 2 Kaplan-Meier estimates of (A) cumulative clinical pregnancy rate and (B) cumulative ongoing pregnancy rate based on the interval between embryo freezing at day 5 and frozen embryo transfer.
Reference
-
1. Trounson A, Mohr L. Human pregnancy following cryopreservation, thawing and transfer of an eight-cell embryo. Nature. 1983; 305:707–709.
Article2. Shapiro BS, Daneshmand ST, Garner FC, Aguirre M, Hudson C. Clinical rationale for cryopreservation of entire embryo cohorts in lieu of fresh transfer. Fertil Steril. 2014; 102:3–9.
Article3. Cobo A, de los Santos MJ, Castellò D, Gámiz P, Campos P, Remohí J. Outcomes of vitrified early cleavage-stage and blastocyst-stage embryos in a cryopreservation program: evaluation of 3,150 warming cycles. Fertil Steril. 2012; 98:1138–1146.e1.
Article4. Bedoschi G, Oktay K. Current approach to fertility preservation by embryo cryopreservation. Fertil Steril. 2013; 99:1496–1502.
Article5. Groothuis PG, Dassen HH, Romano A, Punyadeera C. Estrogen and the endometrium: lessons learned from gene expression profiling in rodents and human. Hum Reprod Update. 2007; 13:405–417.
Article6. Shapiro BS, Daneshmand ST, Garner FC, Aguirre M, Hudson C, Thomas S. High ongoing pregnancy rates after deferred transfer through bipronuclear oocyte cryopreservation and post-thaw extended culture. Fertil Steril. 2009; 92:1594–1599.
Article7. Royal College of Obstetricians and Gynaecologists. The Management of Ovarian Hyperstimulation Syndrome. Green-top Guideline No. 5. London: Royal College of Obstetricians and Gynaecologists;2016.8. Nastri CO, Ferriani RA, Rocha IA, Martins WP. Ovarian hyperstimulation syndrome: pathophysiology and prevention. J Assist Reprod Genet. 2010; 27:121–128.
Article9. Youssef MA, van Wely M, Hassan MA, Al-Inany HG, Mochtar M, Khattab S, et al. Can dopamine agonists reduce the incidence and severity of OHSS in IVF/ICSI treatment cycles? A systematic review and meta-analysis. Hum Reprod Update. 2010; 16:459–466.
Article10. Papanikolaou EG, Tournaye H, Verpoest W, Camus M, Vernaeve V, Van Steirteghem A, et al. Early and late ovarian hyperstimulation syndrome: early pregnancy outcome and profile. Hum Reprod. 2005; 20:636–641.
Article11. Amso NN, Ahuja KK, Morris N, Shaw RW. The management of predicted ovarian hyperstimulation involving gonadotropin-releasing hormone analog with elective cryopreservation of all pre-embryos. Fertil Steril. 1990; 53:1087–1090.
Article12. Salat-Baroux J, Alvarez S, Antoine JM, Cornet D, Tibi C, Plachot M, et al. Treatment of hyperstimulation during in-vitro fertilization. Hum Reprod. 1990; 5:36–39.
Article13. Wada I, Matson PL, Troup SA, Hughes S, Buck P, Lieberman BA. Outcome of treatment subsequent to the elective cryopreservation of all embryos from women at risk of the ovarian hyperstimulation syndrome. Hum Reprod. 1992; 7:962–966.
Article14. Wada I, Matson PL, Troup SA, Morroll DR, Hunt L, Lieberman BA. Does elective cryopreservation of all embryos from women at risk of ovarian hyperstimulation syndrome reduce the incidence of the condition? Br J Obstet Gynaecol. 1993; 100:265–269.
Article15. Ferraretti AP, Gianaroli L, Magli C, Fortini D, Selman HA, Feliciani E. Elective cryopreservation of all pronucleate embryos in women at risk of ovarian hyperstimulation syndrome: efficiency and safety. Hum Reprod. 1999; 14:1457–1460.
Article16. Horwath D, Check JH, Choe JK, Wilson C, Amui J. Frozen embryo transfer outcome according to reason for freezing the embryos. Clin Exp Obstet Gynecol. 2005; 32:19–20.
Article17. Aboulghar MA, Mansour RT, Serour GI, Ramzy AM, Amin YM. Oocyte quality in patients with severe ovarian hyperstimulation syndrome. Fertil Steril. 1997; 68:1017–1021.
Article18. Kasius A, Smit JG, Torrance HL, Eijkemans MJ, Mol BW, Opmeer BC, et al. Endometrial thickness and pregnancy rates after IVF: a systematic review and meta-analysis. Hum Reprod Update. 2014; 20:530–541.
Article19. Bland JM, Altman DG. Survival probabilities (the Kaplan-Meier method). BMJ. 1998; 317:1572.20. Kaplan EL, Meier P. Nonparametric estimation from incomplete observations. J Am Stat Assoc. 1958; 53:457–481.
Article21. Santos-Ribeiro S, Polyzos NP, Lan VT, Siffain J, Mackens S, Van Landuyt L, et al. The effect of an immediate frozen embryo transfer following a freeze-all protocol: a retrospective analysis from two centres. Hum Reprod. 2016; 31:2541–2548.
Article22. Giudice LC. Endometrium in PCOS: Implantation and predisposition to endocrine CA. Best Pract Res Clin Endocrinol Metab. 2006; 20:235–244.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of pregnancy and implantation rates in fresh embryo transfer (ET) and frozen-thawed ET cycles in infertile women with polycystic ovarian syndrome
- Clinical factors that affect the pregnancy rate in frozen-thawed embryo transfer in the freeze-all policy
- Effects of controlled ovarian stimulation regimens on top-quality blastocyst development and perinatal outcomes with the freeze-all strategy: A retrospective comparative study
- Spontaneous ovarian hyperstimulation syndrome following a thawed embryo transfer cycle
- Preliminary clinical outcome of novel strategy for the maximization of cumulative pregnancy rates per retrieval in normal responders
