Early experiences of endovascular aneurysm repair for ruptured abdominal aortic aneurysms
- Affiliations
-
- 1Department of Surgery, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea. tslee@snubh.org
- 2Department of Surgery, The Catholic University of Korea School of Medicine, Seoul, Korea.
- KMID: 2438690
- DOI: http://doi.org/10.4174/astr.2019.96.3.138
Abstract
- PURPOSE
The use of endovascular aneurysm repair (EVAR) for ruptured abdominal aortic aneurysms (r-AAA) is steadily increasing. We report early experiences of EVAR for r-AAA performed in two tertiary referral centers in Korea.
METHODS
We retrospectively reviewed r-AAA patients treated by EVAR from May 2013 to December 2017. An EVAR-first strategy for r-AAA was adopted whenever feasible. The demographic information, anatomic characteristics, operative details, postoperative complications with special attention to abdominal compartment syndrome (ACS), and 30-day mortality were collected and analyzed.
RESULTS
We identified 13 patients who underwent EVAR for r-AAA. Mean age was 74.2 years and mean AAA size was 74.2 mm. Two patients underwent cardiopulmonary resuscitation at initial presentation. Bifurcated stent grafts were used in 12 out of 13 cases and physician-modified endografts with fenestrated/chimney techniques were performed in 2 cases with short neck. Successful stent graft deployment was achieved in all cases. Three patients were suspected of having ACS and 2 of them underwent laparotomy for decompression. The 30-day mortality was 7.7% (1 of 13), the only mortality being a patient that refused decompressive laparotomy for suspected ACS.
CONCLUSION
Despite the small numbers, the outcomes of EVAR for treatment of r-AAA were very promising, even in selected cases with unfavorable anatomy. These outcomes were achieved by a dedicated and well-trained team approach, and by use of high-end angiographic technology. Finally, ACS after EVAR is not uncommon, and requires a high index of suspicion as well as liberal use of decompressive surgery.
MeSH Terms
Figure
-
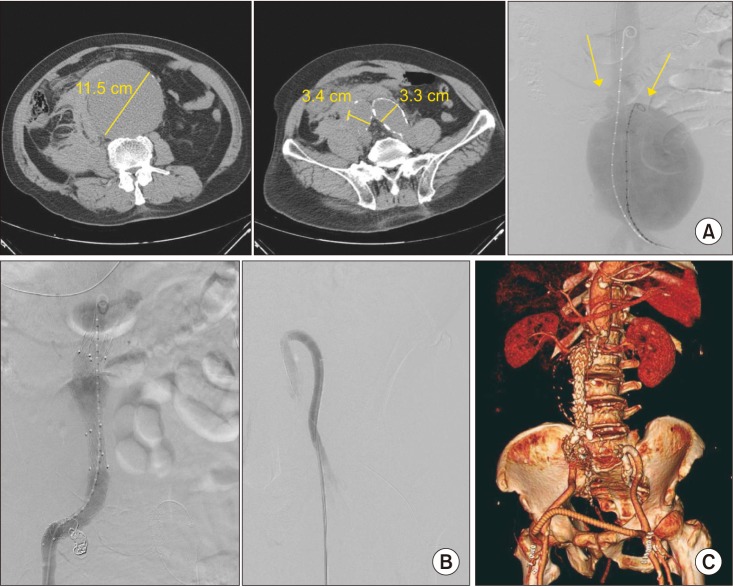
Fig. 1 (A) A case of ruptured 11.5 cm abdominal aortic aneurysm with concomitant bilateral common iliac and right internal iliac artery aneurysms. Initial angiography demonstrates a huge aneurysm with a relatively short aortic neck as shown by the location of both renal arteries (arrows). (B) The patient was treated with an aortouni-iliac device and crossover femorofemoral bypass, and an additional covered stent was inserted from the left external iliac artery into the left internal artery in a reversed U-shape configuration to allow for retrograde pelvic flow from the left femoral artery. (C) Follow-up CT reconstruction demonstrated a patent endograft with flow through the femoro-femoral graft into both the left internal iliac artery and the left lower extremity arterial system.
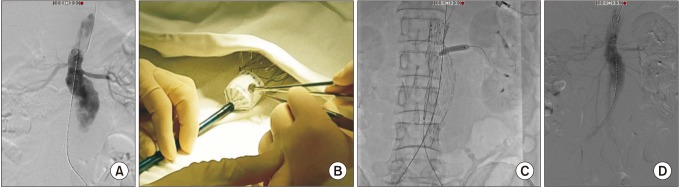
Fig. 2 (A) A case of advanced endovascular aneurysm repair for a ruptured 7.3-cm juxtarenal abdominal aortic aneurysm where the right renal artery was 15 mm below the left renal artery, as shown in the initial angiogram. (B) A single right renal fenestration was created in a bifurcated endograft, which was reinforced with a gold marker. (C) A self-expanding covered stent was deployed into the left renal artery after cannulation through the fenestration and post-dilated with a balloon. (D) Final angiogram showed good flow through both renal arteries with no evidence of endoleak.
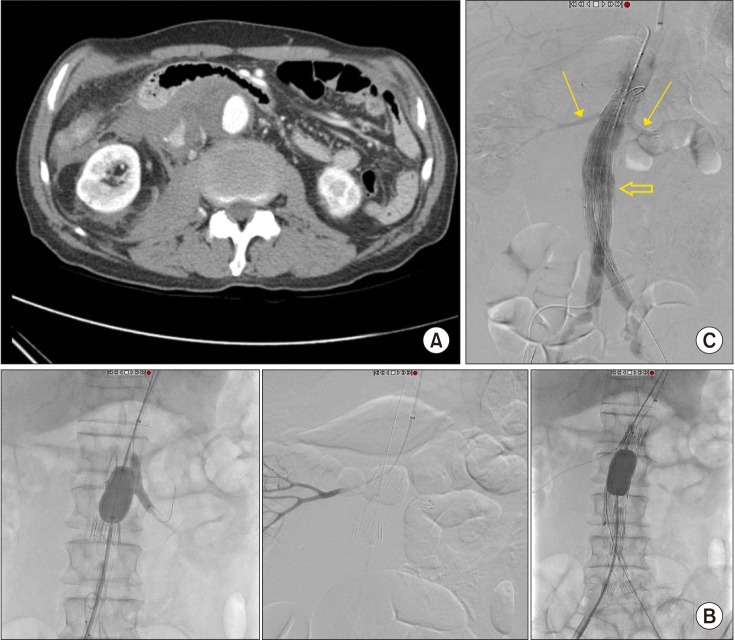
Fig. 3 (A) A case of advanced endovascular aneurysm repair for a ruptured 4.9-cm infrarenal abdominal aortic aneurysm with short neck (neck distance 9.4 mm from the right renal artery and 11.2 mm from the left renal artery). (B) A single renal fenestration was created on an extender endograft for the right renal artery and a chimney technique was performed for the left renal artery. The left chimney technique was performed successfully and the right renal artery was also successfully cannulated throught the endograft from a left brachial approach. However, after deployment of a bifurcated endograft with suprarenal fixation system, further insertion of a covered stent into the right renal artery was unsuccessful. (C) Despite failed cannulation through the fenestration into the right renal artery, flow through both renal arteries was preserved after endograft deployment (small arrows). Final angiogram showed a minor type Ia endoleak (or possibly III) which was observed (large arrow). Eventually the patient developed abdominal compartment syndrome and underwent explorative laparotomy with stent graft explantation and definitive surgery.
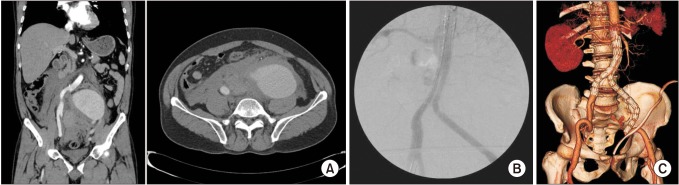
Fig. 4 (A) A case of a ruptured 10.7-cm left common iliac artery aneurysm treated by endovascular aneurysm repair (EVAR). (B) An EVAR procedure was performed with extension of the left limb graft to the external iliac artery. Final angiogram shows good exclusion of the aneurysm without evidence of endoleak. The patient developed abdominal compartment syndrome and therefore underwent emergent decompressive laparotomy with retroperitoneal hematoma evacuation and surgical ligation of the left internal artery. (C) Follow-up CT on postoperative day 14 demonstrates a patent graft without any evidence of endoleak.
Reference
-
1. Aggarwal S, Qamar A, Sharma V, Sharma A. Abdominal aortic aneurysm: a comprehensive review. Exp Clin Cardiol. 2011; 16:11–15. PMID: 21523201.2. Harris LM, Faggioli GL, Fiedler R, Curl GR, Ricotta JJ. Ruptured abdominal aortic aneurysms: factors affecting mortality rates. J Vasc Surg. 1991; 14:812–818. PMID: 1960812.
Article3. Reimerink JJ, Hoornweg LL, Vahl AC, Wisselink W, van den Broek TA, Legemate DA, et al. Endovascular repair versus open repair of ruptured abdominal aortic aneurysms: a multicenter randomized controlled trial. Ann Surg. 2013; 258:248–256. PMID: 23549424.
Article4. Desgranges P, Kobeiter H, Katsahian S, Bouffi M, Gouny P, Favre JP, et al. Editor’s Choice - ECAR (Endovasculaire ou Chirurgie dans les Anevrysmes aortoiliaques Rompus): a french randomized controlled trial of endovascular versus open surgical repair of ruptured aortoiliac aneurysms. Eur J Vasc Endovasc Surg. 2015; 50:303–310. PMID: 26001320.5. IMPROVE Trial Investigators. Powell JT, Sweeting MJ, Thompson MM, Ashleigh R, Bell R, et al. Endovascular or open repair strategy for ruptured abdominal aortic aneurysm: 30 day outcomes from IMPROVE randomised trial. BMJ. 2014; 348:f7661. PMID: 24418950.
Article6. Sweeting MJ, Balm R, Desgranges P, Ulug P, Powell JT. Ruptured Aneurysm Trialists. Individual-patient meta-analysis of three randomized trials comparing endovascular versus open repair for ruptured abdominal aortic aneurysm. Br J Surg. 2015; 102:1229–1239. PMID: 26104471.
Article7. IMPROVE Trial Investigators. Comparative clinical effectiveness and cost effectiveness of endovascular strategy v open repair for ruptured abdominal aortic aneurysm: three year results of the IMPROVE randomised trial. BMJ. 2017; 359:j4859. PMID: 29138135.8. Mureebe L, Egorova N, Giacovelli JK, Gelijns A, Kent KC, McKinsey JF. National trends in the repair of ruptured abdominal aortic aneurysms. J Vasc Surg. 2008; 48:1101–1107. PMID: 18771883.
Article9. Lesperance K, Andersen C, Singh N, Starnes B, Martin MJ. Expanding use of emergency endovascular repair for ruptured abdominal aortic aneurysms: disparities in outcomes from a nationwide perspective. J Vasc Surg. 2008; 47:1165–1170. discussion 1170-1. PMID: 18394857.
Article10. Kirkpatrick AW, Roberts DJ, De Waele J, Jaeschke R, Malbrain ML, De Keulenaer B, et al. Intra-abdominal hypertension and the abdominal compartment syndrome: updated consensus definitions and clinical practice guidelines from the World Society of the Abdominal Compartment Syndrome. Intensive Care Med. 2013; 39:1190–1206. PMID: 23673399.
Article11. Badger SA, Harkin DW, Blair PH, Ellis PK, Kee F, Forster R. Endovascular repair or open repair for ruptured abdominal aortic aneurysm: a Cochrane systematic review. BMJ Open. 2016; 6:e008391.
Article12. IMPROVE Trial Investigators. Endovascular strategy or open repair for ruptured abdominal aortic aneurysm: one-year outcomes from the IMPROVE randomized trial. Eur Heart J. 2015; 36:2061–2069. PMID: 25855369.13. Karkos CD, Menexes GC, Patelis N, Kalogirou TE, Giagtzidis IT, Harkin DW. A systematic review and meta-analysis of abdominal compartment syndrome after endovascular repair of ruptured abdominal aortic aneurysms. J Vasc Surg. 2014; 59:829–842. PMID: 24439324.
Article14. Acosta S, Lindblad B, Zdanowski Z. Predictors for outcome after open and endovascular repair of ruptured abdominal aortic aneurysms. Eur J Vasc Endovasc Surg. 2007; 33:277–284. PMID: 17097899.
Article15. Rubenstein C, Bietz G, Davenport DL, Winkler M, Endean ED. Abdominal compartment syndrome associated with endovascular and open repair of ruptured abdominal aortic aneurysms. J Vasc Surg. 2015; 61:648–654. PMID: 25499708.
Article16. Chen X, Zhao J, Huang B, Yuan D, Yang Y, Ma Y. Abdominal compartment syndrome after endovascular repair for ruptured abdominal aortic aneurysm leads to acute intestinal necrosis: Case report. Medicine (Baltimore). 2016; 95:e5316. PMID: 27893667.17. Powell JT, Sweeting MJ, Ulug P, Thompson MM, Hinchliffe RJ. IMPROVE Trial Investigators. Editor’s choice - re-interventions after repair of ruptured abdominal aortic aneurysm: a report from the IMPROVE randomised trial. Eur J Vasc Endovasc Surg. 2018; 55:625–632. PMID: 29503083.
Article18. Quinn AA, Mehta M, Teymouri MJ, Keenan ME, Paty PSK, Zhou Y, et al. The incidence and fate of endoleaks vary between ruptured and elective endovascular abdominal aortic aneurysm repair. J Vasc Surg. 2017; 65:1617–1624. PMID: 28268109.
Article19. Wong LA, Milner R. Interhospital Transfer of Ruptured AAA’s for EVAR: preposterous or prudent? Vasc Endovascular Surg. 2016; 50:455–457. PMID: 27488418.20. Mehta M, Taggert J, Darling RC 3rd, Chang BB, Kreienberg PB, Paty PS, et al. Establishing a protocol for endovascular treatment of ruptured abdominal aortic aneurysms: outcomes of a prospective analysis. J Vasc Surg. 2006; 44:1–8. discussion 8. PMID: 16828417.
Article21. Moore R, Nutley M, Cina CS, Motamedi M, Faris P, Abuznadah W. Improved survival after introduction of an emergency endovascular therapy protocol for ruptured abdominal aortic aneurysms. J Vasc Surg. 2007; 45:443–450. PMID: 17257800.
Article22. Budtz-Lilly J, Bjorck M, Venermo M, Debus S, Behrendt CA, Altreuther M, et al. Editor’s choice - the impact of centralisation and endovascular aneurysm repair on treatment of ruptured abdominal aortic aneurysms based on international registries. Eur J Vasc Endovasc Surg. 2018; 56:181–188. PMID: 29482972.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Complications and Their Management after Endovascular Aneurysm Repair for the Treatment of Abdominal Aortic Aneurysms
- General Considerations of Ruptured Abdominal Aortic Aneurysm: Ruptured Abdominal Aortic Aneurysm
- Endovascular Treatment of Abdominal Aortic Aneurysm
- Ruptured Abdominal Aortic Aneurysm with Antecedent Endovascular Repair of Abdominal Aortic Aneurysm
- Simultaneous Endovascular Aneurysm Repair for Abdominal Aortic Aneurysm Combined with Saccular Thoracic Aortic Aneurysm
