J Periodontal Implant Sci.
2012 Dec;42(6):231-236.
Influence of crown-to-implant ratio on periimplant marginal bone loss in the posterior region: a five-year retrospective study
- Affiliations
-
- 1Department of Periodontology, Kyungpook National University School of Dentistry, Daegu, Korea. jysuh@knu.ac.kr
Abstract
- PURPOSE
The aim of this study was to evaluate the influence of the crown-to-implant (C/I) ratio on the change in marginal bone level around the implant and to determine the site-related factors influencing the relationship between the C/I ratio and periimplant marginal bone loss.
METHODS
A total of 259 implants from 175 patients were evaluated at a mean follow-up of five years. Implants were divided into two groups according to their C/I ratios: < or =1, and >1. Site-related factors having an influence on the relationship between C/I ratio and periimplant marginal bone loss were analyzed according to the implant location, implant diameter, implant manufacturer, prosthesis type, and guided bone regeneration (GBR) procedure.
RESULTS
It was found that 1) implants with a C/I ratio below 1 exhibited greater periimplant marginal bone loss than implants with a C/I ratio more than 1, 2) site-related factors had an effect on periimplant marginal bone loss, except for the implant system used, 3) the C/I ratio was the factor having more dominant influence on periimplant marginal bone loss, compared with implant diameter, prosthesis type, implant location, and GBR procedure, 4) implants with a C/I ratio below 1 showed greater periimplant marginal bone loss than implants with a C/I ratio greater than 1 in the maxilla, but not in the mandible, 5) and periimplant marginal bone loss was more affected by the implant system than the C/I ratio.
CONCLUSIONS
Within the limitations of this study, implants with a higher C/I ratio exhibited less marginal bone loss than implants with a lower C/I ratio in the posterior regions. The C/I ratio was a more dominant factor affecting periimplant marginal bone loss in the maxilla than the mandible. Meanwhile, the implant system was a more dominant factor influencing periimplant marginal bone loss than the C/I ratio.
MeSH Terms
Figure
-
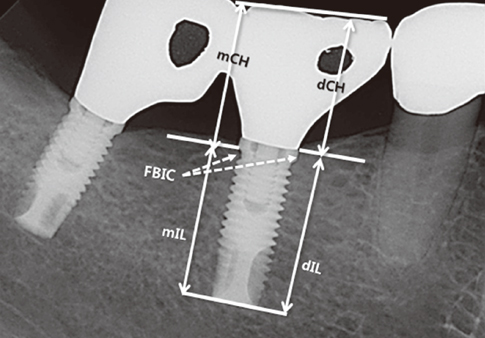
Figure 1 Formula for calculation of crown-to-implant (C/I) ratio. mCH/mIL: mesial C/I ratio, dCH/dIL: distal C/I ratio. An average mesiodistal C/I ratio was obtained per implant restoration. mCH: mesial clinical crown height, mIL: mesial implant length, dCH: distal clinical crown height, dIL: distal implant length, FBIC: the first bone-to-implant contact.
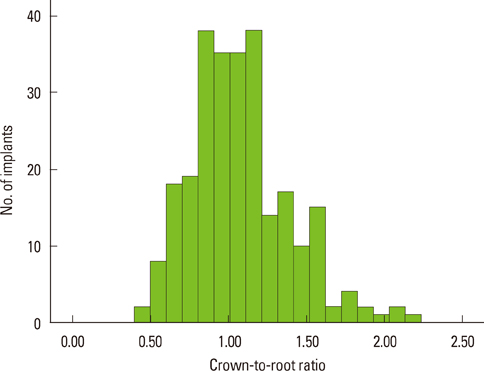
Figure 2 Distribution of the implants according to their crown-to-implant ratio.
Reference
-
1. Grossmann Y, Sadan A. The prosthodontic concept of crown-to-root ratio: a review of the literature. J Prosthet Dent. 2005. 93:559–562.
Article2. Dykema RW. Johnston JF, Dykema LW, Goodacre CJ, Phillips RW, editors. Diagnosis and Treatment Planning. Johnston's modern practice in fixed prosthodontics. 1986. 4th ed. Philadelphia: WB Saunders;8–21.3. Shillingburg HT Jr. Shillingburg HT, Hobo S, Whitsett LD, Jacobi R, Brackett SE, editors. Treatment Planning for the Replacement of Missing Teeth. Fundamentals of fixed prosthodontics. 1997. 3rd ed. Chicago: Quintessence Publishing;89–90.4. Nyman S, Ericsson I. The capacity of reduced periodontal tissues to support fixed bridgework. J Clin Periodontol. 1982. 9:409–414.
Article5. Laurell L, Lundgren D, Falk H, Hugoson A. Long-term prognosis of extensive polyunit cantilevered fixed partial dentures. J Prosthet Dent. 1991. 66:545–552.
Article6. Yi SW, Ericsson I, Carlsson GE, Wennström JL. Long-term follow-up of cross-arch fixed partial dentures in patients with advanced periodontal destruction. Evaluation of the supporting tissues. Acta Odontol Scand. 1995. 53:242–248.
Article7. Bidez MW, Misch CE. Misch CE, editor. Clinical Biomechanics in Implant Dentistry. Contemporary implant dentistry. 2008. St. Louis: Mosby Elsevier;543–555.
Article8. Brose MO, Avers RJ, Rieger MR, Duckworth JE. Submerged alumina dental root implants in humans: five-year evaluation. J Prosthet Dent. 1989. 61:594–601.
Article9. Nasr HF, Meffert RM. A proposed radiographic index for assessment of the current status of osseointegration. Int J Oral Maxillofac Implants. 1993. 8:323–328.10. Haas R, Mensdorff-Pouilly N, Mailath G, Watzek G. Brånemark single tooth implants: a preliminary report of 76 implants. J Prosthet Dent. 1995. 73:274–279.
Article11. Glantz PO, Nilner K. Biomechanical aspects of prosthetic implant-borne reconstructions. Periodontol 2000. 1998. 17:119–124.
Article12. Schulte J, Flores AM, Weed M. Crown-to-implant ratios of single tooth implant-supported restorations. J Prosthet Dent. 2007. 98:1–5.
Article13. Verhoeven JW, Cune MS, de Putter C. Reliability of some clinical parameters of evaluation in implant dentistry. J Oral Rehabil. 2000. 27:211–216.
Article14. Updegrave WJ. Right-angle dental radiography. Dent Clin North Am. 1968. 12:571–579.15. Urdaneta RA, Rodriguez S, McNeil DC, Weed M, Chuang SK. The effect of increased crown-to-implant ratio on single-tooth locking-taper implants. Int J Oral Maxillofac Implants. 2010. 25:729–743.16. Rangert BR, Sullivan RM, Jemt TM. Load factor control for implants in the posterior partially edentulous segment. Int J Oral Maxillofac Implants. 1997. 12:360–370.17. Pilliar RM, Cameron HU, Binnington AG, Szivek J, Macnab I. Bone ingrowth and stress shielding with a porous surface coated fracture fixation plate. J Biomed Mater Res. 1979. 13:799–810.
Article18. Rokni S, Todescan R, Watson P, Pharoah M, Adegbembo AO, Deporter D. An assessment of crown-to-root ratios with short sintered porous-surfaced implants supporting prostheses in partially edentulous patients. Int J Oral Maxillofac Implants. 2005. 20:69–76.19. Blanes RJ, Bernard JP, Blanes ZM, Belser UC. A 10-year prospective study of ITI dental implants placed in the posterior region. II: Influence of the crown-to-implant ratio and different prosthetic treatment modalities on crestal bone loss. Clin Oral Implants Res. 2007. 18:707–714.
Article20. Sekine H, Komiyama Y, Hotta H, Yoshida T. Van Steenberghe D, editor. Mobility Characteristics and Tactile Sensitivity of Osseointegrated Implant-Supporting Systems. Tissue integration in oral and maxillofacial reconstruction. 1986. Amsterdam: Excerpta Medica;326–339.21. Misch CE, Qu Z, Bidez MW. Mechanical properties of trabecular bone in the human mandible: implications for dental implant treatment planning and surgical placement. J Oral Maxillofac Surg. 1999. 57:700–706.
Article22. Akca K, Cehreli MC. Biomechanical consequences of progressive marginal bone loss around oral implants: a finite element stress analysis. Med Biol Eng Comput. 2006. 44:527–535.
Article23. Aalam AA, Nowzari H. Clinical evaluation of dental implants with surfaces roughened by anodic oxidation, dual acid-etched implants, and machined implants. Int J Oral Maxillofac Implants. 2005. 20:793–798.24. Abrahamsson I, Berglundh T. Effects of different implant surfaces and designs on marginal bone-level alterations: a review. Clin Oral Implants Res. 2009. 20:Suppl 4. 207–215.
Article25. Tawil G, Aboujaoude N, Younan R. Influence of prosthetic parameters on the survival and complication rates of short implants. Int J Oral Maxillofac Implants. 2006. 21:275–282.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Influence of crown-to-implant ratio of short vs long implants on implant stability and marginal bone loss in the mandibular single molar implant
- A Retrospective study on upper single tooth implants
- Radiographic evaluation of the proximal bone level between two implants: A 3-year comparative study between Branemark and ITI implants in the mandibular posterior region
- Retrospective study on marginal bone loss around maxillary anterior implants with or without bone graft
- Marginal bone level changes in association with different vertical implant positions: a 3-year retrospective study
