Principal Clinical Factors Predicting Therapeutic Outcomes After Surgical Drainage of Postoperative Cheek Cysts: Experience From a Single Center
- Affiliations
-
- 1Department of Otorhinolaryngology-Head and Neck Surgery, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea. hyunjerry@snu.ac.kr
- 2Department of Otorhinolaryngology-Head and Neck Surgery, Seoul National University Bundang Hospital, Seongnam, Korea.
- KMID: 2437495
- DOI: http://doi.org/10.21053/ceo.2018.00528
Abstract
OBJECTIVES
Postoperative cheek cyst (POCC) is a late postoperative complication of radical maxillary sinus surgery including the Caldwell-Luc (C-L) operation. The present study aimed to evaluate the therapeutic outcomes of surgical treatment for POCC and to assess the clinical factors correlated to these outcomes.
METHODS
This study included 57 patients (67 nostrils) diagnosed with POCC who underwent surgical drainage. The medical records of the patients were retrospectively reviewed for radiological findings, treatment modalities, residual symptoms, and recurrences.
RESULTS
In total, 30 patients were male and 27 patients were female with a mean age of 55 years, and the patients were usually diagnosed with POCC 28.2 years after radical surgery. Endonasal endoscopic marsupialization was performed via inferior meatal antrostomy, and if possible, middle meatal antrostomy was performed at the same time. In patients with cysts that were difficult to reach using an endonasal endoscopic approach, additional open C-L approaches were performed. The median follow-up period was 19.4 months. Overall, adequate drainage and symptomatic relief were achieved in 91% (61/67) of the patients. The recurrence rate was significantly higher in patients who had anterolateral POCC. Failure to achieve symptomatic relief was correlated to a smaller cyst and the use of the open C-L approach for drainage.
CONCLUSION
The location and size of the cyst as well as the use of the open surgical approach were important factors in predicting the therapeutic outcome of POCC. The time point of treatment and surgical approaches should be based on the above-mentioned findings.
Keyword
MeSH Terms
Figure
-
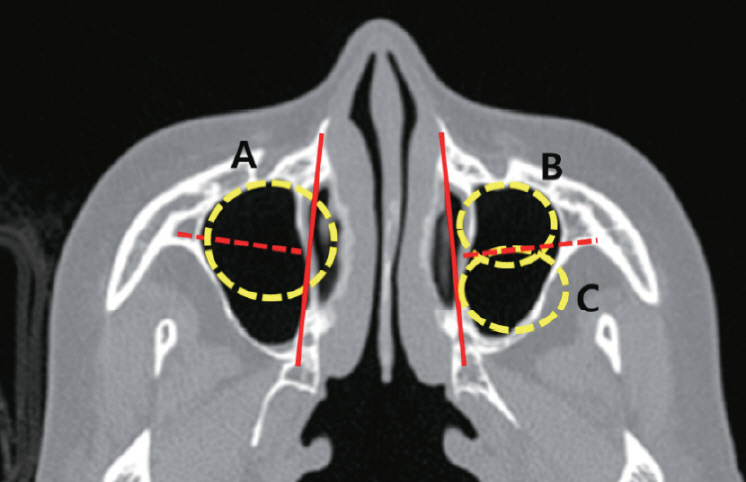
Fig. 1. Classification of postoperative cheek cysts. In the conventional system, a line is drawn between the anterior end of the inferior turbinate and base of the lateral pterygoid process (red lines). A medial cyst (A) extends toward the midline across this imaginary line, and a lateral cyst is classified as anterolateral (B) or posterolateral (C) based on the position of the center of the cyst with reference to another line (red dotted lines) that lies vertically to the initial line.

Fig. 2. Modified classification of postoperative cheek cysts. Line is drawn between the anterior end of the inferior turbinate and base of the lateral pterygoid process (red line). We modified the system such that an anterior cyst was defined as the posterior end of the cyst wall is located anterior to the midline (red dotted line). In cases where the posterior wall of the cyst is posterior to the midline, the cyst is classified as non-anterolateral.

Fig. 3. Case of multiple cysts. Cysts separated by bony or membranous septations (black arrows) were considered as multiple cysts.

Fig. 4. Initial presenting symptoms of postoperative cheek cysts. Cheek pain and swelling were the primary symptoms, followed by dental symptoms, orbital pain, nasal obstruction, and headache. The categories herein are not mutually exclusive.

Fig. 5. Kaplan-Meier probability curves for the risk of cyst recurrence. According to the location of the cyst, the recurrence rates were significantly different (log-rank test, P-value<0.001).
Reference
-
1. Kaneshiro S, Nakajima T, Yoshikawa Y, Iwasaki H, Tokiwa N. The postoperative maxillary cyst: report of 71 cases. J Oral Surg. 1981; Mar. 39(3):191–8.2. Yamamoto H, Takagi M. Clinicopathologic study of the postoperative maxillary cyst. Oral Surg Oral Med Oral Pathol. 1986; Nov. 62(5):544–8.
Article3. Nishioka M, Pittella F, Hamagaki M, Okada N, Takagi M. Prevalence of postoperative maxillary cyst significantly higher in Japan. Oral Med Pathol. 2005; 10(1):9–13.
Article4. Lee KC, Lee NH. Comparison of clinical characteristics between primary and secondary paranasal mucoceles. Yonsei Med J. 2010; Sep. 51(5):735–9.
Article5. Macbeth R. Caldwell, Luc, and their operation. Laryngoscope. 1971; Oct. 81(10):1652–7.
Article6. Kubo I. A buccal cyst occurring after a radical operation of the maxillary sinus. Z Otol Tokyo. 1927; 33:896–7.7. Jang TY, Lee SJ, Kim KT, Choi YS. Management of postoperative mucocele of the maxillary sinus through endoscopic approach. Korean J Otorhinolaryngol Head Neck Surg. 2005; Mar. 48(3):314–9.8. Kwon SH, Yang YS, Min YG. Surgical treatment and clinical study of postoperative maxillary cyst. Korean J Otorhinolaryngol Head Neck Surg. 1997; Aug. 40(8):1115–21.9. Yoshikawa Y, Nakajima T, Kaneshiro S, Sakaguchi M. Effective treatment of the postoperative maxillary cyst by marsupialization. J Oral Maxillofac Surg. 1982; Aug. 40(8):487–91.
Article10. Busaba NY, Salman SD. Maxillary sinus mucoceles: clinical presentation and long-term results of endoscopic surgical treatment. Laryngoscope. 1999; Sep. 109(9):1446–9.
Article11. Huang CC, Chen CW, Lee TJ, Chang PH, Chen YW, Chen YL, et al. Transnasal endoscopic marsupialization of postoperative maxillary mucoceles: middle meatal antrostomy versus inferior meatal antrostomy. Eur Arch Otorhinolaryngol. 2011; Nov. 268(11):1583–7.
Article12. Saito T, Ikeda T, Kono Y, Ohtsubo T, Noda I, Saito H. Implications of endoscopic endonasal surgery for the treatment of postoperative maxillary mucoceles. ORL J Otorhinolaryngol Relat Spec. 2000; Jan-Feb. 62(1):43–8.
Article13. Sawatsubashi M, Murakami D, Oda M, Komune S. Transnasal endoscopic surgery of post-operative maxillary cysts. J Laryngol Otol. 2015; Mar. 129 Suppl 2:S46–51.14. Nakamura K, Kitani S, Sato H, Yumoto E, Kawakita S, Aibara R. Endoscopic endonasal surgery for postoperative maxillary cyst. Nihon Jibiinkoka Gakkai Kaiho. 1995; Jun. 98(6):984–8.
Article15. Lund VJ. Fundamental considerations of the design and function of intranasal antrostomies. Rhinology. 1985; Sep. 23(3):231–6.16. Low WK. Complications of the Caldwell-Luc operation and how to avoid them. Aust N Z J Surg. 1995; Aug. 65(8):582–4.
Article17. Robinson SR, Baird R, Le T, Wormald PJ. The incidence of complications after canine fossa puncture performed during endoscopic sinus surgery. Am J Rhinol. 2005; Mar-Apr. 19(2):203–6.
Article18. Thompson LD. Paranasal sinus mucocele. Ear Nose Throat J. 2012; Jul. 91(7):276–8.
Article19. Abdel-Aziz M, El-Hoshy H, Azooz K, Naguib N, Hussein A. Maxillary sinus mucocele: predisposing factors, clinical presentations, and treatment. Oral Maxillofac Surg. 2017; Mar. 21(1):55–8.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Two Cases of Postoperative Cheek Cyst with Exophthalmos
- A Case of Infraorbital Protrusion of Postoperative Cheek Cyst
- Comparison of Outcomes and Recurrence in Chronic Subdural Hematoma Patients Treated by Burr-Hole Drainage with or without Irrigation
- Factors affecting complications after treatment of epidermal cyst
- Bilateral postoperative maxillary cysts after orthognathic surgery: A case report
